


Case Report - (2022) Volume 7, Issue 1
T inversion myocardial infarction, non-obstructive coronary arteries and repeated chest stress and chest pain in a 64 year-old-woman.
Received Date: Dec 03, 2021 / Accepted Date: Dec 10, 2021 / Published Date: Jan 22, 2022
Copyright: ©Wei Liang, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Citation: Tongjun Liu., Jieling Hu., Wei Liang. (2022). T inversion myocardial infarction, non-obstructive coronary arteries and repeated chest stress and chest pain in a 64 year-old-woman. Adv Nutr Food Sci, 7(1), 88-93.
Abstract
Myocardial infarction with non-obstructive coronary arteries (MINOCA), usually affect old women. It differs from infarction with obstructive coronary arteries in that it is not frequently associated with hypertension, hyperlipidemia or diabetes. We present a case of MINOCA where electrocardiogram (ECG) acted as a parameter of evaluation of the severity of the condition. A 64-year-old woman presented with the symptoms of acute myocardial infarction. ECG showed T wave changes (T ii, iii, avF, V4-V6 inversion). Cardiac magnetic resonance (CMR) imaging confirmed the presence of myocardial ischemia of the inferior ventricular wall. T wave returned to normal on ECG examination after 1 month of follow up after a series of treatments.
Keywords
MINOCA, Non-ST Elevation Myocardial Infarction, Women
Background
MINOCA is defined by as a less than 50% stenosis of all major epicardial vessels and accounts for of 6-8% of myocardial infarc¬tions [1, 2]. Studies have shown that patients with MINOCA are mostly young females with a low incidence of hypertension, hy¬perlipidemia and diabetes [3-6]. We present a case where ECG was used as a parameter for evaluating the severity of MINOCA.
Case Presentation
A 64-year-old female patient with a history of grade-I hyperten-sion dating since half a year without hyperlipemia, presented to the emergency department with a sudden onset of repeated chest distress, dyspnea, shortness of breath, and chest pain. These man¬ifestations were accompanied by sweating. Medical history of lower lung lobectomy, hysterectomy and benign nodectomy of the breast was reported. Her symptoms deteriorated and were not well controlled by Musk Baoxin pills prior to admission. Clinical ex¬amination was unremarkable.
Investigations
ECG showed a first-degree atrioventricular block and T wave changes (T â?±, â?², avF, V4-V6 inversion) (figure 1). Evaluation of cardiac enzymes revealed elevated levels of hypersensitive tro-ponin I (48.4pg/mL) and pro-BNP (413.1pg/mL). Chest thin-sec-tion CT scan showed multiple small nodules in both lungs, a few cords in the lower lobes of both lungs slightly thickened pleura on both sides, and calcified aortic wall. Cardiac ultrasound (UCG) showed aortic widening with 39 mm inner diameter, mild aortic insufficiency and 62% left ventricular ejection fraction (LVEF). Coronary Angiography with CT (CTA) showed no obvious ab¬normalities in major coronary vessels, and no calcification or soft plaque formation was found. CMR showed that there was plaque enhancement at 12 o ‘clock at the base of the left ventricular short axis with cardiac edema suggested by T2W at this point( figure 2. Resting myocardial perfusion imaging revealed mild ischemic changes in the apex (figure 3).
Based on the above examination and clinical presentation, we made the diagnosis of myocardial infarct with non-obstructive cor¬onary arteries. We offered pharmacotherapy in order to reduce the blood lipid level and platelet. During the treatment, we continued to monitor cardiac enzymes (figure 4) and electrocardiogram (fig¬ures 5, 6.1, 6.2, 7, 8) dynamically. She was discharged with normal a heart rate and normal levels of cardiac enzymes.

