


Research Article - (2020) Volume 5, Issue 1
Prevalence of Antibiotic-Resistant Bacteria Isolated From Infant Stools Aged Less Than 2 Years after Antibiotic Therapy Treatment
2University of Mustapha Stambouli, Faculty of Natural and Life Sciences, Department of Agronomy, Laboratory of Research on Biological Systems and Geomantic, P.O. Box 305, Mascara 29000, Algeria
Received Date: Nov 16, 2019 / Accepted Date: Dec 27, 2019 / Published Date: Jan 15, 2020
Copyright: ©Mokrani Slimane, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
65 stool samples were analyzed for insulation, identification and multiresistant bacteria becoming from infant aged less than two years of the pediatric ward of Khalil Amrane Hospital-Bejaia. The study of antibiotic administration by type, revealed that amoxicillin was the most commonly administered antibiotic with a rate of (33.33%) followed by gentamicin at (20.43%) and ampicillin at (17.20%). As well, the distribution of antibiotics administered by family and group revealed the predominance of B-Lactamines with a percentage of (72.04%) of which the group of penicillins of group A is predominant (50.54%). The identifications and antibiotic susceptibility tests of the various isolated pathogenic strains were carried out. From all samples, 35 bacterial isolates were identified by macroscopic, microscopic observations, and physiological and biochemical tests. According to which it can be seen clearly that the most frequent species isolated was Clostridium perfringens with 12 (34.28%) isolates. Followed, by Escherichia coli with 11 (31.43%) isolates. Enterobacter sp were represented by 8 (22.86%) isolates. The least frequent species was Staphylococcus aureus with 4 (11.83%) isolates. Furthermore, antibiogram method showed that all bacteria tested were multiresistant to 1 to 6 antibiotics.
Keywords
Multiresistant Bacteria, Antibiotics, Infants and Stool Samples.
Introduction
Infectious diseases are a global concern. Among the concerns raised by this issue, bacterial resistance to antibiotics requires particular attention and specific measures [1]. In the other hand, the intestinal flora or microbiota is the set of bacteria that colonizes the digestive tract. A human being harbours 1014 bacteria in his digestive tract whereas it consists of only 1013 eukaryotic cells [2-4]. Also, for many years, the digestive microbiota has been poorly or not studied, as more than 70% of the bacteria in it cannot be cultivated by conventional methods [5]. Whereas, in the fight against infectious diseases, vaccines and antibiotics are the most valuable therapeutic tools available. However, the target bacteria develop new mechanisms to become more resistant to the action of antibiotics. Here and there pathogenic strains that are resistant to them develop [6]. Furthermore, multi-resistant bacteria as strains of a bacterial species found resistant to at least two classes of antibiotics to which strains of the same species are usually susceptible. The consequences of multi-resistant bacterial infections are multiple; the severity of disease, due to the ineffectiveness of antibiotics, and the increase in mortality [7]. As given this resistance problem that accompanies the massive use of antibiotics, important scientific and economic interests have emerged for metabolites or other molecules with antibacterial or probiotic activities [8-10]. Particularly, bacteria are considered resistant or multi-resistant (MRB) when, due to the accumulation of natural or acquired resistance, they are only sensitive to a small number of antibiotics usually active in therapy. BMRs are no more pathogenic or virulent than susceptible species, but they are more difficult to treat and cause treatment failures [11]. Those MRB are primarily concerned with hospital infections; enterobacteriaceae producing extended spectrum beta-lactamases, methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci, multi-resistant Acinetobacter baumanii and multi-resistant Pseudomonas aeruginosa [12].
This study was focused on the isolation and identification of multi¬resistant bacteria isolated from hospital in Bejaia region from the stools of infants less than two years of age, who had developed diarrhea after antibiotic treatment.
Materials and Methods
Stools Sampling
65 stool samples from infants aged from 1 to 24 months were taken from Boukhalfa Hospital, Amizour-Bejaia (36°38’41.3 “N 4°53’42.0 “E). Diarrhea was observed in all infants that had previously received antibiotic treatment for different diseases. An aliquot of each stool samples equivalent to a nut, were collected sterilely and released into coproculture boxes. Data as age and antibiotic administrated were collected.
Distribution percentage of each antibiotic administered was calculated according to the following formula:
Where: ADP (%): Distribution percentage; n: number of each antibiotic administered, N: total number of antibiotics administered.
