

Review Article - (2025) Volume 10, Issue 3
A Clinical Review on Intellectual Disability
2Psychiatrist and addiction treatment, Resident Doctor, Ain Shams University (ASU), Egypt
Received Date: Aug 25, 2025 / Accepted Date: Sep 22, 2025 / Published Date: Sep 26, 2025
Copyright: ©2025 Hesham Maged Mohamed Abdelfatah, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Abdelfatah, H. M. M., Gomaa, M. M. (2025). A Clinical Review on Intellectual Disability. Int J Psychiatry, 10(3), 01-09.
Abstract
About 2.3% of the population has an intellectual disability. The diagnosis of this disability is based on medical history, personal ability, and adaptive function. More than 75% of people with intellectual disability are classified as having mild intellectual disability, while a small percentage of people with severe symptoms are classified as having severe intellectual disability or profound intellectual disability. The specific cause of intellectual disability has not been identified, but genetics and heredity play a role. Complications before, during, or after birth also play a role. also, mother's Substance abuse and alcohol intake during pregnancy play a role, physical ill health and disabilities are more common in people with intellectual disabilities, mental ill health is more common in children and adolescents and adults with intellectual disabilities. Also, people with intellectual disabilities don’t live as long as other people, and life expectancy is shorter than in general population.
Keywords
Intellectual Disability, Mutation, Genetic Factors, Chromosomal Abnormality, Down Syndrome, Cognitive Function, Physical Ill Health, Lifespan
Discussion
At First We Discussed the Prevalence of Intellectual Disabilities that Not Uncommon
A meta-analysis of 52 studies reported the prevalence of intellectual disabilities to be 10.37/1000 population Prevalence varied according to age, income group of the country of origin (with higher rates from low income countries), and study design [1]. In high-income countries. rates for all ages combined were 9.2/1000, with the highest rates in child/young person populations only at 18.3/1000, and the lowest rates in adult-only populations at 4.9/1000. Careful understanding of the nuances is needed though to interpret these findings. Twenty-live of the studies included in the meta-analysis did not provide their age range: a further two did not report their observation period, and some studies were outliers in their findings. An earlier 1960 and 1987 is of lesser review of studies between relevance to today's population, given cohort effects, almost all were studies in childhood/youth, and some provided very limited meth-ideological information [2]. Studies of prevalence are, of course, challenging to conduct, as they ideally require intelligence to be tested on whole populations and therefore would considerable resources and costs. Other approaches can provide useful information, for example: Studies of administrative samples, such as people known to local authorities, which account for the majority of studies. These are the people who are making demands upon services, so the information is useful, but there are likely to be some people with intellectual disabilities not included in these samples and some people who do not have intellectual disabilities within the sample. For example, a rate of 4.3/1,000 aged 16+ was reported from Welsh local authorities as being in receipt or in need of intellectual disabilities services [3].
Studies of people with a record of intellectual disabilities in their general practitioner medical records. In high-income countries, people are likely to have been assessed once their developmental delay was reported, so a record is likely to exist. However, this is complicated by the multiple and changing terminology in use over time. For example, a rate of 5.4/1000 patients aged 18+ was re- ported from an English database of 451 practices [4].
Other secondary analysis of data routinely collected for other samples can be analyzed at relatively little costs, but findings refine purposes. These have the attraction that large and whole country the original definitions used and the ways the data were collected for example, a rate of 4.9/1000 aged 16+ (self-/proxy report) was reported from an analysis of Scotland's 2011 census 5, and a rate of 23/1000 school-aged children/young persons (teacher report was reported from Scotland's 2015 pupil census 6.
Population intelligence approximates to a normal distribution with a mean intelligence quotient of 100 and a standard deviation of 15 points. A statistical definition of intellectual impairments is an intelligence quotient less than two standard deviations from the mean, that is, <70. Simplistically, this would suggest that 2.3% of the population have intellectual impairments [5]. However: The greatest deviation from the normal distribution of intelligence is at the extreme ends.
A test error of 5 points is recognized-and a normal distribution would place 2.5% within the range of 70-75, so this can greatly in fluency identified prevalence.
There is the Flynn effect (overly high scores due to out-of-date test norms). Intellectual disabilities are a social construct, not simply a statistical measure of impairments; the definitions of intellectual disabilities in the standard classificatory manuals ICD-10 and DSM-5 also include the functional requirement of the need for additional support [6-8]. People learn throughout their lives, and so a child with an intelligence quotient of 69 will need additional educational support at school but, as an adult, may gradually acquire life skills to live independently, maintain relationships, hold employment, raise children, and not identify with intellectual disabilities nor be identified by others as having intellectual disabilities or put demand on services designed for people with intellectual disabilities. In countries that provide additional educational support for children with intellectual disabilities, there is a clear advantage to having the label, and flexibility in its use is beneficial for children with abilities that are a little above an intelligence quotient of 70 ('borderline' intellectual disabilities).