Figure 1: Admission ECG on May 27
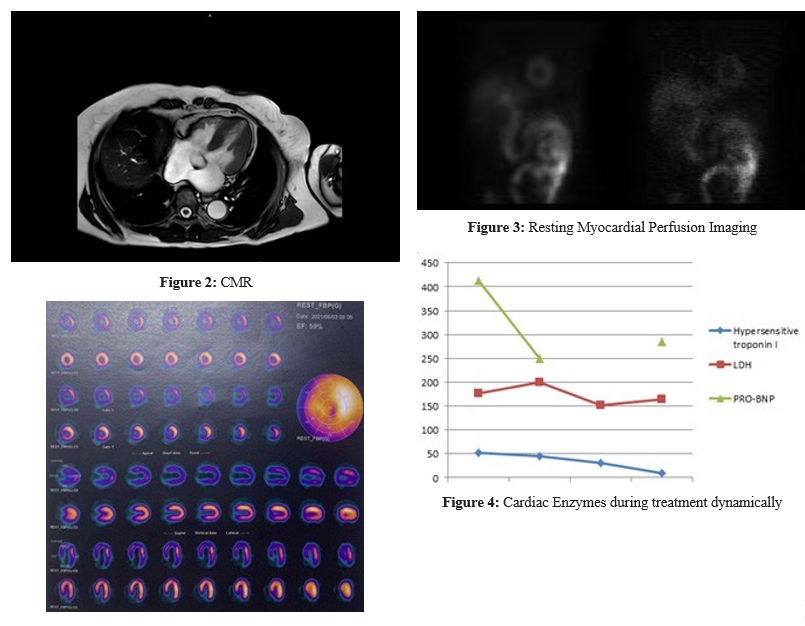

Figure 5: ECG on May 28
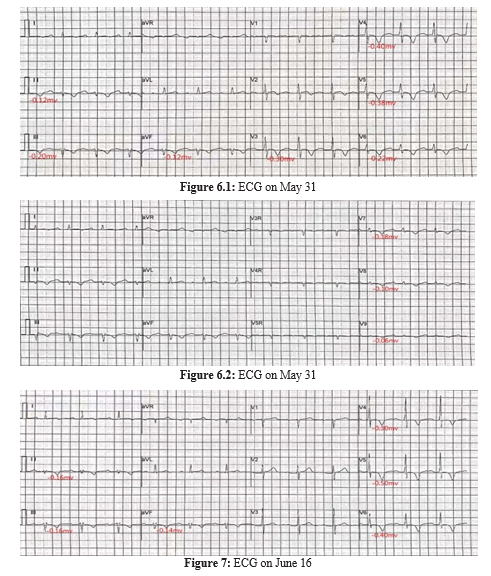

Figure 8: ECG on July 2
Outcome And Follow-Up
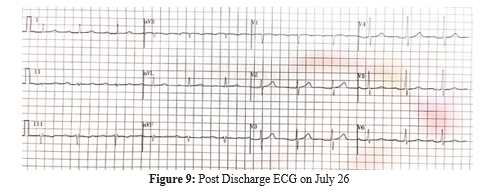
Pharmacotherapy included Plavix, Lipitor and Betallow regularly for 2 months. No significant cardiovascular symptoms were noted during subsequent outpatient appointments. T wave returned to normal appearance on ECG examination after 1 month of follow up (figure 9).
Discussion
MINOCA refers to acute myocardial infarction with non-obstruc-tive coronary arteries on angiography. With the advance of med-ical technology, MINOCA has been widely reported around the world with 5%-7% global prevalence [1]. Studies have shown that there may be racial differences in the incidence of MINOCA, since the incidence of MINOCA is higher among black people [2]. Al-though MINOCA can occur in all ages and genders, it is reported that the majority of patients are older women, with a median age of 55, with a worse overall prognosis and higher mortality in women than in men [1]. Compared with patients with myocardial infarc¬tion related to obstructive coronary artery disease, patients with MINOCA tend to be younger and are less likely to be complicated with hypertension, hyperlipidemia and diabetes and are more like¬ly to present with non-ST-segment elevation myocardial infarction [3-5].
In the acute phase of MINOCA, patients present with myocardial infarction due to acute myocardial ischemia. The main symptoms are chest pain and tachypnea, which makes the differentiation between MINOCA and acute coronary syndrome (ACS) of ath¬erosclerosis challenging. In addition to the similarity in clinical symptoms, the biomarkers and echocardiography results are very similar. ECG alone is not enough to distinguish MINOCA from atherosclerotic ACS during the acute phase of the disease, although non-ST-segment elevation myocardial infarction is usually present [5]. Daily ECG examination and monitoring of ECG evolution are significant for patient risk stratification. Coronary angiography (CAG) may be the first step to diagnose MINOCA and evaluate the patient’s condition, which is characterized by the absence of obstructive lesions in epicardial vessels [5]. For follow-up exam¬ination, the AHA recommends cardiac magnetic resonance imag¬ing (CMRI), which can confirm the clinical diagnosis of MINOCA after the exclusion of myocarditis, primary cardiomyopathy and other diseases. For the determination of the pathogenesis of MI-NOCA patients, some studies recommend coronary optical coher¬ence tomography (OCT) and cardiac magnetic resonance (CMR) [6]. OCT and CMR imaging identified the underlying mechanism in 84.5% of women with MINOCA, 75.5% of whom were isch¬emic and 24.5% of whom were non-ischemic.
