
Journal of Clinical Rheumatology Research(JCRR)
ISSN: 2832-7756 | DOI: 10.33140/JCRR

Research Article - (2024) Volume 4, Issue 2
Infiltrated: The Intricacies of Phlegmon in an Adult Male -A Case Report in Frontier Corps Teaching Hospital Peshawar
Received Date: Oct 17, 2024 / Accepted Date: Nov 19, 2024 / Published Date: Nov 21, 2024
Copyright: ©Â©2024 Nayab Mustansar, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Mustansar, N., Khan, A. M., Afsar, M., Khan, S., Gohar, H., et al. (2024). Infiltrated: The Intricacies of Phlegmon in an adult male -A Case Report in Frontier Corp Teaching Hospital Peshawar. J Clin Rheum Res, 4(2), 01-04.
Abstract
Plegmon is an inflammatory mass that can result from various infectious or inflammatory processes, often observed in the context of acute appendicitis. This case report details a 37- year-old male presenting with severe right iliac fossa (RIF) pain, nausea, and vomiting, ultimately diagnosed with plegmon formation. The case underscores the clinical relevance of differentiating plegmon from other abdominal conditions, particularly acute appendicitis, and discusses the pathophysiological transition from appendicitis to plegmon.
Introduction
Plegmon is an inflammatory mass that can result from various infectious or inflammatory processes, often observed in the context of acute appendicitis. This case report details a 37- year-old male presenting with severe right iliac fossa (RIF) pain, nausea, and vomiting, ultimately diagnosed with plegmon formation. The case underscores the clinical relevance of differentiating plegmon from other abdominal conditions, particularly acute appendicitis, and discusses the pathophysiological transition from appendicitis to plegmon.
Case Presentation
A 37 years old male with history of severe RIF pain, nausea, and vomiting presented to FC teaching hospital Peshawar. No significant past medical or surgical history; no known comorbidities.
Clinical Examination
On Physical Examination, The Patient Appeared in Moderate Distress. Abdominal Examination Revealed:
• Tenderness-Marked in the RIF.
• Rebound Tenderness Present, indicating peritoneal irritation Guarding: Mild guarding observed, but no rigidity.
• Vital Signs: Stable; temperature mildly elevated at 99.5°F.
Investigations
Laboratory Tests:
• Elevated white blood cell count (WBC): 12,000/mm³ (normal range: 4,000-11,000/mm³).
• Mild elevation in C-reactive protein (CRP).
Ultrasound Abdomen:
• Hypoechoic mass in the RIF with surrounding inflammatory changes.
• No free fluid detected, but significant edema of adjacent tissues was noted.
CT Abdomen and Pelvis:
• Heterogeneous soft tissue mass consistent with plegmon.
• Peri-appendiceal inflammation observed, with no evidence of perforation or frank abscess formation as shown in figure:1 below:
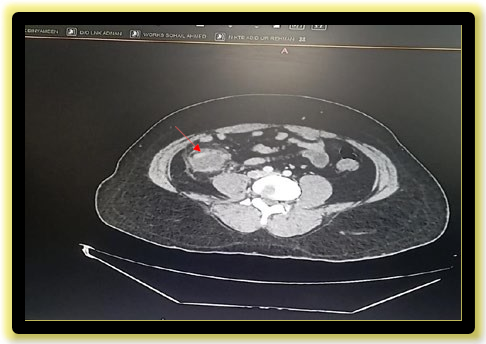
Figure 1: CECT abdomen Showing phlegmon formation as directed by arrow Differential Diagnosis
Considering the clinical presentation and imaging findings, the differential diagnoses included:
• Acute appendicitis with local inflammatory response
• Mesenteric lymphadenitis
• Crohn’s disease
• Omental infarction
Discussion
Acute Appendicitis: An Overview
Acute appendicitis is one of the most common surgical emergencies, characterized by inflammation of the appendix. It typically presents with abdominal pain, often starting periumbilically before migrating to the RIF, accompanied by nausea, vomiting, and fever and Signs include tenderness in the RIF, rebound tenderness, and occasionally, a palpable mass.
Pathophysiology of Appendicitis Leading to Plegmon Formation
• Initial Inflammation: Acute appendicitis often begins with obstruction of the appendiceal lumen (due to fecalith, lymphoid hyperplasia, or tumors), leading to increased intraluminal pressure and ischemia.
• Bacterial Proliferation: The obstruction results in stagnation of luminal contents, creating an environment conducive to bacterial growth. The most common pathogens involved include Escherichia coli, Bacteroides fragilis, and Enterococcus species.
• Inflammatory Response: The body's immune response leads to infiltration of neutrophils and macrophages into the appendiceal wall, resulting in edema and further obstruction.
• Progression to Plegmon: If the inflammation is contained and the infection does not progress to perforation, a localized inflammatory mass, or plegmon, may form. This is characterized by:
• Infiltration of Surrounding Tissues: The inflammatory process can extend to adjacent structures, causing edema and necrosis of peritoneal fat.
• Fibrosis: Over time, the inflammatory mass may become organized, leading to a fibrous capsule formation.
• Clinical Implications
Recognizing plegmon formation is critical for management. Misdiagnosis as a simple appendicitis can lead to inappropriate treatment, such as delayed surgical intervention, which may increase the risk of complications such as perforation, abscess formation, or peritonitis.
Management
Management of a patient with plegmon primarily involves:
• Conservative Treatment:
• Supportive Care: Pain management, hydration, and monitoring.
• Antibiotics: Initiation of broad-spectrum intravenous antibiotics to cover common
• pathogens. Antibiotic therapy is crucial in controlling infection and preventing complications.
• Surgical Intervention: Indicated if the patient does not improve with conservative
management or if there is progression to an abscess or significant clinical deterioration. In this case, due to the absence of abscess formation and stable clinical status, a conservative approach was initiated with close follow-up
Prognosis
The prognosis for patients with plegmon is generally favorable with appropriate management. Most cases resolve with conservative treatment, although complications can occur if the underlying cause is not adequately addressed.
Conclusion
This case highlights the importance of recognizing the transition from acute appendicitis to plegmon formation in patients presenting with RIF pain and gastrointestinal symptoms. Timely diagnosis and appropriate management are essential to prevent complications. Imaging studies play a critical role in identifying the nature of the inflammatory process, aiding clinicians in making informed decisions regarding patient care.
References
- Kirsner, J.B., & Abramson, S.B. (2020). "Plegmon: Clinical considerations." *Journal of Gastroenterology*, 55(6), 1249-1256.
- Heller, S., & Schreiber, M. (2018). "Management of abdominal plegmon: When to operate." *Annals of Surgery*, 267(5), 872877.
- Sato, K., & Seki, K. (2021). "Differentiation of plegmon from abscess in acute abdomen: A review." *Clinical Radiology*, 76(3),182-191.
- Tiwari, A., et al. (2019). "Ultrasound and CT imaging of plegmon: A case study." *British Journal of Radiology*, 92(1093), 20190022.