
Journal of Research and Education(JRE)
ISSN: 2996-2544 | DOI: 10.33140/JRE


Review Article - (2025) Volume 3, Issue 1
Role of Clinical Pharmacists in Reducing Antimicrobial Resistance: Systematic Review
Received Date: Jan 21, 2025 / Accepted Date: Feb 25, 2025 / Published Date: Feb 28, 2025
Copyright: ©©2025 Birbirsa Sefera. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Sefera, B. (2025). Role of Clinical Pharmacists in Reducing Antimicrobial Resistance: Systematic Review. J Res Edu, 3(1), 01-07.
Abstract
Background: Antimicrobial resistance is a global health challenge, and the world is more vulnerable to the adverse health impacts of antimicrobial resistance. Healthcare workers, including pharmacists, can play a key role in reducing antimicrobial resistance. There is little study done on the role of clinical pharmacy in reducing antimicrobial resistance, particularly in Ethiopia.
Objective: The aim of this review is to investigate the role of clinical pharmacists in reducing antimicrobial resistance.
Method: The databases MEDLINE, EMBASE, PUBMED, and Google Scholar were searched for articles published between 1999 and 2019 that involved studies on the role of clinical pharmacists and the expanded services of clinical pharmacists in the healthcare system and their contributions to antimicrobial use. PRISMA-2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) was used to conduct this review.
Results: Studies from different countries have demonstrated that the roles of clinical pharmacists in health care teams result in overall improved clinical and economic outcomes.
Conclusions: This review highlights that integration of clinical pharmacist services into healthcare systems will assist in reducing the growth of catastrophic antimicrobial resistance.
Keywords
Antibiotics, Antimicrobial Resistance, Antimicrobial Stewardship Program, Clinical Pharmacists.
Abbreviations
CP: Clinical Pharmacist
AMR: Antimicrobial Resistance
WHO: World Health Organization
IPA: International Pharmaceutical Abstracts
Introduction
Antimicrobial Resistance (AMR) is defined as the resistance of bacterial, viral, parasitic, and fungal microorganisms to antimicrobial medicines that were previously effective for the treatment of infectious diseases. It occurs when bacteria, viruses, and other microorganisms change in ways that cause existing medications (e.g. antibiotics for bacterial infections and antivirals for viral infections) to be ineffective [1]. Infections caused by antibiotic-resistant microorganisms are associated with high morbidity, mortality, and healthcare costs; AMR annually causes 23,000 deaths in America, 25,000 deaths in the European Union, and 700,000 deaths worldwide. By 2050, it is predicted that there will be 10 million deaths annually and US$100 trillion in global economic loss caused by drug-resistant bacterial infections if AMR continues to rise at the same pace as in the last decades. Overprescribing and inappropriate prescribing of antibiotics are the principal and modifiable drivers of AMR [2].
Antimicrobial resistance is a serious global health challenge that impacts all countries and all people, regardless of their wealth or status. It is predicted that by 2050, there will be more than ten million deaths per year attributed to AMR. Further, it is predicted that the greatest number of these deaths will be in developing countries. Therefore, there is an urgent need to act to minimize the emergence of antimicrobial resistant bacteria in developing countries. The management of the development and spread of AMR requires a multifaceted approach, including the participation of all healthcare workers. According to the first objective of the World Health Organization (WHO) global action plan on AMR, avoiding overuse and misuse of antibiotics requires healthcare professionals' awareness and understanding of AMR with effective communication, education, and training. In this context, a clinical pharmacist is a key member of the antimicrobial multidisciplinary team involved in patients' pharmacotherapy monitoring. Pharmacists are important members of the healthcare team and they play a major role in medicine use and the provision of advice regarding appropriate medicine use. Education and training of pharmacists has the potential to influence the behavior of healthcare team members and consumers as part of a multidimensional strategy for changing practice and ensuring the quality use of antibiotics [3]. Representative data on the extent of the problem in low and middle-income countries is relatively scarce, but high levels of resistance are increasingly being reported worldwide. Antibiotic stewardship, that is, interventions designed to optimize the use of antibiotics, is therefore one of the key actions of the World Health Organization (WHO) Global Action Plan to contain antibiotic resistance [4]. Although the role of multidisciplinary has been done in different countries to reduce AMR so far, there is no evidence that shows the role of clinical pharmacists alone in combating AMR. Therefore, the aim of this review is to investigate the role of clinical pharmacists in reducing antimicrobial resistance in hospital and community settings.
