



Research Article - (2018) Volume 3, Issue 1
Study of New onset Diabetes Mellitus in Acute Coronary Syndrome Patients
2Kjk Hospital, Trivandrum, India
3Gajra Raja Medical College Gwalior, India
Received Date: Jun 13, 2018 / Accepted Date: May 27, 2018 / Published Date: Jun 15, 2018
Copyright: ©Ashish singhal, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: There is limited information on the incidence of diabetes despite INDIA being the Global capital for Diabetes. Though much of data is available in patients already diagnosed with diabetes but data regarding the new onset diabetes in the subset of Acute coronary syndrome (ACS) is very limited.
Materials and methods: This was a Cohort study in which 200 consecutive ACS patients were included. Lab data about their FBS; PPBS; Lipid profile & Hba1c, BMI, BP and their clinical status was collected at the time of admission, after discharge at 2 weeks, 6 weeks & 3,6 & 12 months post ACS.
Results: In study 85% were males. Mean age was 56 years. Prevalence of various atherosclerotic risk factors in study population matched the regional prevalence of them. 20% (n=40) developed New onset diabetes (NOD), 2.5% (n=5) developed Impaired fasting Glucose, 6% (n=12) developed Impaired glucose tolerance in and 1.5% (n=3) developed both Impaired fasting glucose and Impaired Glucose tolerance over a follow up period of 1 year. MACE rates & Revascularisation rates were significantly higher in NOD population. NOD patients had significantly higher BMI, waist circumference, BP, TG, LDL and Low HDL. NOD patients were on Higher dosage of statins, diuretics and Beta blockers.
Conclusion: The study highlights two important things, first incidence of new onset diabetes in acute coronary syndrome patients is High, second new onset diabetes has a significant impact on the clinical outcome of ACS patients
Keywords
Acute coronary syndrome, New onset diabetes, incidence
Introduction
Diabetes Mellitus The mounting incidence and prevalence of type 2 diabetes, driven by increasing population age, obesity, and physical inactivity, compound this high global burden as does the increasing longevity of patients with diabetes.
India has more diabetics than any other country in the world, according to the International Diabetes Foundation. The disease currently affects more than 62 million Indians, which is more than 7.1% of India’s adult Population [1].
CAD & Diabetes Mellitus
Those with diabetes have two- to four-fold higher risk of developing coronary disease than people without diabetes, and CVD accounts for an overwhelming 65-75 per cent of deaths in people with diabetes [2].
The risk of New Onset Diabetes (NOD) is associated with many factors like diet, physical activity, medical conditions like hypothyroidism, CKD, family history, smoking, dyslipidemia, hypertension and with a wide variety of drugs including statins, thiazide diuretics, beta-blockers, glucocorticoids, niacin etc [3].
Among patients with multivessel CAD and preserved left ventricular ejection fraction, whatever the treatment regimen is, rates of overall and cardiac-related deaths is high among diabetic compared with non-diabetic patients [4].
Though much of data is available about the patients with pre-existing diabetes but data about new onset diabetes in ACS patients and its impact on their outcomes is very limited. This study gives an insight into the subject concerned.
Materials and Methods
This is a Cohort study. 200 consecutive ACS patients in department of cardiology, Government Medical College, Trivandrum are taken up for study after having proper written and informed consent. A brief history including chief complaints; history of presenting & past illness; personal & family history; drug & addiction history was taken. Clinical data like BMI, waist circumference, BP & lab data i.e. FBS; PPBS; Lipid profile; Hba1c & drugs presription were studied at the time of admission, after discharge at 2 weeks, 6 weeks, 3,6 & 12 months post ACS. Clinical outcomes were also assessed at every visit including MACE and revascularization events.
New onset diabetes mellitus was detected as per standard diagnostic criteria with one or more of the below:
1. Fasting plasma glucose >=126 mg/dl
2. Post prandial plasma glucose >=200 mg/dl
3. Hba1c > = 6.5%
After collecting data the patients in study sample who developed new onset diabetes mellitus (n=40) were compared with a randomly selected control group (n=60) of patients from the same study sample after matching their all baseline characteristics at the time of admission. These two groups are then compared with appropriate statistical tests.