People with intellectual disabilities experience premature death hence the proportion of the population with intellectual drivable as progressively falls within older age groups. abilities until they attend school, so rates are lower in pre-scholar’s than in school- aged children. Cohort effects can influence rates over time, for example, the sika virus epidemic in South America in 2015-2016 causing micro-cephaly, immunization, iodine, maternal smoking, and alcohol intake (currently falling, but could possibly increase with the introduction of first trimester diagnosis, improved antenatal, perinatal, and neonatal health care, increased survival of very low-birthweight infants, identification and treatment of metabolic causes of intellectual disabilities like phenylketonuria, better childhood education, access to cardiac surgery for children with Down syndrome, improved lifestyles, and access to health care [9].
Migration and clustering can influence spatial patterning at local levels and can be influenced by economic factors and local policy. Prevalence of mild intellectual disabilities is influenced by many cultural and societal factors that determine whether a mild learning impairment is likely to result in a functional disability, contributing to geographic differences. Clearly, there is an intellectual gradient across the population, and the cut-off of 70 is purely arbitrary. Indeed, the accepted cut-off was changed in 1973, substantially affecting rates. Despite these complexities, there are some reasonably consistent findings across studies: In high-income countries, about 5/1000 adults have intellectual disabilities, falling to about 2/1000 over the age of 65 years.
Prevalence is higher in children and young people than in adults. Prevalence is higher in boys/men than girls/women; across the whole of Scotland, 58% of people with intellectual disabilities are male [5].
Prevalence is higher in low-income countries than in high- and middle-income countries for multiple reasons, including life-style and health care, although in areas that are less driven by technol- ogy, having mild intellectual impairments may be less disabling. The great majority of people with intellectual impairments have mild intellectual impairments (6 mild impairment: 1 moderate to profound impairments), and the majority with intellectual impair- ments in whom this is disabling have mild, rather than severe, in- tellectual disabilities.
Causes and Degree of Intellectual Disabilities
People with intellectual disabilities have some characteristics in common such as needing additional educational support at school, finding it hard to manage money and bills without help as an adult, and having difficulties remembering the temporal sequencing of events. Every person with intellectual disabilities is also unique. Each child inherits a range of genetic information from both their parents which is not shared with other children with intellectual. Identifying the cause of intellectual debilities is undertaken by pediatrician’s and clinical geneticists. There are four degrees of intellectual disability (Mild – Moderate – Severe – Profound).

Figure 1: Degrees of Intellectual Disability
Genetic Factors
Genetic studies indicate intelligence is highly heritable and can itself be conceptualized as a spectrum of syndromes [10]. Additionally, there are many genetic causes of intellectual disabilities, and recent and ongoing studies have found numerous copy number variants associated with developmental disorders. genetic conditions include: Chromosomal anomalies, Examples are trisomy Down syndrome (trisomy 21). Palau’s syndrome (trisomy 13), Edwards syndrome (trisomy 15); autosomal deletions, for example, cri-du chat syn- drome (terminal deletion of chromosome 15), Williams syndrome (deletion on chromosome 7), and Prader-Willi syndrome and An- gelman's syndrome (deletion on chromosome 15 or uniparental disomy), and sex-linked conditions, for example, fragile X syn- drome. Autosomal and sex-linked recessive conditions (particu- larly in communities with high rates of consanguinity). Examples are phenylketonuria, homocystinuria, galactosaemia, lipid disor- ders-Tay-Sachs disease, Gaucher disease, Niemann-Pick disease; and mucopolysaccharidoses Hunter's disease and Hurler's disease. Autosomal and sex-linked dominant conditions. Examples in tu- berous sclerosis and neurofibromatosis.
Regarding the Prevalence of Individual Conditions in Childhood
1/800 has Down syndrome.
1/3600 boys and 1/4000-6000 girls have fragile-X syndrome.
1/7500 has Williams syndrome.
1/10,000 has Cornelia de Lange.
1/10,000-25,000 has Prader-Willi syndrome.
1/15,000 has Angelman syndrome.
1/20.000 has Smith-Magenis syndrome.
1/50,000 has cri-du-chat syndrome.
In addition to causing intellectual disabilities, physical condition’s, and influencing trajectories, these genetic conditions can cause a range of other cognitive, behavioural, and mental health problems, for which the term 'behavioural phenotype is used. Behavioural phenotypes have attracted particular research attention and can in- form clinical assessments. Examples include high rates of demen- tia in middle-aged and older adults with Down syndrome; affective psychosis in Prader-Willi syndrome; self-injurious behavioral in Smith-Magnus syndrome; and depression in phenylketonuria [11- 16]. While these behavior’s/mental ill as interventions may help the individual. Additionally, some health is genetically driven, it is important to avoid therapeutic nihilism syndromes effect phys- iological differences, which influence treatment choices, for ex- ample, the low rates of heart disease and low blood Pressure in down syndrome differing immunology causing high rate of thyroid disorder and other immunological disorders.