Methodology
Literature Search Strategy
A literature search was conducted to identify articles published between 1999 and 2019 that involved studies on antimicrobial use or AMR involving clinical pharmacists in hospital and community settings using databases such as MEDLINE, EMBASE, PUBMED, and Google Scholar. The following ‘Medical Subject Headings’ (MeSH) terms were used to search articles: (Antimicrobial agents or antibiotics) OR (Drug Resistance, Bacterial or Antimicrobial resistance) AND (clinical pharmacy or pharmacies) OR (community pharmacy services) OR (professional role/ or pharmacy service, hospital/or pharmacy/or pharmacists/or pharmacy practice.) OR (clinical pharmacy) AND (community pharmacist OR clinical pharmacist OR pharmaceutical care) AND (antimicrobial resistance or antibiotic cost).
Google Scholar was also used to search for articles with the ap-propriate keywords. The following search terms: Antibiotic stew¬ardship, antimicrobial prescribing, clinical pharmacy, antibiotic consumption, physician’s perception, clinical pharmacy, antimi¬crobial utilization, infectious disease; pharmacist intervention, an¬timicrobial stewardship, guideline adherence, pharmacist, urgent care, antibiotic, antimicrobials, intravenous, therapy-switch, phar¬macist, clinical pharmacy, medication error, internal ward, cost, pharmacists, outcomes, interventions, multidisciplinary, hospital, antibiotic optimization, and antibiotic control programmers. The search words were used in different combinations. Cross-referenc-es of articles identified using these databases were also searched.
Eligibility Criteria
The Inclusion Criteria Were as Follows:
• Papers reporting descriptive accounts and papers reporting primary research involving an AMDT with pharmacy involvement
• Full-text papers published in peer-reviewed journals
• English-language full papers
• Papers involving interventions targeting hospital settings
The Exclusion Criteria Are as Follows
• Papers that were not available in full-text were discarded.
• Papers where there was either no multidisciplinary team or where the pharmacist had no role in the intervention were excluded.
Results
Searched Results
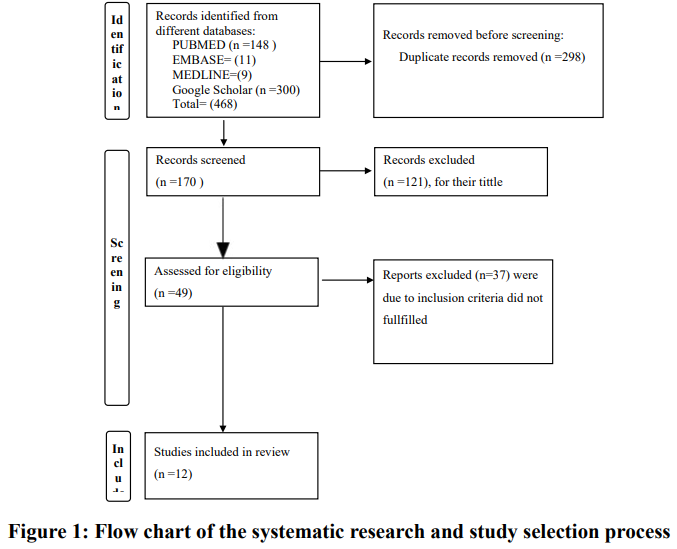
A total of 468 articles were obtained on initial searching from MEDLINE, EMBASE, PUBMED, and Google Scholar. A total of 298 articles were removed due to duplications. Finally, a total of 121 articles were excluded by observing their titles and abstracts. Consequently, only 37 articles were subjected to a full-text review. Finally, 12 articles were selected to be included in our review (Fig. 1).