Sample size Calculation
|
Population size(for finite population correction factor or fpc)(N): |
1000000 |
|
Hypothesized % frequency of outcome factor in the population (p): |
7.2%+/-1 |
|
Confidence limits as % of 100(absolute +/- %)(d): |
1% |
|
Design effect (for cluster surveys-DEFF): |
1 |
Sample Size(n) for Various Confidence Levels
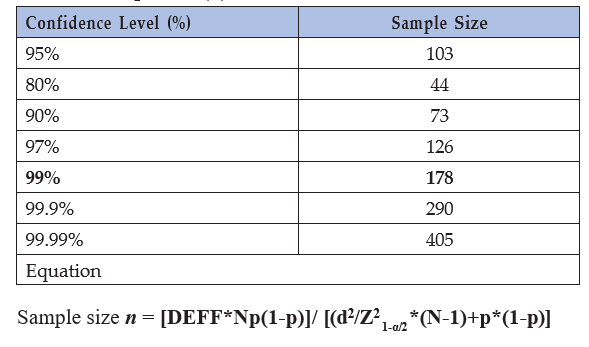
Hypothesized frequency of 7.2% is taken from the Korean study which calculated the incidence of new onset diabetes in post PTCA patients
Inclusion Criteria
Any ACS Patient as per standard defined criteria mentioned below: Patients with acute onset ischemic symptoms along with ECG showing significant ST-T changes with or without cardiac biomarkers like CPK-MB & Troponins above the Upper normal limits as per Lab.
Exclusion Criteria
• Patients diagnosed to have diabetes mellitus at time of admission (As per standard definition: Hba1c > 6.5, FBS>126 mg/dl, 2 hour PPBS>200 mg/dl or RBS>200 mg/dl with symptoms consistent with diabetes mellitus)
• Patients who are already diagnosed or on treatment for diabetes mellitus.
• Patients who do not give consent for participation in the study.
Results
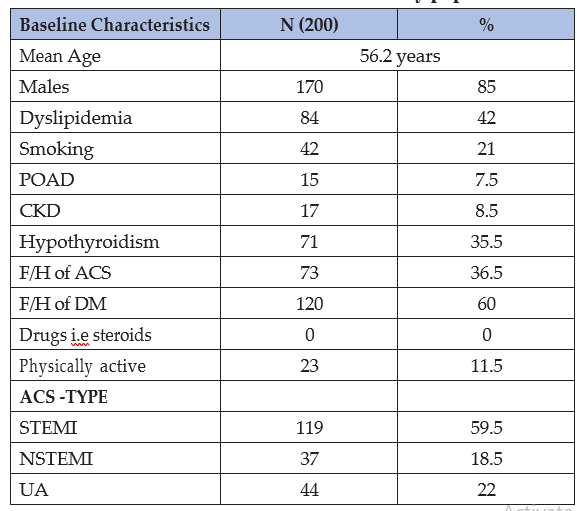
The baseline characteristics of study population were comparable to prevalent characteristics of ACS patients quoted in several studies of the region. (Table 1)
Table 1: Baseline characteristics of study population
After collecting data a Control group was made for analytical purpose from the study population itself. Control group was formed from the remaining patients (n=140) who did not develop NOD, IFG or IGT till last follow up of 1 year. 60 patients out of 140 patients were selected randomly after their baseline characteristics were matched as shown in Table 3 and then comparative analysis was done.
Discussion
There is limited information on the incidence of diabetes in India. One such data source is the New Delhi Birth Cohort study, which reported an annual incidence of 1.0% for males and 0.5 % for females, even though this population was in the 4th decade of life [5].