Figure 2: Two main of ID Etiologic Genetic Factors
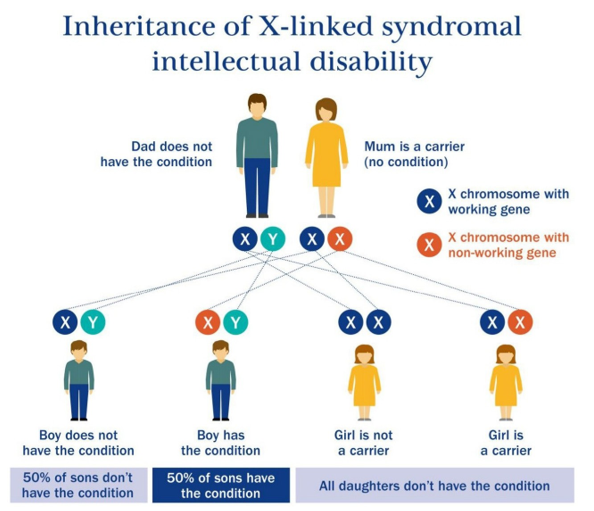
Figure 3: Inheritance of X-linked Syndromal Intellectual Disability
Antenatal Factors
Include, Teratogenic drugs and toxins. Examples include alcohol Infections. Examples include toxoplasmosis, rubella, cytomegalo- virus, herpes simples, syphilis, zika virus, and other infections. Fetal growth retardation. Examples include placental dysfunction and hypoxia Endocrine. Examples include iodine deficiency
Perinatal Factors
Include: Birth injury, especially in premature and low-birthweight infants Kernicterus, Infections, Postnatal factors,Postnatal Factors Include
Infections, encephalitis, Toxins, Brain tumor’s, Head injury, Starvation.
Extreme prematurity has been shown to account for 17% of cases of intellectual disabilities, together, gestational age and birthweight centile have been reported to account for 26.6% of intellectual dis-abilities [17]. The month of conception (January-March conception, compared with summer conception) has been reported to account for 15% of intellectual disabilities, postulated to be related to vitamin D or infections at the critical first trimester stage of development [18]. Fetal alcohol syndrome is underdiagnosed.
Mental Ill Health
Two recent systematic reviews reported that mental ill health is more common in children, young people, and adults with intellectual disabilities than in the general population [19,20]. Problem behaviors, such as aggressive, self-injurious, and destructive behavior, are very common in people with intellectual disabilities and do not have an obvious comparator in the general population. Widely reported prevalence rates have been given in view of differences in populations studied (some from mental health services and so their rates are biased and inflated), methods used to identify mental ill health, the types of conditions included within the re-ported mental ill health (particularly whether or not problem be haviours and/or autism are included), the diagnostic criteria used whether studies are reporting point or life pre disorders,lation if strictly applied, especially for public CD-10 and DSM-5 under- report mental ill It is not surprising that mental ill health is more with intellectual disabilities, compared with the general population in view of complex biological factors, psychological and oral advantages, and additional developmental factors [22].
Population-based studies in children and young people with intellectual disabilities reported the prevalence of mentality including problem behaviors, ranging from 30% [23-25]. A robust UK study reported a rate of 36% in 1 chi young people (aged 5-16 years) with intellectual disabilities com pared with 8% of 17.774 children without intellectual disabilities in the same survive the children and young people with intellectual disabilities accounted for 14% of all children with mental health [26].
Population-based studies in adults with intellectual disabilities reported the prevalence of mental ill health, excluding problem be haviours, ranging from 14.5% (when also excluding ADHD, dementia, and personality disorder, people aged 65 and over, and people with severe intellectual disabilities (271) to 43.8% (with moderate to profound intellectual disabilities only [27-28]. The largest adult population-based prevalence study, in which each person was individually assessed, included 1023 adults with im lectual disabilities [29]. It reported a point prevalence of mental health of 40.9%, or 28.3% excluding problem behavior’s, and more robust methods than previous smaller studies [30,31]. Some types of mental ill health are more common in people with intellectual disabilities, including schizophrenia, bipolar disorder, dementia (particularly in adults with Down syndrome), but also in adults with intellectual disabilities of other or unknown causes, autism [26,32-38]. ADHD, and pick with intellectual disabilities are reported to be higher than for other children and young people for 27 out of 28 ICD-10 categories (26) Prevalence rates of mental ill health in children and young people Depression and anxiety are common in people with intellectual dis abilities, but probably not more so than in the general population [34,39].
intellectual disabilities. In a large-scale, population-based study of Problem behaviors are very common in the population with adults aged 16+ years, 22.5% were reported to have problem behaviors, and of those, 10% had aggressive behavior and 5% had self- injurious behavior [29,40,41].