Isolation and Purification of Isolates
The isolation of different multiresistant bacteria was carried out using the traditional microbiolgy method; one tube containing nutrient broth was used to enrich E. coli and Enterobacter sp. A second tube of nutrient broth was added with a layer of vasline oil, to ensure anaerobiosis, and for the enrichment of Clostridium peringens. Also, Staphylococcus aureus were enriched in a third tube containing Giolitti Cantoni broth. The three tubes were incubated at 37°C/24h. After incubation, isolation of each bacteria was carried out on selective media corresponding to each bacteria: EMB agar for Enterobacter sp and E. coli. Chapman medium for Staphylococcus aureus; liver meat agar for Clostridium peringens. Then, isolates were purified by 2 to 3 successive inoculation on the same selective medium as that of the isolation [13].
Identification of isolated bacteria
Macroscopic Identification
The identification of pathogenic bacteria through the microscopic aspect of colonies on selective agars is an essential step for the orientation of Genera and species [14]. Pure colonies are characterized by their macroscopic aspects on the corresponding selective agars for each species.
Microscopic Identification
Microscopic identification of isolated strains is performed by Gram staining [15]. Cell shapes and their modes of association are noted as shell, bacillus, isolated grouped in two, chain or cluster [1].
Biochemical and Physiological Identification
The identification of each isolate was based on mini specific biochemical galleries for genera or species including Clostridium perfringens, E. coli, S. aureus and Enterbacter sp according to [16].
Distribution percentages of each species were calculated according to the following formula:
Where: SDP (%): species distribution percentage; m: number of isolates of each species, M: total number of isolates bacteria.
Antibiogram
Antibiogram Standardization
Bacterial concentration inocula of each isolate were determined in order to perform the antibiogram technique. Bacterial suspensions were prepared in saline buffer solution and the standardized concentrations used were 108 CFU/ml for Gram-positive (S. aureus) bacteria and 107 CFU/ml for Gram-negative bacteria (E. coli and Enterobacter sp) equivalent to standard 0.5 McFarland. Except for Clostridium perfringens consisting of concentration of 109 CFU/ ml [17].
Antibiogram Technique
The antibiotic susceptibility test was performed according to the recommendations of the Antibiogram Committee of the French Society of Microbiology [18]. The method consists of inoculum seeding of each bacterial isolate on MuÃÂ??ller Hinton medium. Inoculation was carried out by the swabbing method on the howl agar surface of the Petri plates. This operation was repeated three times by turning by turning the petri dishes by an angle of 60°. Discs of antibiotics were then placed on the surface of the agar. After incubation at 37°C/24h the diameters of the inhibition zones were measured [19].
Resistance percentages of each species against antibiotics ware calculated according to the following formula:
Where: RP: Resistance percentage; l: number of resistant isolates for each species,
L: total number of isolated bacteria for each species.
Statistical Analysis
Resistance percentages (RP) of each species for antibiotics group were compared by comparison test of two proportions using STATISTICA 5.0.
Results
Frequency of Antibiotics Administered
The study of antibiotic administration by type revealed that amoxicillin was the most commonly prescribed with a percentage of 33.33% followed by gentamicin at 20.43% and ampicillin at 17.20%. The lowest administration percentages noted were for colistin and oxacillin at 1%; cefotaxime and cefatriaxone at 5% (Figure 1).The study of antibiotic administration by family and group revealed the predominance of B-Lactamines with a percentage of (72.04%) of which the group a penicillins group was predominant (50.54%). Followed, by the family of aminosides with (20.43%). aminosides avec (20,43 %).des aminosides avec (20,43 %).
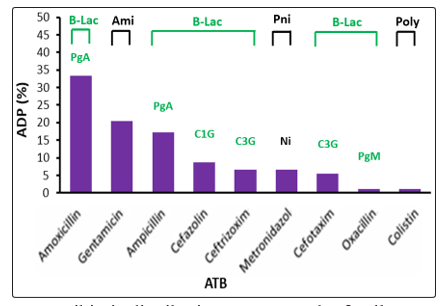
Figure 1: Antibiotic distribution percentage by family, group and type
(ADP: distribution percentage, ATB: antibiotic). B-Lac: Beta-Lactamine; Poly: polymixin; Np: nitriated products; Am: Aminosides; PgA: Group A penicillins, PgM: Group M penicillins; C1G: 1st generation cephalosporins; C3G: 3rd generation cephalosporins; Ni: Nitro-imidazoles A
Identification of Isolated Strains
Macroscopic and Microscopic Identification
Isolation on different selective media allowed 35 bacterial isolates to four species. The macroscopic and microscopic characteristic aspects of the colonies of each species are grouped in Table 1.