K R Thankappan, et al. studied incidence of diabetes in 326 industrial workers in kerala. At two years follow up, 13.3 % of the 241 workers who were either normal or had pre-diabetes at baseline developed diabetes providing an incidence rate of 6.65 % per year. Among the 134 workers with normal FPG at baseline 28.4 % progressed to pre-diabetes, 5.2 % developed diabetes, and among the 107 pre-diabetics, 23.4 % developed diabetes at year two. The odds of progressing to diabetes from pre-diabetes were five times higher compared to those from normal FPG (OR 5.53; CI 2.28–13.37) [6].
In our study New onset diabetes was detected in 20% (n=40) , Impaired Fasting Glucose in 2.5% (n=5) , Impaired glucose tolerance in 6% (n=12) and both Impaired fasting glucose and Impired Glucose tolerance in 1.5% (n=3) over a follow up period of 1 year out of total study population of 200. (Table 2)
Table 2 : Number of Patients developed deranged Blood sugars and Hba1c in study population over one year
|
Impaired Blood Sugar Category |
No. |
% |
|
NOD |
40 |
20% |
|
IFG |
5 |
2.50% |
|
IGT |
12 |
6% |
|
IFG+IGT |
3 |
1.50% |
The calculated incidence rate in our study is 0.2 per person per year, this is very high in comparison to available data on incidence of diabetes. This can be explained on the fact that the study population was selected from Acute coronary syndrome patients which itself is an absolute marker of presence of atherosclerotic vascular disease. Multiple comorbidities like dyslipidemia, obesity, Hypertension, smoking and genetic predisposition puts these patients at higher risk of coronary events as well as make them prone to develop new onset diabetes. Not only the comorbidities the presence of statins and beta blockers along with thiazide diuretics also adds fuel to fire in new onset diabetes in these group of patients.
Kyeong-Hyeon Chun et al studied around 6,777 patients who underwent DES implantation between January 2006 and December 2011. At a median follow-up of 3.9 years, new onset diabetes occurred in 436 (7.2%) patients. This was a comparative and background study for our study but the incidence of new onset diabetes is far below than our study re-iterating the fact our countrymen are more predisposed to this illness [7].
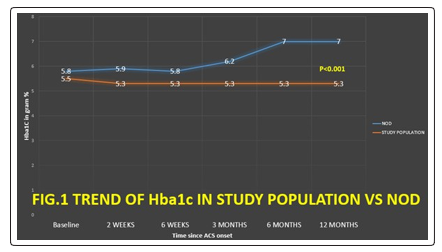
Another important data we got from our study While analyzing the time trends of Blood sugar & Hba1c levels of patients , that most of the patients (n=37; 92.5%) who developed new onset diabetes in the first 6 month duration after the acute coronary event (Fig. 1). Thus implicating that the latent diabetes gets clinically revealed very rapidly after occurrence of ACS. Our study corroborates the finding of aggressive treatment required for new onset diabetes 3 months after renal transplantation [8].
As compared to control group the NOD patients had significantly Higher BMI, waist circumference, BP, Triglyceride level, LDL level, Low HDL level. (Table 3).
The significant difference in BMI & waist circumference suggests that these patients gained weight rapidly despite of repeated advisory of active lifestyle and healthy diet. In (EPIC)–Potsdam Study which included 7720 men and 10 371 women founded that RR estimates in men and women were slightly higher for each unit of BMI gain between ages 25 and 40 y [men: 1.25 (95% CI: 1.21, 1.30); women: 1.24 (1.20, 1.27)] than between ages 40 and 55 y [men: 1.13 (1.10, 1.16); women: 1.11 (1.08, 1.14)] [9].
Our results support the hypothesis that elevated BP is associated with increased risk of diabetes and this corroborates with the largest evidence available yet in the metanalysis performed in 2015 by Connor etal. In this metanalysis a cohort of 4.1 million adults, free of diabetes and cardiovascular disease, was identified using validated linked electronic health records. Among the overall cohort, 20 mm Hg higher SBP and 10 mm Hg higher diastolic BP were associated with a 58% and a 52% higher risk of new-onset diabetes (hazard ratio: 1.58; 95% confidence interval [CI]: 1.56 to 1.59; and hazard ratio: 1.52; 95% confidence interval: 1.51 to 1.54), respectively. Estimates were similar even after excluding individuals prescribed antihypertensive or lipid-lowering therapies [10].