The incidence of mental ill health in adults, excluding problem for psychotic disorders [33,42]. The incidence of dementia has also behaviors, has been reported to be 12.6% over a 2-year period- been reported for older adults with intellectual disabilities NOT 8.3% for affective disorders, 1.7% for anxiety disorders, and 1.4% due to Down syndrome and found to be considerably higher than for the age-matched general population. At the age of 65 years or older, the standardized incidence ratio for dementia was 4.98 [43]. Regarding problem behaviours, the 2-year incidence of aggression was reported as 1.8%, and of self-injury 0.6% [40,41]. Full remission of psychosis after 2 years was only 14.3%, aggression 27.7% [33]. incidences are higher than those found in the general population. much of the current high prevalence of mental ill health is due to and self-injury 38.2% [40,41]. These findings suggest that while incidence is higher than those found in the general population much of the current high prevalence of mental ill health is due to. Enduring disorders, rather than new episodes, though research on this is limited in quantity. longitudinal cohorts show high and enduring rates of depression Studies on common types of mental ill health using general population and anxiety in adults with intellectual disabilities, compared with the general population [44-46].
Longitudinal studies have also reported on the mental ill health of children and young people with intellectual disabilities. In in Australian cohort study, children and young people aged 4-195 years were followed over four waves of data collection over 14 years. High rates of psychopathology levels were reported, with hyperactivity more prominent at younger ages and persisting for longer in children/young people with more severe degrees of intel-lectual disabilities. Emotional disorders emerged later in childhood [47-49]. Similar findings have been reported from longitudinal studies in children with intellectual disabilities/ borderline intellectual disabilities (excluding those with more severe intellectual dis-abilities or with additional sensory or physical disabilities) in the Netherlands [50,51].
Neurodevelopmental Disorders Cluster
The term 'ESSENCE' (Early Symptomatic Syndromes Eliciting Neurodevelopmental Clinical Examination) to describe this [52]. He defined ESSENCE as major problems in: motor skills; general development; speech and language, social interaction and communication; behavior; hyperactivity or impulsivity; hypo activity, inattention; and sleep or feeding difficulties. Genetic data also increasingly support clustering of neurodevelopmental (including epilepsy) and mental health problems [53].
Physical Ill Health, Disabilities, and Multi-Morbidity
Additional physical ill health and disabilities are common in people with intellectual disabilities. Indeed, multi-morbidity is typical for people with intellectual disabilities, and hence too is polypharmacy [4,54]. This has implications, as it adds complexity to mental and physical health assessments (for example, distinguishing be- tween complex partial seizures, depression, and anti-epileptic drug side effects), in assessments that are also challenging due to communication needs, impairment of understanding, and visual and hearing impairments, all of which are common in people with intellectual disabilities. This probably contributes to the under- recognition of mental ill health that occurs in this population. It also means that there are more disease-disease, drug-disease, and drug- drug inter-actions to take account of when managing conditions. For example, postural problems and deformities (common in people with cerebral palsy and people with profound intellectual disabilities) impact upon gastro-oesophageal reflux disease (GORD), which is extremely common in people with intellectual disabilities, more so the more severe their intellectual disabilities, and can cause anxiety, GORD occurs in about 50% of adults with intellectual disabilities, a con sequence is that drugs to manage osteoporosis cannot be tolerated, drugs, commonly prescribed for people with intellectual disabilities, and osteoporosis is common in this population. Many psychotropic lower the seizure threshold, and epilepsy is common. People with intellectual disabilities may not be able to self-report drug side effects is essential. Anticholinergic burden due to polypharmacy of drugs and are reliant on others observing these; hence, pharmacovigilance with these side effects is an issue for people with intellectual disabilities, with potential negative side effects such as further impairment of cognition [55].
Long-term conditions are more common for adults with intel- lectual disabilities, compared to the general population. Children, young people, and adults with intellectual disabilities have higher rates of epilepsy (25%), visual impairment (50%), hearing impairment (40%), impacted cerumen, GORD (50%), dysphagia, constipation, diabetes, thyroid dysfunction, osteoporosis, contractures, mobility and balance impairments, injuries, eczema, xerosis, obesity, and heart failure, compared with the general population [4,54,56-60]. Asthma is also reported to be more common in people with intellectual disabilities and may be due to obesity, but it is possible that some of this is a misdiagnosis of reflux pneumonitis or aspiration pneumonia. In some cases, the excess physical ill health burden relates to the person's underlying cause of intellectual disabilities (for example, thyroid dysfunction and Down syndrome). but lifestyle and environmental factors and suboptimal support and health care are also important contributors. Some problems pre-dispose to others. For example, psychotropic drugs (prescribed to about 20% of the adult population with intellectual disabilities) can increase diabetes risk, as can obesity which is common, and sedentary lifestyles, also common [61-63]). In view of the shorter life expectancy of people with more severe intellectual disabilities and those with syndromal causes for their intellectual disabilities, older adults with intellectual disabilities s have different characteristics, compared with younger adults. Older adults as a group have milder levels of intellectual disabilities and lesser quantities of additional physical ill health. The profile of their health needs changes, as they have lower rates of the physical ill health and disabilities associated with severe intellectual disabilities but start to acquire physical ill health associated with ageing. In extreme old age, the health characteristics of people with intellectual disabilities becomes more like those of the general population.