Characteristics of Studies Included in This Review
In our review the filtered articles were pre and post interventional studies and randomized clinical trials studies. Articles included in this study were conducted on role of clinical pharmacist in reducing antimicrobial resistance. The majority of the studies were pre and post interventional studies in ten of the articles whereas RCTs in the two articles (Table 1) [5-16].
Rate of Reduction of Antimicrobial Resistance
Significantly less inappropriate doses for indication compared to the pre-intervention group (10.6% vs. 23.9%, p = 0.02), and less antibiotics prescribed for an inappropriate duration (15.8% vs. 32.4%, p < 0.01), more patients in the post intervention group had medications prescribed with appropriate dose, duration, and indication (51% vs. 66%, p = 0.04) [7]. Consumption of antimicrobials decreased from 48.9 % during pre-ASP to 36.9% in post-ASP (P = 0.001). The mean monthly antibiotic cost, during the pre-ASP was US$ 30,727.56, and US$ 9,623.73 in the last period of the study (P = 0.001) [Table 1] [10].
|
Author,Year [Reference] |
Country |
Setting |
Objective |
Study Design |
Study Duration |
Participants |
Types of Intervention |
Relevant Outcome |
Outcome Measure |
Total sample Size |
|
N. Elkassas et al, 2018[5] |
Egypt |
General Hospital |
To evaluate the acceptance of the role of the pharmacist in implementing antibiotic stewardship |
Pre-post study |
July,2014-Dec, 2015 |
Patients |
CP involved in advising physicians about proper selection of antibiotics |
Acceptance post intervention, (p<0.001) DRPs is reduced, compliance to clinical pharmacist by physician increased |
Defined daily dose (DDD) per 1000 patient-days |
805 |
|
Niaz Al-Somai.et al 2014 (6) |
Saudi Arabia |
Tertiary hospital |
to measure the |
|
|
Niaz Al-Somai.et al 2014 (6) |
Saudi Arabia |
Tertiary hospital |
to measure the |
357 |
|
Kiresten E. et al.2016 [7] |
USA |
Teaching hospital |
To assess the impact of pharmacist intervention on appropriateness of antimicrobial prescribing on a geriatric psychiatric unit |
Pre and post study |
August 2014 - January 2015 |
Patients |
CP reviewed patient chart and evaluated appropriateness of antimicrobial prescribing on geriatric psychiatric unit |
Significantly less inappropriate doses for indication compared to the pre-intervention group (10.6% vs. 23.9%, p = 0.02), and less antibiotics prescribed for an inappropriate duration (15.8% vs. 32.4%, p < |
Percentage |
133 |
|
|
|
|
|
|
|
|
|
0.01), more patients in the post intervention group had medications prescribed with appropriate dose, duration, and indication (51% vs. 66%, p = 0.04) |
|
|
|
N. Lauren, et al. 2019 [8] |
USA |
Hospital |
To evaluate the impact of a pharmacist-led ASP in the urgent care setting |
Pre-post study |
2014 - 2016 |
Patients |
N. Lauren, et al. 2019 [8] |
Antimicrobial prescribing for all patients including all diagnoses was significantly improved during |
pre- and post ASP compared by percentage |
300 |
|
|
|
|
|
|
|
|
|
the post-ASP period compared with the pre-ASP period (53.3% and 41.3%, respectively; p = 0.037) |
|
|
|
Hai-Xia Zhang. et al 2014 (9) |
China |
Tertiary hospital |
To evaluate the
impact and cost-benefit value of |
pre and post study |
January 1, 2011 to
June 30, 2012 |
Patients |
CP intervened real-time monitoring of medical records and controlling of the prescriptions of prophylactic |
Prolonged duration of prophylaxis decreased from 7.58 days to 2.91 days (p<0.001). Mean antibiotic cost decrease from $338.59 to $98.95 (p, 0.001).] and |
Cost benefit analaysis |
370 |
|
|
|
|
|
|
|
|
|
significant increase was observed in the rate of correct choice of antibiotics (p< 0.001) after the intervention |
|
|
|
Lucas M. et al. 2012 [10] |
Brazil |
Hospital |
To assess the impact of an intervention-prospective audit with feedback to prescriber, with and without the presence of a pharmacist in ASP team |