Our study clearly shows how the deranged Triglyceride, LDL & HDL levels influence the glucose homeostasis. This leads to insulin resistance, depletion of beta cells & raised blood glucose levels which manifests as diabetes. Framingham offspring study and ASCOT BPLA study founded that low HDL and high Triglyceride had significant power in prediction of new onset diabetes [11,12].
Drugs & NOD
NOD patients were on higher dosage of Beta blockers and statins also more number of NOD patients were on diuretics (Table 3 & Table 4). Table 3: Baseline characteristics of NOD & Control Group
|
|
NOD (N=40) |
Control (N=60) |
p |
||
|
Mean |
sd |
Mean |
sd |
||
|
Age in years |
53.7 |
9.5 |
53.6 |
8.2 |
0.952 |
|
BMI |
32.3 |
2 |
30.1 |
1.3 |
0.52 |
|
Waist circumference in cm |
92.9 |
6.1 |
90 |
4.8 |
0.945 |
|
SBP |
146.5 |
18.3 |
127.8 |
11.6 |
0.481 |
|
DBP |
90.7 |
9.5 |
89.5 |
5.9 |
0.456 |
|
Hba1C |
5.8 |
0.3 |
5.5 |
0.2 |
0.436 |
|
FBS (mg/dL) |
94.4 |
10.6 |
85.8 |
11.9 |
0.542 |
|
PPBS (mg/dL) |
141.4 |
18.6 |
130.2 |
11.8 |
0.694 |
|
TG (mg/dL) |
165 |
20 |
148 |
18 |
0.439 |
|
TC (mg/dL) |
224.4 |
17 |
222.6 |
8.5 |
0.489 |
|
HDL (mg/dL) |
33.7 |
2.3 |
42.7 |
6.2 |
0.368 |
|
LDL (mg/dL) |
120.4 |
12.2 |
107 |
8.5 |
0.707 |
|
VLDL (mg/dL) |
24.1 |
2.9 |
23.9 |
6.2 |
0.9 |
|
|
NOD (N=40) |
Control (N=60) |
p |
||
|
N |
% |
N |
% |
||
|
High dose Beta Blockers (>100mg/day metoprolol or equivalent) |
6 |
15 |
28 |
46.7 |
0.001 |
|
Diuretic |
10 |
25 |
7 |
11.7 |
0.082 |
|
Statin high dose |
36 |
90 |
44 |
73.3 |
0.041 |
Table 4: Comparison of Followed up characteristics (at 1 year) in NOD vs Control population
|
|
NOD |
Control |
p-value |
||
|
Mean |
sd |
Mean |
sd |
||
|
Hba1C (%) |
7.03 |
0.24 |
5.38 |
0.2 |
<0.001 |
|
FBS (mg/dL) |
162.25 |
30.19 |
79.97 |
12.15 |
<0.001 |
|
PPBS (mg/dL) |
206.5 |
31.28 |
122.37 |
12.98 |
<0.001 |
|
BMI (kg/m2) |
33.86 |
2 |
27.74 |
1.47 |
<0.001 |
|
WAIST CIRCUMFERENCE (cm) |
98.08 |
5.27 |
87.85 |
5.28 |
<0.001 |
|
SBP (mm Hg) |
159.4 |
11.18 |
120.98 |
12.72 |
<0.001 |
|
DBP (mm Hg) |
98.13 |
5.91 |
89.55 |
5.75 |
<0.001 |
|
TG (mg/dL) |
163.38 |
21.2 |
133.48 |
18.24 |
<0.001 |
|
TC (mg/dL) |
225.8 |
13.4 |
224.7 |
8.5 |
0.633 |
|
HDL (mg/dL) |
33.75 |
2.58 |
50.43 |
5.78 |
<0.001 |
|
LDL (mg/dL) |
120.23 |
12.79 |
96.58 |
8.6 |
<0.001 |
|
VLDL (mg/dL) |
24.68 |
3.19 |
24.43 |
6.12 |
0.819 |
|
|
NOD (N=40) |
Control (N=60) |
p |
||
|
N |
% |
N |
% |
||
|
High dose Beta Blockers (>100mg/day metoprolol or equivalent) |
32 |
80 |
32 |
53 |
0.006 |
|
Diuretic |
21 |
52.5 |
7 |
11.7 |
<0.001 |
|
Statin high dose |
36 |
90 |
44 |
73.3 |
0.041 |
The mechanism underlying the small increase in new-onset T2DM in patients treated with statins is unknown. An increase in cholesterol content of pancreatic beta islet cells has been reported to decrease insulin secretion [13].