Table 1: Macroscopic and Microscopic Identification of Isolated Bacteria
|
ID |
A |
B |
C |
D |
|
Mac |
1-2 mm diameter creamy opac golden-yellow |
black; large colonies |
small flat green metal shine |
medium bulging mucoids |
|
Mic |
Gram positive ; cocci; grape bunches and/or isolated and/or pairs and/or short chain |
Gram positive ; bacilli |
Gram negative; coccobacilli |
Gram negative; bacilli |
ID: identification, Mac: macroscopic identification; Mic: macroscopic identification; A: Staphylococcus aureus; B: Clostridium perfringens;
C: E. coli; D: Enterobacter sp.
Biochemical and physiological identification
The identification of each species was confirmed by mini biochemical galleries regrouping specific tests for each species. S. aureus isolates produced coagulase, DNAase and catalase enzymes. Also, C. perfringens was characterized by particularly motility; growth at 44°C and formation of subterminal ovoid spore formation. Also, E. coli isolates were determined by growth at 44°C and indol production. Whereas, Enterobater sp isolates were identified by characteristics test like lactose assimilation; indole production.
Table 2: Biochemical and physiological identification of isolated bacteria
|
Species/test |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
|
S. aureus |
+ |
+ |
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. perfringens |
|
|
+ |
+ |
+ |
+ |
+ |
|
|
|
|
|
|
|
|
|
sos |
|
E. coli |
|
|
|
|
|
|
|
+ |
+ |
|
|
|
|
|
|
|
|
|
Enterobater sp |
|
|
|
|
- |
- |
+ |
|
+ |
+ |
+ |
+ |
+ |
- |
+ |
+ |
|
+ positive reaction; - : negative reaction; 1. coagulase; 2. DNAase; 3. catalase; 4. growth at 50°C; 5. Gas production; 6. H2S production;
7. motility; 8. growth at 44°C; 9. indole production; 10. Urea production, 11. TDA (Tryptophan deaminase); 12. Citrate assimilation; 13. VP (Voges proskaer) 14. RM (methyl red); 15. Glucose assimilation; 16. Lactose assimilation; 17. sos: subterminal ovoid spore.
The results of identification are summarized in Table 3.
Table 3: Identification of Bacterial Isolates
|
Code |
Species |
Code |
Species |
|
P1 |
Staphylococcus aureus |
P19 |
Clostridium perfringens |
|
P2 |
Staphylococcus aureus |
P20 |
Clostridium perfringens |
|
P3 |
Staphylococcus aureus |
P21 |
Clostridium perfringens |
|
P4 |
Staphylococcus aureus |
P22 |
Clostridium perfringens |
|
P5 |
Enterobacter sp |
P23 |
Clostridium perfringens |
|
P6 |
Enterobacter sp |
P24 |
Clostridium perfringens |
|
P7 |
Enterobacter sp |
P25 |
Escherichia coli |
|
P8 |
Enterobacter sp |
P26 |
Escherichia coli |
|
P9 |
Enterobacter sp |
P27 |
Escherichia coli |
|
P10 |
Enterobacter sp |
P28 |
Escherichia coli |
|
P11 |
Enterobacter sp |
P29 |
Escherichia coli |
|
P12 |
Enterobacter sp |
P30 |
Escherichia coli |
|
P13 |
Clostridium perfringens |
P31 |
Escherichia coli |
|
P14 |
Clostridium perfringens |
P32 |
Escherichia coli |
|
P15 |
Clostridium perfringens |
P33 |
Escherichia coli |
|
P16 |
Clostridium perfringens |
P34 |
Escherichia coli |
|
P17 |
Clostridium perfringens |
P35 |
Escherichia coli |
|
P18 |
Clostridium perfringens |
|
|
According to the identification results, it can be seen clearly that the most frequent species isolated was Clostridium perfringens with 12 (34.28%) isolates. Followed, by Escherichia coli with 11 (31.43%) isolates. Enterobacter sp were represented by 8 (22.86%) isolates. The least frequent species was Staphylococcus aureus with 4 (11.83%) isolates (Figure 2).
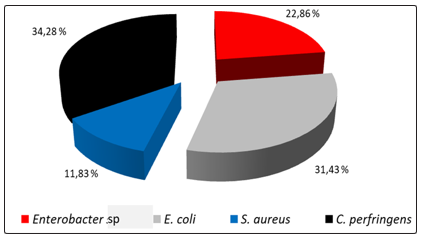
Figure 2: Species Distribution Percentage (SDP) of the Isolated Bacteria by Genera and Species
Antibiogram
The results of the antibiogram revealed that resistance varied according to antibiotic and the bacterial species. Also, multi resistance of different isolates resulted in variable inhibition zones (Figure 3).