Pre-post study |
January 2003 to December 2008 |
Patients |
follow all patient-cases prospectively, recording the clinical data associated with the antimicrobial agent and the patient illness |
Consumption of antimicrobials decreased from 48.9 % during pre-ASP to 36.9% in post-ASP (P = 0.001). The mean monthly antibiotic cost, during the pre-ASP was US$ 30,727.56, and US$ 9,623.73 in the last period of the study (P = 0.001) |
mean monthly consumption in DDD/100 patient-days |
250 |
|
Box MJ. et al 2015 (11) |
California |
Health care center |
To assess impact of Pharmacists on ASP Teams in a Community Setting |
Pre and post study |
2011 - 2014 |
Patients |
CP has a role in educational interventions and pharmacist led antimicrobial therapy duration of iv treatment |
Improved the mean time to targeted antibiotic therapy (61.1 vs. 35.4 hrs; p = 0.001),
reduced median time to positive culture from 3 days to 2 days (p=0.0001), |
Mean, median and percentage |
212 |
|
|
|
|
|
|
|
|
|
Adherence to the antibiotic treatment was 48.4% in the CG and 67.2% in the IG, p = 0.033) |
|
|
|
Dunn K, et al. 201 1[12] |
Ireland |
university hospital |
To assess the impact of the introduction of antimicrobial subcommittee-led, pharmacist delivered guidelines and |
Pre-post study |
December 2006 to June 2007 |
Patients |
Application of stickers, guidelines to the drug chart, and providing consultation service to physician during |
Significant reduction in the duration of IV antimicrobial treatment Improvement in the timeliness of IV to PO switch |
Percentage and proportion |
753 |
|
|
|
|
criteria for switching from IV to PO antimicrobials |
|
|
|
IV to PO switch by PC |
|
|
|
|
Angoulvant F et al. 2013[13] |
France |
tertiary pediatric hospital, |
To evaluate therapeutic education delivered in a pediatric emergency care and attitudes about judicious |
randomized controlled trial |
February 2, 2009 to
September 26, 2011 |
Patients |
Therapeutic education on antibiotic was delivered by CP in the pediatric emergency department |
parents satisfied with the information on antibiotics received was significantly higher (96.9% versus 83%, P=0.002) |
percentage of parents satisfied |
300 |
|
|
|
|
antibiotic use |
|
|
|
|
|
|
|
|
Gross et al. 2001 [14] |
USA |
Tertiarycy Hospital |
To improve the quality of patient care by ensuring the effectiveness of treatment regimens |
Pre-post study |
November 1993 |
Patients |
Management of Antimicrobial recommendation |
Better antimicrobial recommendations, cost effectiveness |
Appropriateness use, cure and failure of the first regimen |
180 |
|
H. Khalili et al. 2013 [15] |
Iran |
university Hospital |
To evaluate the effect of clinical pharmacy services on medication costs |
Pre and post study |
September 2010 to September 2011 |
Patients |
CP intervention involved with adding, discontinuation, and changing the frequency, duration or dose of drugs and Management of drug interactions, therapeutic drug level monitoring, stability of drugs and preventing medication error |
Direct medication cost per patient was decreased ($160,140.5±12,445.1 versus $141,621.8±10,540.8),
Hospitalization duration of patients reduced (15.8±4.9 versus 17.3±5.6 days, P<0.001) and total number of ordered medication per patient was reduced by 9±4.7 and 6.6±3.1 (P<0.001), CP recommendation on stability of drugs and |
Percentage. and mean±standard deviation (SD) |
1996 |
|
|
|
|
|
|
|
|
|
preventing medication error was accepted 100% by nurses and physicians |
|
|
|
Gums et al, 1999 [16] |
USA |
Hospital |
To identify financial and outcome benefits of therapeutic intervention by a multidisciplinary antimicrobial treatment team |
RCT |
September 1994 to March 1996 |
Patients |
Clinical pharmacist involved in recommendations concerning antibiotic therapy and monitoring, as necessary |