In a recently published meta-analysis of 13 statin trials with 91,140 participants, statin therapy was associated with a slightly higher incidence of new-onset T2DM (hazard ratio [HR]: 1.09, 95% confidence interval [CI]: 1.02 to 1.17 [14].
In the meta-analysis of 6 trials enrolling 55 675 patients with hypertension, β-blockers conferred a 32% increased risk of new-onset diabetes compared with placebo or non-diuretic antihypertensive agents. The risk of new-onset diabetes with β-blockers increased with duration of therapy [15].
Our study shows the combined effect of all the diabetogenic risk factors culminating into manifest diabetes after onset of ACS. Though the individual estimate of each risk factor contribution can’t be estimated in present study but their role in new onset diabetes is definitely proven. Our results have been supported and confirmed by several previous studies as mentioned above.
Comparison of Clinical Outcomes (mace) Between NOD and Controls (Table 5)
There are total 2 deaths in study population, out of which 1 was cardiac death occurred due to cardiogenic shock in NOD group and other was due to Severe Sepsis and Multi-organ dysfunction in excluded group.
Table 5: Comparison of Clinical Outcomes between Nod and Controls
|
CLINICAL EVENT |
NOD N=40 |
CONTROLS N=60 |
TOTAL EVENTS |
P-VALUE |
|
MACCE RATES |
29 |
17 |
62 |
0.00001 |
|
DEATH |
1 |
0 |
2 |
0.21 |
|
CARDIAC DEATH |
1 |
0 |
1 |
0.21 |
|
ACS |
3 |
2 |
7 |
0.34 |
|
STENT THROMBOSIS |
1 |
0 |
2 |
0.21 |
|
HOSPITALISATION DUE TO HF, CARDIOGENIC SHOCK AND ARRYTHMIA |
25 |
15 |
50 |
0.002 |
|
CVA |
0 |
0 |
1 |
1 |
|
REPEAT REVASCULARISATION |
||||
|
TLR |
2 |
1 |
5 |
0.33 |
|
TVR |
8 |
5 |
18 |
0.08 |
|
PCI FOR NEW LESIONS |
2 |
0 |
3 |
0.08 |
|
CABG |
0 |
0 |
0 |
NA |
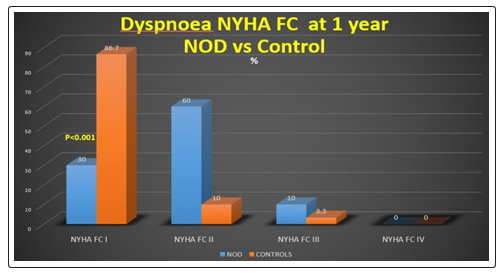
Most of the hospitalizations were due to heart failure in the study. Overall analyzing the Dyspnoea NYHA FC at the end of 1 year showed that 86.7% of control patients were in NYHA FC I whereas only 30% of NOD patients were in NYHA FC I while rest of them had worse NYHA FC which was clinically significant. (Fig. 2)
MACCE (Major adverse cardio cerebro vascular events included: Death, ACS, CVA & Hospitalisation due to Heart failure, Cardiogenic shock or arrhythmia. Overall on analysis the MACCE rates and revascularization were significantly higher in NOD population suggesting the etiological role of overall disturbed metabolic profile of these patients in the form of overweight, dyslipidemia, hypertension and deranged glucose levels culminating into a bad outcome and prognosis. The fact in our study is supported by quite a few studies [16].