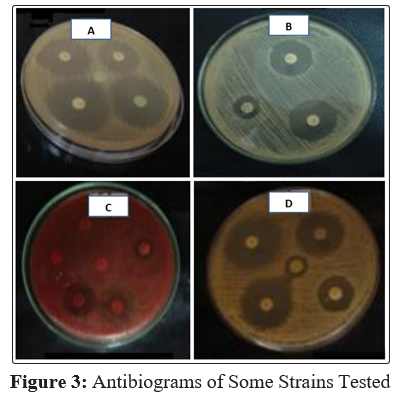
(A: P10 Enterobacter sp; B: P2 S. aureus; C: P13 C. perfringens and D: P33 E. coli).
Antibiogram of S. aureus
In this study we observed 100% resistance to penicillin, followed by cephotaxime and cephoxitine for 25% resistance each. All strains were not resistance to erythromycin, vancomycin, gentamycin and chloramphenicol (Figure 4)
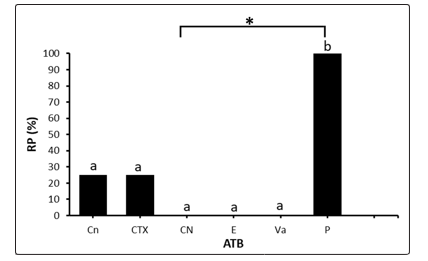
Figure 4: Resistance Percentage of S. aureus Strains
(PR: percentage resistance; E: Erythromycin; Va: Vancomycin; Cn: cefoxitin; CN: gentamycin; CTX: cefotaxim; P: Penicillin and C: Chloramphenicol). Bars designated by the same lowercase letter are statistically identical (P>0.05); *: significant difference.
Antibiogram of C. perfringens
The Clostridium perfringens strains showed 100% resistance to chloramphenicol and ampicillin, 8.33% to imipenem and 6.66% to colistin (Figure 5).
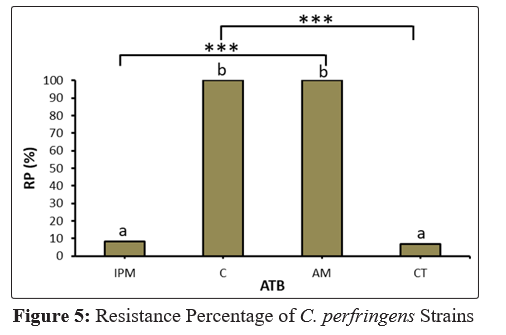
PR: percentage resistance; IPM: imipenem; C: Chloramphenicol; AM: ampicillin; CT: Colistin). Bars designated by the same lowercase letter are statistically identical (P>0.05); ***: high significant difference.
Antibiogram of E. coli
Based on antibiotic susceptibility test results, E. coli isolates showed 54.54% resistance to the combination of trimethoprim/ sulfamethoxazole antibiotics, 9.09% resistance to cefotaxime, ceftriaxone and gentamycin. All isolates were sensible to imipenem and chloramphenicol (Figure 6).
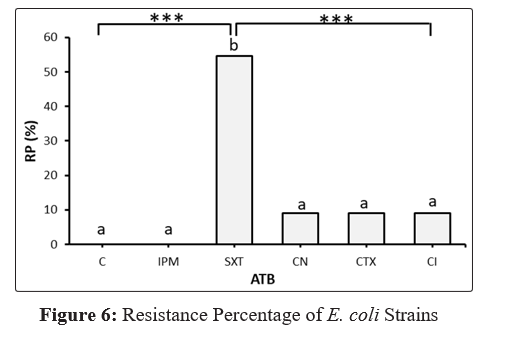
(PR: percentage resistance; NC: gentamycin; IPM: imipenem; C: Chloramphenicol; CTX: Cefotaxime; CI: ceftriaxone and SXT: trimethoprim / sulfamethoxazole). Bars designated by the same lowercase letter are statistically identical (P>0.05); ***: high significant difference.
Enterobacter sp Antibiotic Susceptibility Test
The maximum resistance rate of Enterobacter sp isolates was noted for amoxicillin/clavulanic acid of 80%, followed by amoxicillin of 70%. Resistance to cefotaxime, kanamycin and gentamycin was 40% for all the isolates tested. While, the resistance to ceftriaxon was 10%. All isolates showed no resistance to chloramphenicol, amikacin and imipenem (Figure 7).