Lifespan
People with intellectual disabilities do not live as long as other people; and life expectancy is shorter, the more severe the person's intellectual disabilities. A recent systematic review included 27 studies and found that although life expectancy has improved in recent decades, it is lower, compared with the general population. by about 20 years, with no evidence of any closure of the inequality gap [64]. More severe intellectual disabilities and/or additional comorbidities were associated with the shortest life expectancy. Standardized mortality rates showed a greater inequality for women than for men, for reasons that are unknown. The main causes of death differed from the general population, with respiratory disease the most common, then circulatory diseases.
greater congenital, and lesser ischemic, disease compared with the general population). Cancer was less common, compared with the general population, and the cancer profile differed from that in the general population.
Specific syndromes can also shorten life expectancy, including death in utere and in infancy and childhood. Life expectancy for people with Down syndrome has improved markedly over the last 50 years, with access to treatments for congenital heart disorders and improved surgical techniques and post-operative care accounting for much of this , but is still reported to be 30 years less than in the general population [65]. Down syndrome has been reported to occur in 1.2/1000 pregnancies, of which 78.1% are live births. Survival at 1 year for live births in 1995-1999 was 91.6% , and 85% are estimated to survive to 10 years [66,67]. The proportion of people with Down syndrome reduces in older cohorts, 75% survive to 50 years, 50% to 58.6 years, and 25% to 62.9 years [68].
The shorter life expectancy of people with intellectual disabilities does not relate to syndromal causes of death and multi-morbidity. Some deaths are potentially avoidable, being amenable to good quality care. A confidential inquiry reviewed 247 deaths of people with intellectual disabilities, finding that 22% were aged less than 50 years [69]. Avoidable deaths from causes that could have been amenable to good-quality health care occurred in 37%, com- pared with only 13% of the general population [69]. A further large-scale study (16,666 people with intellectual disabilities-656 deaths. compared with age, gender, and practice-matched controls, 113,562-1358 deaths) also found high rates of deaths amenable to good-quality health care at 37.0%, compared with 22.5% in the general population [70]. The authors also pointed out the standard definition of amenable deaths they used did not include some types of death that could be considered amenable to health care and which they found occurred more commonly in people with intellectual disabilities, including deaths from urinary tract infections and aspiration pneumonitis [70]. Hence, these disturbing figures are actually an undercount of the deaths amenable to good care that people with intellectual disabilities experience. Improving health care for people with intellectual disabilities needs to become a priority for clinicians, service commissioners, and policymakers.
Conclusion
While a variety of studies focus on the multiple potential risk factors for intellectual disability, few have comprehensively examined the groups most at risk. Our review indicates that the risk is higher in cases of lower socioeconomic status, ethnicity, teenage motherhood, adolescent mental illness, and alcoholism. This highlights the target of desirable strategies. These include identifying and monitoring at-risk groups before, during, and after pregnancy, as well as the potential for new developmental disabilities in children, improved antenatal, perinatal, and neonatal health care, increased survival of very low-birthweight infants, identification and treatment of metabolic causes of intellectual disabilities like phenylketonuria, better childhood education, access to cardiac surgery for children with Down syndrome, improved lifestyles, and access to health care.
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this article.
Funding& Support
This research did not receive grants from any funding agency in the public and commercial sector.References
- Maulik, P. K., Mascarenhas, M. N., Mathers, C. D., Dua, T., & Saxena, S. (2011). Prevalence of intellectual disability: a meta-analysis of population-based studies. Research in developmental disabilities, 32(2), 419-436.
- Roeleveld, N., Zielhuis, G. A., & Gabreels, F. (1997). The prevalence of mental retardation: a critical review of recent literature.
- Feice, D. (2004). Interpretation of intellectual disability in Wales for policy and strategic purposes. Welsh Centre for Intellectual Disabilities, Cardiff. 12.
- Carey, I. M., Shah, S. M., Hosking, F. J., DeWilde, S., Harris, T., Beighton, C., & Cook, D. G. (2016). Health characteristics and consultation patterns of people with intellectual disability: a cross-sectional database study in English general practice. British Journal of General Practice.
- Scottish Learning Disabilities Observatory. Scotland: population characteristics. http://www.sldo.ac.uk/census- 2011-information/learningdisabilities/topics/population/
- Scottish Learning Disabilities Observatory Children and young people with disabilities and autism spectrum disorders identified through the Scottish Pupil Census. https://www. sldo.at.uk/ projects/children-and-young-people-health/pup- census/.