On Multivariate cox-regression analysis with backward check (Table 6) we found that High BMI (HAZARD RATIO 1.172; 95% CONFIDENCE INTERVAL 1.031-1.332) & LOW HDL (HAZARD RATIO 1.161; 95% CONFIDENCE INTERVAL 1.026-1.331) are the only two variables significantly associated with New onset diabetes. However, this doesn’t means that the other variables were not contributing to the etiology of new onset diabetes rather there role was shadowed in presence of other risk factors and also the study sample was small and underpowered to detect significant predictors on multivariate analysis.
Table 6: Multivariate Analysis of Predictors of New-Onset T2DM-Cox-regression analysis with backward check
|
|
B |
SE |
Wald |
df |
Sig. |
HR |
95.0% CI for HR |
|
|
Lower |
Upper |
|||||||
|
BetaBlockers |
0.008 |
0.011 |
0.501 |
1 |
0.479 |
1.008 |
0.986 |
1.031 |
|
Diuretic |
-0.059 |
0.389 |
0.023 |
1 |
0.88 |
0.943 |
0.44 |
2.022 |
|
Statin high dose |
0.574 |
0.904 |
0.403 |
1 |
0.525 |
1.775 |
0.302 |
10.431 |
|
Statin low dose |
0.314 |
0.638 |
0.242 |
1 |
0.623 |
1.369 |
0.392 |
4.783 |
|
OUTCOME |
0.025 |
0.31 |
0.006 |
1 |
0.937 |
1.025 |
0.558 |
1.882 |
|
BMI |
0.159 |
0.065 |
5.914 |
1 |
0.015 |
1.172 |
1.031 |
1.332 |
|
WAISTCIRC. |
-0.025 |
0.052 |
0.235 |
1 |
0.628 |
0.975 |
0.881 |
1.08 |
|
SBP |
0.005 |
0.018 |
0.079 |
1 |
0.778 |
1.005 |
0.971 |
1.041 |
|
DBP |
0.036 |
0.036 |
1.031 |
1 |
0.31 |
1.037 |
0.967 |
1.112 |
|
Hba1C |
0.643 |
0.675 |
0.908 |
1 |
0.341 |
1.903 |
0.507 |
7.143 |
|
FBS |
0.008 |
0.007 |
1.293 |
1 |
0.255 |
1.008 |
0.994 |
1.022 |
|
PPBS |
0.003 |
0.006 |
0.327 |
1 |
0.567 |
1.003 |
0.992 |
1.015 |
|
TG |
-0.001 |
0.009 |
0.013 |
1 |
0.908 |
0.999 |
0.981 |
1.017 |
|
TC |
0 |
0.015 |
0 |
1 |
0.992 |
1 |
0.971 |
1.03 |
|
HDL |
-0.15 |
0.04 |
14.112 |
1 |
0.01 |
1.161 |
1.026 |
1.031 |
|
LDL |
0.013 |
0.015 |
0.732 |
1 |
0.392 |
1.013 |
0.984 |
1.042 |
|
VLDL |
0.096 |
0.068 |
2.012 |
1 |
0.156 |
1.101 |
0.964 |
1.258 |
Conclusion
It is well known that diabetes itself is hallmark of complex atherosclerotic process with varying manifestations, causing morbidity and mortality. Presence of diabetes worsens the outcomes in a Coronary artery disease patient by many times. However, the occurrence of new onset diabetes in a coronary artery disease patient has not been studied well till date. With only miniscule data available on this subject, this study is a modest attempt to quantify the new onset diabetes in coronary artery disease patients after acute coronary syndrome.
|
What is known? |
|
What this study adds? |
|
Take Home Message Early and regular screening of blood glucose of ACS patients should be done to prevent, detect and treat diabetes mellitus especially for first 6 months. Adopt healthy lifestyle, Take care of comorbidities and watch for drug (s) affect. |
References
- Indian Heart Association Why South Asians Facts.