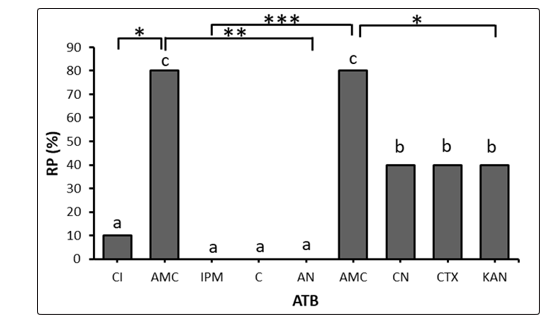
Figure 7: Resistance Percentage of Enterobacter sp Strains
(PR: resistance percentage; C: Chloramphenicol; AN: amikacin; Am: amoxylline, CI: ceftriaxon; CN: gentamycin; IPM: imipenem; CTX: Cefotaxime; KAN: kanamycin; AMC: amoxicillin/clavulanic acid). Bars designated by the same lowercase letter are statistically identical (P>0.05); *: significant difference; ** and ***: high significant difference
Discussion
The phenomenon of antibiotic resistance has become a major concern, especially with regard to nosocomial infections, following increased and uncontrolled administration, especially of broad spectrum antibiotics. Hence a major interest in the study of antibiotic resistance and the understanding of this global scourge since its origin; namely in infants of young age.
In this current study, different bacteria were isolated from infants less than two years of age after antibiotic therapy; Clostridium perfringens 12(34.28%), E. coli 11(31.43%), Staphylococcus aureus 8 (22.86%) and Enterbacter sp 4 (11.83%). According to [5], analysis of the composition of the intestinal flora in taxa (bacterial genera and/or phylogenetic groups) reveals the existence of recurrent components, found in all individuals. Three bacterial Phyla, Firmicutes, Bacteroidetes and Actinobacteria account for the largest share of the dominant faecal bacteria. In particular, the phylum of Firmicutes (Gram-positive bacteria) is still highly represented. It first includes the group called “Eubacterium rectal-Clostridium coccoides” which is often the most important representing 14 to 31% of total bacteria on average depending on the studies [20,21]. Recent studies reported by [22], stated that antibiotics are known to affect the intestinal microbial flora, and the following changes may result in diarrhea associated with antibiotics. Also, occurrence of Staphylococci in fecal samples obtained from 50 infants at 1, 2, 4 and 8 weeks of age that colonization increases by 20% in infants aged 3 days, 40% in infants aged 1 week, 52% in infants aged 2 weeks 60% in infants aged 4 weeks and 64% at 8 weeks of age [23]. Furthermore, the faecal flora of Escherichia coli was characterized in 70 Swedish children, followed during the first year of their lives. Revealing that 42% of the 70 children were colonized by Escherichia coli as early as 3 days after birth [24].
In this work, investigation of the frequency of antibiotic administration in young infants clearly revealed the dominance of antibiotics of the B-Lactamines family, particularly, group A (amoxicillin and ampicillin), followed by aminosides (gentamycin). However, adult antibiotic administration percentages are 5 to 10% for ampicillin, 10 to 25% for amoxicillin/clavulanic acid, 15 to 20% for 3rd generation cephalosporins (cefotaxime), and 2 to 5% for fluoroquinolones (pefloxacin, ofloxacin), macrolides (erythromycin) and tetracyclines (metacyline) [25].
Current findings revealed that resistance of the isolated bacteria species in infant’s stools were variable depending on antibiotic tested. Especially, since the introduction of antibiotics into the therapeutic arsenal of infectious diseases, microorganisms have developed defenses that make them insensitive to antibacterial agents. These antibiotic resistance to therapeutic doses appear more or less rapidly depending on the chemical complexity of the antibiotics and the genetic make-up of the bacteria [26]. All bacterial species or genera are concerned by the phenomenon of antibiotic resistance, which sometimes poses real therapeutic problems [27-29]. However, the misuse of these compounds, whether in the medical or agri-food sectors, has resulted in the progressive emergence of a multitude of resistance mechanisms [30]. In addition, resistant mutants spontaneously appear and are then selected. Mutants are not created directly by exposure to an antibiotic [31].
The frequency of antibiotic resistance varies from country to country. Differences in antibiotic therapy practice are undoubtedly among the possible causes of this difference [32,33].