- World Health Organization. (1992). The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines (Vol. 1). World Health Organization.
- Edition, F. (2013). Diagnostic and statistical manual of mental disorders. Am Psychiatric Assoc, 21(21), 591-643.
- Jacobs, M., Cooper, S. A., McGowan, R., Nelson, S. M., & Pell, J. P. (2016). Pregnancy outcome following prenatal diagnosis of chromosomal anomaly: a record linkage study of 26,261 pregnancies. PLoS One, 11(12), e0166909.
- Davies, G., Tenesa, A., Payton, A., Yang, J., Harris, S. E., Liewald, D., ... & Deary, I. J. (2011). Genome-wide association studies establish that human intelligence is highly heritable and polygenic. Molecular psychiatry, 16(10), 996-1005.
- Oliver, C., Holland, A. J. (1986). Down's syndrome and Alzheimer's dis ease: a review. Psychological Medicine, 16,307-22.
- Prasher, V. P. (1995). Agespecific prevalence, thyroid dysfunction and depressive symptomatology in adults with Down syndrome and dementia. International Journal of Geriatric Psychiatry, 10(1), 25-31.
- Bouras, N., Beardsmore, A., Dorman, T., Cooper, S. A., & Webb, T. (1998). Affective psychosis and Prader–Willi syndrome. Journal of Intellectual Disability Research, 42(6), 463-471.
- Soni, S., Whittington, J., Holland, A. J., Webb, T., Maina, E., Boer, H., & Clarke, D. (2007). The course and outcome of psychiatric illness in people with Prader–Willi syndrome: implications for management and treatment. Journal of Intellectual Disability Research, 51(1), 32-42.
- Taylor, L., & Oliver, C. (2008). The behavioural phenotype of Smith–Magenis syndrome: evidence for a gene– environment interaction. Journal of Intellectual Disability Research, 52(10), 830-841.
- Pietz, J., fatkenheuer, B., Armbruster, M., Esser, G., & Schmidt, H. (1997). Psychiatric disorders in adult patients with early-treated phenylketonuria. Pediatrics, 99(3), 345-350.
- Mackay, D. F., Smith, G. C. S., Dobbie, R., Cooper, S. A., & Pell, J. P. (2013). Obstetric factors and different causes of special educational need: retrospective cohort study of 407 503 schoolchildren. BJOG: An International Journal of Obstetrics & Gynaecology, 120(3), 297-308.
- Mackay, D.F., Smith, G. C. S., Cooper, S-A. et al. (2016). Month of conception and developmental disorders: A record- linkage study of 801,603 children. American Journal of Epidemiology. 184,485-93.
- Buckles, J., Luckasson, R., & Keefe, E. (2013). A systematic review of the prevalence of psychiatric disorders in adults with intellectual disability, 2003–2010. Journal of Mental Health Research in Intellectual Disabilities, 6(3), 181-207.
- Einfeld, S. L., Ellis, L. A., & Emerson, E. (2011). Comorbidity of intellectual disability and mental disorder in children and adolescents: A systematic review. Journal of Intellectual and Developmental Disability, 36(2), 137-143.
- Smiley, E. (2005). Epidemiology of mental health problems in adults with learning disability: an update. Advances inpsychiatric treatment, 11(3), 214-222.
- Simpson, N., Mizen, L., & Cooper, S. A. (2016). Intellectual disabilities. Medicine, 44(11), 679-682.
- Rutter, M., Tizard, J., & Whitmore, K. (1970). Education,health, and behaviour. (No Title).
- Birch, H. G. (1970). Mental subnormality in the community: a clinical and epidemiologic study.
- Dekker, M. C., Koot, H. M., Ende, J. V. D., & Verhulst, F. C. (2002). Emotional and behavioral problems in children and adolescents with and without intellectual disability. Journal of Child Psychology and Psychiatry, 43(8), 1087-1098.
- Emerson, E., & Hatton, C. (2007). Mental health of children and adolescents with intellectual disabilities in Britain. The British Journal of Psychiatry, 191(6), 493-499.
- Deb, S., Thomas, M., & Bright, C. (2001). Mental disorder in adults with intellectual disability. 1: Prevalence of functional psychiatric illness among a community-based population aged between 16 and 64 years. Journal of Intellectual Disability Research, 45(6), 495-505.
- Bailey, N. (2007). Prevalence of psychiatric disorders in adults with moderate to profound learning disabilities. Advances in Mental Health and Learning Disabilities, 1(2), 36-44.
- Cooper, S. A., Smiley, E., Morrison, J., Williamson, A., & Allan, L. (2007). Mental ill-health in adults with intellectual disabilities: prevalence and associated factors. The British journal of psychiatry, 190(1), 27-35.