Considered as a heterogeneous disease, MINOCA has different pathological mechanisms, which mainly include epicardial coro¬nary vasospasm and spontaneous coronary artery dissection cor¬onary embolism or thrombosis, coronary microvascular dysfunc¬tion, takotsubo cardiomyopathy and myocarditis [7-14]. Among them, coronary microvascular dysfunction is one of the most recognized causes. The diagnosis of MINOCA is often difficult because its clinical phenotype, such as symptoms, ECG, and bio-markers, may be similar to acute myocardial infarction. The diag¬nostic criteria for MINOCA proposed by the AHA in 2019 [1] are:
1. Acute myocardial infarction. Detection of a rise or fall of cTn with at least 1 value above the 99th percentile upper refer¬ence limit and corroborative clinical evidence of infarction evidenced by at least 1 of the following: a) Symptoms of myocardial ischemia; b)New ischemic electrocardiographic changes; c)Development of pathological Q waves; d)Imaging evidence of new loss of viable myocardium or new regional wall motion abnormality in a pattern consistent with an isch¬emic cause; e)Identification of a coronary thrombus by angi¬ography or autopsy.
2. Non-obstructive coronary arteries on angiography: defined as the absence of obstructive disease on angiography (i.e., no coronary artery stenosis ≥50%) in any major epicardial vessel. This includes patients with: a) Normal coronary arteries (no angiographic stenosis); b) Mild luminal irregularities (angio¬graphic stenosis <30% stenoses); c) Moderate coronary ath¬erosclerotic lesions (stenoses >30% but <50%).
3. No specific alternate diagnosis for the clinical presentation: alternate diagnoses include but are not limited to nonischemic causes such as sepsis, pulmonary embolism, and myocarditis. Up to now, there are no guidelines for the treatment of MINO¬CA, because there are no prospective randomized controlled clinical trials in this population. Existing treatment strategies are mainly based on clinical experience and expert consen¬sus, and individualized treatment for the etiology is required, and the prognosis also depends on the specific etiology [11]. The treatment of MINOCA mainly includes emergency sup¬portive treatment, myocardial protection and individualized treatment for the etiology. Emergency supportive treatment is mainly for the rapid management of malignant arrhythmias and cardiogenic shock. Many clinical studies have shown that cardio-protective drugs (such as dual antiplatelet, statins, ACEI/ARB and β -blockers) are recommended as a second-ary prevention therapy for MINOCA patients. The specific drug selection depends on the specific etiology of the patient. For example, β -blockers are contraindicated in patients with coronary vasospasm. Studies have shown that treatment with statins or ACEI/ARB has a long-term gain effect on patients’ prognosis, β -blockers have a positive effect, and dual anti¬platelet has a neutral effect [3, 15, 16]. The key point in the management MINOCA is to diagnose the underlying individ¬ual mechanisms in order to achieved tailored managing strat¬egies specific for each case [5, 10]. The major limitations of this case report was that the patient refused to undergo CAG, and the imaging manifestations of blood perfusion insufficien¬cy of small branches of coronary arteries were not left and the specific cause of myocardial ischemia of the patient was not found.
References
- Pasupathy, Sivabaskari, et al. “Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries.” Circulation 131.10 (2015): 861-870.
- Smilowitz, N. R., Mahajan, A. M., Roe, M. T., Hellkamp, A. S., Chiswell, K., Gulati, M., & Reynolds, H. R. (2017). Mortality of myocardial infarction by sex, age, and obstructive coronary artery disease status in the ACTION Registry–GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry–Get With the Guidelines). Circulation: Cardiovascular Quality and Outcomes, 10(12), e003443.