First, the S. aureus isolates tested in this work were resistant to cefoxitin (25%); cefotaxim (25%) and penicillin (100%). Paerticularly, Staphylococcus aureus is mainly resistant to penicillin G by penicillinase production. Methicillin-resistant staphylococci are also resistant to many other antibiotics. Thus, resistance to aminosides, which concerned only streptomycin and kanamycin in the past, has been modified by the appearance of two new plasmid resistance phenotypes [34].
Second, the isolates of C. perfringens tested in this current study were resistant to chloramphenicol and ampicillin (100%); imipenem (8.33%) and colistin (6.66%). For example, [35] reported that multidrug-resistant strains of Clostridium were found only in the hospital setting in subjects treated with antibiotics. Ampicillin was the antibiotic to which most anaerobic strains were resistant; and no strain was found to be resistant to imipenem. Furthermore, significant growth in the number of ampicillin-resistant strains were observed among hospitalized patients with a recent history of unspecified antibiotic treatment [36]. A distinct correlation between antibiotic consumption and the local prevalence of resistant anaerobic fecal microorganisms has been reported for ampicillin and doxycycline [37,38]. The most important factor in Clostridium’s resistance to B-lactamines appears to be the production of B-lactamases [39,40]. These mechanisms of resistance to B-lactam antibiotics in anaerobic bacteria are developed and attributed to B-lactamases that inactivate the antibiotic by changing the number or type of penicillins binding proteins (PLP), and that affect the affinity of proteins for antibiotics; as well as the penetration of the antibiotic will be blocked in the active site through the change in the external membrane porins of the target bacteria [41-43]. Resistance to carbapenems such as imipenem is very rare [44,45].
Third, the isolates of enterobacteriaceae tested in this study are resistant to different antibiotic tested. E. coli showed multi resistant to the combination of trimethoprim/sulfamethoxazole (54.54%), and (9.09%) for cefotaxim, ceftriaxone and gentamycin. Whereas, Enterobacter sp isolates revealed resistance to amoxicillin/clavulanic acid (80%), amoxicillin (70%), and resistance of (40%) to cefotaxim, kanamycin and gentamycin, and ceftriaxon (10%). In addition, resistance of enterobacteriaceae to the combination of amoxicillin-clavulanic acid and first-generation cephalosporins (cefalotin) is between 40% and 60%, with a large number of intermediate strains probably strong producers of penicillinase. Resistance frequencies are lower for second generation cephalosporins (cefoxitin) at 23%, third generation cephalosporins at 7 to 10% [46]. Also, imipenem remains active on almost all enterobacteriaceae, despite the description of some resistant strains, either because of a significant decrease in permeability associated with cephalosporinase hyperproduction or because of carbapenemase production [47]. Furthermore, with regard to aminoglycosides, the most significant development was the emergence in 1969 of plasmid resistance to gentamicin, which was often associated with resistance to kanamycin. In the other fand, there was a rapid increase in the frequency of this resistance until 1974, followed by a decrease and stabilization around 10% [48]. Also, resistance to amikacin, which is more stable to enzymatic inactivation, remains below 5%. Resistance to sulfonamides is stable, around 35% of the strains, while trimethoprim resistance is slightly lower. For chloramphenicol, resistance is 20%, the trend is towards decreasing and then stabilizing resistance [49].
In E. coli, resistance to aminopenicillins gradually increased to more then 50%. A large part of these strains appear intermediate, even resistant, and even to the combinations of amoxicillin (or ticarcillin)-clavulanic acid due to the production of either a high level of penicillinase or TRI (TEM resistant to β-lactamase inhibitors) enzymes [50-52]. Furthermore, for other antibiotics, resistance frequencies appear relatively stable, with the exception of those for cotrimoxazole, but also quinolones where resistance has increased over the past ten years with a current frequency of more than 15% for nalidixic acid and more than 10% for ciprofloxacin [53]. Also, in E. coli resistance is frequent to ampicillin (29.8%, varying from 15.5% to 53.9% depending on the country) where the only antibiotics for which resistance is less than or equal to 10% are imipenem (0%), second and third generation cephalosporins (1 to 5%), (10%), imipenem (0%), aminosides (1 to 7%) except kanamycin [49].
Strains belonging to the genus Enterobacter almost constantly combine natural resistance with various acquired resistance traits. These are typically hospital bacteria. Natural resistances are resistance to first generation aminopenicillins and cephalosporins by cephalosporinase production [54,55]. The frequency of acquired resistances appears to be relatively lower today than in the past for Enterobacter cloacae.