Median length of stay was reduced from 9 to 5.7 days, (p=0.0001) Median patient services’ charges were reduced by |
Mean cost
Mean time |
252 |
|
|
|
|
composed of
Pharmacists, a clinical microbiologist, and an infectious disease specialist. |
|
|
|
|
$4404/intervention, (p=0.008) and median hospital costs were reduced by $2642/intervention ( p=0.016) |
|
|
Table1: Summary of included studies on role of clinical pharmacist in reducing antimicrobial resistance in, Ethiopia
Discussion
The results of our study revealed that pharmacists’ roles have expanded to provide multifaceted services in patient care, resulting in improved health outcomes from clinical services and reduced health care costs. This is consistent with the findings made in Australia [17]. In this review, the majority of articles showed the roles of clinical pharmacists in reducing the cost of antimicrobials, decreasing consumption of antimicrobials, significant reduction in duration of antibiotic use, and achieving optimal clinical outcomes related to antimicrobial use, which is in line with a study done at Peradeniya University in Australia in 2013[18]. Medications prescribed with appropriate dose, duration, and indication were observed in this study, which is in line with a study done at Louisiana University in the USA [19].
Conclusion
The provision of qualified clinical pharmacist services in healthcare systems has the potential to have a significant impact on reducing antimicrobial resistance. Studies from different countries have demonstrated that implementation of a pharmacist-led urgent care ASP, therapeutic advice, IV to PO conversion recommendation as per criteria, appropriate antimicrobial selection, and reduction of hospital stay and consumption of antimicrobials when they are recognized as part of the health care team. Antimicrobial stewardship involving pharmacists should be established in hospitals to ensure rational antimicrobial use. Therefore, integration of clinical pharmacist services into healthcare systems will assist in reducing the growth of catastrophic AMR.
Strengths and Limitations
To our knowledge, there have been few reviews of the actual or potential role of pharmacists in combating the challenge of AMR. This systematic review includes the novelty of summarizing the role of clinical pharmacists in reducing antimicrobial resistance available in literature. A limitation of this review is the inclusion of studies in English only, which can cause information bias. Moreover, only MEDLINE, EMBASE, PUBMED, and Google Scholar databases were searched. The absence of other databases such as Scopus could have introduced selection bias. While the authors discussed the inclusion criteria and data being extracted, there is still the potential for confusion bias.
References
- Draft political declaration of the high-level meeting of the General Assembly on antimicrobial resistance. New York: United Nations; 2016 (AMR 16-16108; accessed 13 June2019).
- Saha, S. K., Hawes, L., & Mazza, D. (2018). Improving antibiotic prescribing by general practitioners: a protocol for a systematic review of interventions involving pharmacists. BMJ open, 8(4), e020583.
- Sakeena, M. H. F., Bennett, A. A., & McLachlan, A. J. (2018). Enhancing pharmacists’ role in developing countries to overcome the challenge of antimicrobial resistance: a narrative review. Antimicrobial Resistance & Infection Control, 7, 1-11.
- Van Dijck, C., Vlieghe, E., & Cox, J. A. (2018). Antibiotic stewardship interventions in hospitals in low-and middle-income countries: a systematic review. Bulletin of the World Health Organization, 96(4), 266.
- Elkassas, N., Abbassi, M., & Farid, S. (2018). Evaluation of the physician’s acceptance to clinical pharmacy interventions after antibiotic stewardship implementation in the ICU in a general hospital in Egypt. Bulletin of Faculty of Pharmacy, Cairo University, 56(2), 219-223.