- Waters DD, Ho JE, DeMicco DA, Breazna A, Arsenault BJ, et al. (2011) Predictors of new-onset diabetes in patients treated with atorvastatin: results from 3 large randomized clinical trials. J Am Coll Cardiol 57: 1535-1545.
- James B Meigs (2010) Epidemiology of Type 2 Diabetes and Cardiovascular Disease: Translation From Population to Prevention. Diabetes Care 33: 1865-1871.
- Kyeong-Hyeon Chun (2015) Predictors and Long-Term ClinicalOutcome of New Onset Diabetes After Percutaneous CoronaryIntervention. JACC 65.
- Huffman MD, Prabhakaran D, Osmond C, Fall CH, Tandon N, et al. (2011) Incidence of cardiovascular risk factors in an Indian urban cohort results from the New Delhibirth cohort. J Am Coll Cardiol 57: 176574.
- KR Thankappan, GK Mini, PS Sarma, RP Varma (2017) Incidence of type-2 diabetes among industrial Workers in Kerala, India. Int J Diabetes Dev Ctries 37: 280-285.
- Kyeong-Hyeon Chun (2015) Predictors and Long-Term Clinical Outcome of New Onset Diabetes After Percutaneous Coronary Intervention. JACC 65.
- Cullen TJ, McCarthy MP, Lasarev MR, Barry JM, Stadler DD (2014) Body mass index and the development of new-onset diabetes mellitus or the worsening of pre-existing diabetes mellitus in adult kidney transplant patients; J Ren Nutr 24: 116-122.
- Anja Schienkiewitz, Matthias B Schulze, Kurt Hoffmann, Anja Kroke, Heiner Boeing (2006) Body mass index history and risk of type 2 diabetes: results from the European Prospective Investigation into Cancer and Nutrition (EPIC)–Potsdam Study1,2,3. Am J Clin Nutr 84: 427-433
- Connor A Emdin, Simon G Anderson, Mark Woodward, Kazem Rahimi (2015) Usual Blood Pressure and Risk of New-Onset Diabetes, Evidence From 4.1 Million Adults and a Meta- Analysis of Prospective Studies. J Am Coll Cardiol 66: 1552- 1562.
- Peter WF Wilson, James B Meigs (2007) Lisa Sullivan, PhD; et al; Prediction of Incident Diabetes Mellitus in Middle-aged Adults The Framingham Offspring Study. Arch Intern Med 167: 1068-1074.
- Ajay K Gupta, Bjorn Dahlof, Joanna Dobson, Peter S Sever, Hans Wedel, et al. (2008) Determinants of New-Onset Diabetes Among 19,257 Hypertensive Patients Randomized in the Anglo-Scandinavian Cardiac Outcomes Trial–Blood Pressure Lowering Arm and the Relative Influence of AntihypertensiveMedication. Diabetes Care 31: 982-988.
- M Hao, JS Bogan (2009) Cholesterol regulates glucose- stimulated insulin secretion through phosphatidylinositol 4,5-biphosphate. J Biol Chem 284: 29489-29498.
- Naveed Sattar, David Preiss, Heather M Murray, Paul Welsh, Brendan M Buckley, et al. (2010) Statins and risk of incident diabetes: a collaborative meta-analysis of randomised statin trials. The Lancet 375: 735-742.
- Franz H Messerli, Sripal Bangalore, Stevo Julius (2008) Risk/ Benefit Assessment of β-Blockers and Diuretics Precludes Their Use for First-Line Therapy in Hypertension. Circulation 117: 2706-2715.
- Almgren T, Wilhelmsen L, Samuelsson O, Himmelmann A, Rosengren A, et al. (2007) Diabetes in treated hypertension is common and carries a high cardiovascular risk: results from a 28-year follow-up. J Hypertens. 25: 1311-1317.