- Cooper, S. A., & Bailey, N. M. (2001). Psychiatric disorders amongst adults with learning disabilities-prevalence and relationship to ability level. Irish Journal of Psychological Medicine, 18(2), 45-53.
- Corbett, J. A. (1979). Psychiatric morbidity and mentalretardation. Psychiatric illness and mental handicap, 11-25.
- Turner, T. H. (1989). Schizophrenia and mental handicap: an historical review, with implications for further research. Psychological medicine, 19(2), 301-314.
- Cooper, S. A., Smiley, E., Morrison, J., Allan, L., Williamson, A., Finlayson, J., ... & Mantry, D. (2007). Psychosis and adults with intellectual disabilities: Prevalence, incidence, and related factors. Social psychiatry and psychiatric epidemiology, 42(7), 530-536.
- Cooper, S. A., Smiley, E., Allan, L., & Morrison, J. (2018). Incidence of unipolar and bipolar depression, and mania in adults with intellectual disabilities: prospective cohort study. The British Journal of Psychiatry, 212(5), 295-300.
- Cooper, S. A. (1997). High prevalence of dementia among people with learning disabilities not attributable to Down's syndrome. Psychological medicine, 27(3), 609-616.
- Strydom, A., Livingston, G., King, M., & Hassiotis, A. (2007). Prevalence of dementia in intellectual disability using different diagnostic criteria. The British Journal of Psychiatry, 191(2), 150-157.
- Baird, G., Simonoff, E., Pickles, A., Chandler, S., Loucas, T., Meldrum, D., & Charman, T. (2006). Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP). The lancet, 368(9531), 210-215.
- Brugha, T. S., Spiers, N., Bankart, J., Cooper, S. A., McManus, S., Scott, F. J., ... & Tyrer, F. (2016). Epidemiology of autism in adults across age groups and ability levels. The British Journal of Psychiatry, 209(6), 498-503.
- Reid, K. A., Smiley, E., & Cooper, S. A. (2011). Prevalence and associations of anxiety disorders in adults with intellectual disabilities. Journal of Intellectual Disability Research, 55(2), 172-181.
- Cooper, S. A., Smiley, E., Jackson, A., Finlayson, J., Allan, L., Mantry, D., & Morrison, J. (2009). Adults with intellectual disabilities: prevalence, incidence and remission of aggressive behaviour and related factors. Journal of intellectual disability research, 53(3), 217-232.
- Cooper, S. A., Smiley, E., Allan, L. M., Jackson, A., Finlayson, J., Mantry, D., & Morrison, J. (2009). Adults with intellectual disabilities: prevalence, incidence and remission of selfâ?ÂÃÂ?ÂÂinjurious behaviour, and related factors. Journal of Intellectual Disability Research, 53(3), 200-216.
- Smiley, E., Cooper, S. A., Finlayson, J., Jackson, A., Allan, L., Mantry, D., ... & Morrison, J. (2007). Incidence and predictors of mental ill-health in adults with intellectual disabilities: prospective study. The British Journal of Psychiatry, 191(4), 313-319.
- Strydom,A., Chan, T., King, M., Hassiotis,A., & Livingston, G. (2013). Incidence of dementia in older adults with intellectual disabilities. Research in developmental disabilities, 34(6), 1881-1885.
- Maughan, B., Collishaw, S., & Pickles, A. (1999). Mild mental retardation: psychosocial functioning in adulthood. Psychological Medicine, 29(2), 351-366.
- Collishaw, S., Maughan, B., & Pickles, A. (2004). Affective problems in adults with mild learning disability: the roles of social disadvantage and ill health. The British Journal of Psychiatry, 185(4), 350-351.
- Richards, M., Maughan, B., Hardy, R., Hall, I., Strydom, A., & Wadsworth, M. (2001). Long-term affective disorder in people with mild learning disability. The British Journal of Psychiatry, 179(6), 523-527.
- Einfeld, S. L., & Tonge, B. J. (1996). Population prevalence of psychopathology in children and adolescents with intellectual disability: II epidemiological findings. Journal of Intellectual Disability Research, 40(2), 99-109.
- Tonge, B. J., & Einfeld, S. L. (2003). Psychopathology and intellectual disability: The Australian child to adult longitudinal study. International review of research in mental retardation, 26(1), 61-91.
- Einfeld, S. L., Piccinin, A. M., Mackinnon, A., Hofer, S. M., Taffe, J., Gray, K. M., ... & Tonge, B. J. (2006). Psychopathology in young people with intellectual disability. Jama, 296(16), 1981-1989.
- Wallander, J. L., Dekker, M. C., & Koot, H. M. (2006). Risk factors for psychopathology in children with intellectual disability: a prospective longitudinal population-based study. Journal of Intellectual Disability Research, 50(4), 259- 268.
- De Ruiter, K. P., Dekker, M. C., Verhulst, F. C., & Koot, H. M.(2007). Developmental course of psychopathology in youths with and without intellectual disabilities. Journal of Child Psychology and Psychiatry, 48(5), 498-507.