- Lindahl, B., Baron, T., Erlinge, D., Hadziosmanovic, N., Nordenskjöld, A., Gard, A., & Jernberg, T. (2017). Medical therapy for secondary prevention and long-term outcome in patients with myocardial infarction with nonobstructive coronary artery disease. Circulation, 135(16), 1481-1489.
- Basmah, S., Erica, S. S., Rachel, P. D., John, F. B., Judith, H. L., John, A. S., ... & Gail, D. O. (2018). Presentation, Clinical Profile, and Prognosis of Young Patients With Myocardial Infarction With Nonobstructive Coronary Arteries (MINOCA): Results From the VIRGO Study. Journal of the American Heart Association, 7(13), e009174.
- Tamis-Holland, J. E., Jneid, H., Reynolds, H. R., Agewall, S., Brilakis, E. S., Brown, T. M., ... & American Heart Association Interventional Cardiovascular Care Committee of the Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Epidemiology and Prevention; and Council on Quality of Care and Outcomes Research. (2019). Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: a scientific statement from the American Heart Association. Circulation, 139(18), e891-e908.
- Reynolds, H. R., Maehara, A., Kwong, R. Y., Sedlak, T., Saw,J., Smilowitz, N. R., ... & Hochman, J. S. (2021). Coronary optical coherence tomography and Cardiac magnetic resonance imaging to determine underlying causes of myocardial infarction with nonobstructive Coronary arteries in women. Circulation, 143(7), 624-640.
- Montone, R. A., Niccoli, G., Russo, M., Giaccari, M., Del Buono, M. G., Meucci, M. C., ... & Crea, F. (2020). Clinical, angiographic and echocardiographic correlates of epicardial and microvascular spasm in patients with myocardial ischaemia and non-obstructive coronary arteries. Clinical Research in Cardiology, 109(4), 435-443.
- Pirozzolo, G., Seitz, A., Athanasiadis, A., Bekeredjian, R., Sechtem, U., & Ong, P. (2020). Microvascular spasm in non-ST-segment elevation myocardial infarction without culprit lesion (MINOCA). Clinical Research in Cardiology, 109(2), 246-254.
- Da Costa, A., Isaaz, K., Faure, E., Mourot, S., Cerisier, A., & Lamaud, M. (2001). Clinical characteristics, aetiological factors and long-term prognosis of myocardial infarction with an absolutely normal coronary angiogram; a 3-year follow-up study of 91 patients. European heart journal, 22(16), 1459-1465.
- Cheema, A.N., et al., Myocardial infarction with nonobstructive coronary artery disease (MINOCA): a review of patho-physiology and management. (1531-7080 (Electronic)).
- S Scalone, G., Niccoli, G., & Crea, F. (2019). Editor’s Choice-Pathophysiology, diagnosis and management of MINOCA: an update. European Heart Journal: Acute Cardiovascular Care, 8(1), 54-62.
- Ong, P., Camici, P. G., Beltrame, J. F., Crea, F., Shimokawa, H., Sechtem, U., ... & Coronary Vasomotion Disorders International Study Group. (2018). International standardization of diagnostic criteria for microvascular angina. International journal of cardiology, 250, 16-20.
- Prasad, A., Lerman, A., & Rihal, C. S. (2008). Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. American heart journal, 155(3), 408-417.
- Tornvall, P., Gerbaud, E., Behaghel, A., Chopard, R., Collste, O., Laraudogoitia, E., ... & Agewall, S. (2015). Myocarditis or “true” infarction by cardiac magnetic resonance in patients with a clinical diagnosis of myocardial infarction without ob-structive coronary disease: a meta-analysis of individual patient data. Atherosclerosis, 241(1), 87-91.
- Choo, E. H., Chang, K., Lee, K. Y., Lee, D., Kim, J. G., Ahn,Y., ... & KAMIRâ?NIH Investigators. (2019). Prognosis and predictors of mortality in patients suffering myocardial infarction with nonâ?obstructive coronary arteries. Journal of the American Heart Association, 8(14), e011990.
- Nordenskjöld, A.M., et al., Randomized evaluation of beta blocker and ACE-inhibitor/angiotensin receptor blocker treatment in patients with myocardial infarction with non-obstruc-tive coronary arteries (MINOCA-BAT): Rationale and design. (1097-6744 (Electronic)).