Conclusion
The spread of antibacterial-resistant pathogens is one of the most serious threats to the effective treatment of a disease. This current study described isolation and identification of multi-resistant antibiotic bacteria from infant stools less than two years old, which showed the high frequency of high resistance for 3 to 6 antibiotics in bacteria belonging to C. perfringens, S. aureus, Enterobacter sp and E. coli. Antibiotic resistance is still a topical issue as this phenome is evolving more and more, causing many problems in the treatment of infections. Particularly, this study was focused on the detection of multi resistant bacteria in infant stools. But, it is important to determine the modes of delivery of these bacteria to young infants.
References
- Bousakraoui M, Zouhair S, Soraa N, Benaouda A, ZeraouLi K et al. (2017) Practical guide to pathogenic bacteria - 2017Edition.MoroccanSocietyofPediatri Infectious Disease and Vaccinology.https://pharmacie.ma/uploads/pdfs/Le-guide-pratique-des-bacteries pathogenes.pdf
- Martín R, Miquel S, Langella P, Bermúdez-Humarán LG (2014) The role of metagenomics in understanding the human microbiome in health and disease. Virulence 5: 413-423.
- Thomas S, Izard J, Walsh E, Batich K, Chongsathidkiet P et al. (2017) The host microbiome regulates and maintains human health: a primer and perspective for non-microbiologists. Cancer research 77: 1783-1812.
- Sender R, Fuchs S, Milo R (2016) Revised estimates for the number of human and bacteria cells in the body. PLoS biology 14: e1002533.
- Corthier G, Sokol H, Dore J (2007) Diversity of the microbiota and its functions. Obésité 2: 215-220.
- Piazzini C (2000) Bacteria are resistant. Network CNDP, Paris.
- Poyart C, Jardy L, Quesne G, Berche P, Trieu-Cuot P (2003) Genetic basis of antibiotic resistance in Streptococcus agalactiae strains isolated in a French hospital. Antimicrobial agents and chemotherapy 47: 794-797.
- Nettles CG, Barefoot SF (1993) Biochemical and genetic characteristics of bacteriocins of food-associated lactic acid bacteria. Journal of food Protection 56: 338-356.
- Coates A, Hu Y, Bax R, Page C (2002) The future challenges facing the development of new antimicrobial drugs. Nature Reviews Drug Discovery 1: 895.
- Davies J, Davies D (2010) Origins and evolution of antibiotic resistance. Microbiol. Mol. Biol. Rev 74: 417-433.
- C-CLIN Ouest S (2002) Risques infectieux et soins ambulatoires. Hygiène des soins infirmiers en ambulatoire 13-31.
- Giamarellou H (2006) Treatment options for multidrug-resistant bacteria. Expert Rev. Anti. Infect 601-618.
- Mokrani S, Sadoun, Djamila (2009) Ruminococcin A and its antibacterial role against multidrug-resistant strains isolated from hospitals in the Bejaia region, University of Béjaia, Algeria p 01-152.
- Singh OV (2017) Food-borne pathogens and Antibiotic resistance. Wiley Blackwell. Published by John Wiley and sons, Inc, Hoboken, New Jersey.
- Gram C (1884) The Differential Staining of Schizomycetes in Tissue Sections and in Dried Preparations. Fortschitte der Medicin. 2:185-189.
- Bergey’s M, Garriti GM, Bell JA, Timothy GL (2008) Taxonomie outline of the prokaryotes: Bergeys manual of systematic bacteriology. Ed. Springer, New York.
- CA-SFM: Antibiogram Committee of the French Society for Microbiology 2003 (2005) Special issue of the SFM, http:// www.sfm.asso.fr/
- CA-SFM: Antibiotic Committee of the French Society of Microbiology (2009) Special Issue Release SFM,https://www.sfm-microbiologie.org/wp-content/ uploads/2019/02/CASFM2019_V1.0.pdf
- Darghout S, Metheni A (2016) Morphological, biochemical and mutagenesis characterization of Pseudomonas aeruginosa strains in the Constantine region. Master memory. University of Constantine p 01-58.
- Sghir A, Gramet G, Suau A, Rochet V, Pochart P et al. (2000) Quantification of bacterial groups within human fecal flora by oligonucleotide probe hybridization. Appl Environ Microbiol 66: 2263-6.
- Rigottier-Gois L, Le Bourhis AG, Geneviève G, Rochet V, Doré J (2003) Fluorescent hybridisation combined with flow cytometry and hybridisation of total RNA to analyse the composition of microbial communities in human faeces using 16S rRNA probes. FEMS Microbiology Ecology 43: 237-45.