- Gillberg, C. (2010). The ESSENCE in child psychiatry: early symptomatic syndromes eliciting neurodevelopmental clinical examinations. Research in developmental disabilities, 31(6), 1543-1551.
- Moreno-De-Luca, A., Myers, S. M., Challman, T. D., Moreno- De-Luca, D., Evans, D. W., & Ledbetter, D. H. (2013). Developmental brain dysfunction: revival and expansion of old concepts based on new genetic evidence. The Lancet Neurology, 12(4), 406-414.
- Cooper, S. A., McLean, G., Guthrie, B., McConnachie, A., Mercer, S., Sullivan, F., & Morrison, J. (2015). Multiple physical and mental health comorbidity in adults with intellectual disabilities: population-based cross-sectional analysis. BMC family practice, 16(1), 110.
- O'Dwyer, M., Peklar, J., McCallion, P., McCarron, M., & Henman, M. C. (2016). Factors associated with polypharmacy and excessive polypharmacy in older people with intellectual disability differ from the general population: a cross-sectional observational nationwide study. BMJ open, 6(4), e010505.
- Bowley, C., & Kerr, M. (2000). Epilepsy and intellectual disability. Journal of Intellectual Disability Research, 44(5), 529-543.
- Böhmer, C. J. M., Niezen-de Boer, M. C., Klinkenberg-Knol,E. C., Devillé, W. L. J. M., Nadorp, J. H. S. M., & Meuwissen,S. G. M. (1999). The prevalence of gastroesophageal reflux disease in institutionalized intellectually disabled individuals. Oficial journal of the American College of Gastroenterology| ACG, 94(3), 804-810.
- Robertson, J., Chadwick, D., Baines, S., Emerson, E., Hatton,C. (2017). People with intellectual disabilities and dysphagia.Disability Rehabilitation, 12,1-16.
- McCarron, M., Swinburne, J., Burke, E., McGlinchey, E., Carroll, R., & McCallion, P. (2013). Patterns of multimorbidity in an older population of persons with an intellectual disability: results from the intellectual disability supplement to the Irish longitudinal study on aging (IDS-TILDA). Research in developmental disabilities, 34(1), 521-527.
- Hermans, H., & Evenhuis, H. M. (2014). Multimorbidity in older adults with intellectual disabilities. Research indevelopmental disabilities, 35(4), 776-783.
- Sheehan, R., Hassiotis, A., Walters, K., Osborn, D., Strydom, A., & Horsfall, L. (2015). Mental illness, challenging behaviour, and psychotropic drug prescribing in people with intellectual disability: UK population based cohort study. Bmj, 351.
- Melville, C. A., Cooper, S. A., Morrison, J., Allan, L., Smiley, E., & Williamson, A. (2008). The prevalence and determinants of obesity in adults with intellectual disabilities. Journal of applied research in Intellectual Disabilities, 21(5), 425-437.
- Finlayson, J., Jackson,A., Cooper, S.A., Morrison, J., Melville, C., Smiley, E., ... & Mantry, D. (2009). Understanding predictors of low physical activity in adults with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, 22(3), 236-247.
- O'Leary, L., Hughes-McCormack, L., Cooper, S-A. (2018). Life expectancy and causes of death of people with intellectual disabilities: a systematic review. Journal of Applied Research in Intellectual Disabilities, 31, 325-342.
- Hijii, T., Fukushige, J., Igarashi, H., Takahashi, N., & Ueda, K. (1997). Life expectancy and social adaptation in individuals with Down syndrome with and without surgery for congenital heart disease. Clinical Pediatrics, 36(6), 327-332.
- Bell, R., Rankin, J., & Donaldson, L. J. (2003). Down's syndrome: occurrence and outcome in the north of England, 1985–99. Paediatric and perinatal epidemiology, 17(1), 33-39.
- Leonard, Bower, Petterson, & Leonard. (2000). Survival of infants born with Down’s syndrome: 1980–96. Paediatric and perinatal epidemiology, 14(2), 163-171.
- Glasson, E. J., Sullivan, S. G., Hussain, R., Petterson, B. A., Montgomery, P. D., & Bittles, A. H. (2002). The changing survival profile of people with Down's syndrome: implications for genetic counselling. Clinical genetics, 62(5), 390-393.
- Heslop, P., Blair, P. S., Fleming, P., Hoghton, M., Marriott, A., & Russ, L. (2014). The Confidential Inquiry into premature deaths of people with intellectual disabilities in the UK: a population-based study. The Lancet, 383(9920), 889-895.
- Hosking, F. J., Carey, I. M., Shah, S. M., Harris, T., DeWilde, S., Beighton, C., & Cook, D. G. (2016). Mortality among adults with intellectual disability in England: comparisons with the general population. American Journal of Public Health, 106(8), 1483-1490.