- Al-Somai, N., Al-Muhur, M., Quteimat, O., & Hamzah, N. (2014). The impact of clinical pharmacist and ID intervention in rationalization of antimicrobial use. Saudi Pharmaceutical Journal, 22(6), 516-521.
- Ellis, K., Rubal-Peace, G., Chang, V., Liang, E., Wong, N., & Campbell, S. (2016). Antimicrobial stewardship for a geriatric behavioral health population. Antibiotics, 5(1), 8.
- Fay, L. N., Wolf, L. M., Brandt, K. L., DeYoung, G. R.,Anderson, A. M., Egwuatu, N. E., & Dumkow, L. E. (2019). Pharmacist-led antimicrobial stewardship program in an urgent care setting. American Journal of Health-System Pharmacy, 76(3), 175-181.
- Zhang, H. X., Li, X., Huo, H. Q., Liang, P., Zhang, J. P., & Ge, W. H. (2014). Pharmacist interventions for prophylactic antibiotic use in urological inpatients undergoing clean or clean-contaminated operations in a Chinese hospital. PloS one, 9(2), e88971.
- Magedanz, L., Silliprandi, E. M., & Dos Santos, R. P. (2012). Impact of the pharmacist on a multidisciplinary team in an antimicrobial stewardship program: a quasi-experimental study. International journal of clinical pharmacy, 34, 290-294.
- Box, M. J., Sullivan, E. L., Ortwine, K. N., Parmenter, M. A., Quigley, M. M., Aguilarâ?Higgins, L. M., ... & Lim, R. A. (2015). Outcomes of rapid identification for gramâ?positive bacteremia in combination with antibiotic stewardship at a communityâ?based hospital system. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 35(3), 269-276.
- Dunn, K., O’Reilly, A., Silke, B., Rogers, T., & Bergin,C. (2011). Implementing a pharmacist-led sequential antimicrobial therapy strategy: a controlled before-and-after study. International journal of clinical pharmacy, 33, 208-214.
- Angoulvant, F., Rouault, A., Prot-Labarthe, S., Boizeau, P., Skurnik, D., Morin, L., ... & Bourdon, O. (2013). Randomized controlled trial of parent therapeutic education on antibiotics to improve parent satisfaction and attitudes in a pediatric emergency department. PLoS One, 8(9), e75590.
- Gross, R., Morgan, A. S., Kinky, D. E., Weiner, M., Gibson,G. A., & Fishman, N. O. (2001). Impact of a hospital-based antimicrobial management program on clinical and economic outcomes. Clinical Infectious Diseases, 33(3), 289-295.
- Khalili, H., Karimzadeh, I., Mirzabeigi, P., & Dashti-Khavidaki, S. (2013). Evaluation of clinical pharmacist's interventions in an infectious diseases ward and impact on patient's direct medication cost. European journal of internal medicine, 24(3), 227-233.
- Gums, J. G., Yancey Jr, R. W., Hamilton, C. A., & Kubilis, P. S. (1999). A randomized, prospective study measuring outcomes after antibiotic therapy intervention by a multidisciplinary consult team. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 19(12), 1369-1377.
- Sakeena, M. H. F., Bennett, A. A., & McLachlan, A. J. (2018). Enhancing pharmacists’ role in developing countries to overcome the challenge of antimicrobial resistance: a narrative review. Antimicrobial Resistance & Infection Control, 7, 1-11.
- Coombes, I., Fernando, G., Wickramaratne, M., Peters, N., Lynch, C., Lum, E., & Coombes, J. (2013). Collaborating to develop clinical pharmacy teaching in Sri Lanka. Pharmacy Education, 13(1), 29-35.
- LaRochelle, J. M., Ghaly, M., & Creel, A. M. (2012). Clinical pharmacy faculty interventions in a pediatric intensive care unit: an eight-month review. The Journal of Pediatric Pharmacology and Therapeutics, 17(3), 263-269.