- De la Cochetiere MF, Durand T, Lepage P, Bourreille A, Galmiche JP et al. (2005) Resilience of the Dominant Human Fecal Microbiota upon Short-Course Antibiotic Challenge. American Society for Microbiolog 43: 5588-5592.
- Lindberg E, Adlerberth I, Hesselmar B, Saalman R, Strannegård et al. (2004) High Rate of Transfer of Staphylococcus aureus from Parental Skin to Infant Gut Flora. American Society for Microbiology 42: 530-534.
- Nowrouzian F, Hesselmar B, Saalman R, Strannegard IL, Åberg N et al. (2003) Escherichia coli in Infants’ Intestinal Microflora: Colonization Rate, Strain Turnover, and Virulence Gene Carriage. International Pediatric Research Foundation, Inc 54: 8-14.
- Bartlett JG (2002) Antibiotic-associated diarrhea. N Eng J Med 9: 346334.
- Rios AC, Moutinho CG, Pinto FC, Del Fiol FS, Jozala A et al. (2016) Alternatives to overcoming bacterial resistances: state-of-the-art. Microbiological research 191: 51-80.
- Martinez JL, Fajardo A, Garmendia L, Hernandez A, Linares JF et al. (2008) A global view of antibiotic resistance. FEMS microbiology reviews 33: 44-65.
- Gootz TD (2010) The global problem of antibiotic resistance. Critical Reviews™ in Immunology, 30: 79-93.
- Li B, Webster TJ (2018) Bacteria antibiotic resistance: New challenges and opportunities for implant-associated orthopedic infections. Journal of Orthopaedic Research® 36: 22-32.
- Roy D (2000) Identification et caractérisation de la région variable des intégrans de classe I identifiés chez différents isolats cliniques à Gram-négatif et caractérisation du mécanisme de résistance aux B-lactamines chez un isolat de Salmonella spp. Isolé au Québec. Thèse de doctorat, université de Laval, Canada.
- Prescott LM, Harley JP, Klein DA (2003) Microbiologe. De Boeck and Larcier - Bruxelles.
- Fomsgaard, A., Hoiby, N., Friis, H, Gahrn-Hansen B, Kolmos HJJ, et al. (1995) Prevalence and antibiotic sensitivity of Danish versus other European bacterial isolates from intensive and hematology oncology units. Eur. J. Clin. Microb. Infect. Dis. 14: 275-281.
- Okeke IN, Edelman R (2001) Dissemination of antibiotic-resistant bacteria across geographic borders. Clinical infectious diseases 33: 364-369.
- Corne P (2004) Staphylococcus aureus in an intensive care unit: genetic, phenotypic and epidemiological study. Doctoral thesis, University of Montpellier, France p1-174.
- Stark CA, Edlund C, Sjostedt S, Kristensen G, Nord CE (1993) Antimicrobial Resistance in Human Oral and Intestinal Anaerobic Microfloras. American Society for Microbiology 37: 1665-1669.
- Levy SB, Marshall B, Schluederberg S, Rowse D, Davis J(1988) High frequency of antimicrobial resistance in human fecal flora. Antimicrob. Agents Chemother 32: 1801-1806.
- Kling PA, Ostensson R, Granstrom S, Burman LG (1989) A 7-year survey of drug resistance in aerobic and anaerobic fecal bacteria of surgical inpatients: clinical relevance and relation to local antibiotic consumption. Scand J Infect. Dis 21: 589-596.
- WHO: World Health Organization (2018) Antimicrobial resistance and primary health care: brief (No. WHO/HIS/ SDS/2018.57).
- Nord CE, Hedberg M (1990) Resistance to beta-lactam antibiotics in anaerobic bacteria. Rev. Infect. Dis. 12: 231-234.
- Bourgeois S, Laham A, Besnard M, Andremont A, Fattal E (2005) In vitro and in vivo evaluation of pectin beads for the colon delivery of β-lactamases. Journal of drug targeting 13: 277-284.
- Finegold SM (1989) Mechanisms of resistance in anaerobes and new developments in testing. Diagn. Microbiol. Infect. Dis 12: 117-120.
- Munita JM, Arias CA (2016) Mechanisms of antibiotic resistance. Microbiology spectrum 4: 1-37.
- Kapoor G, Saigal S, Elongavan A (2017) Action and resistance mechanisms of antibiotics: A guide for clinicians. Journal of anaesthesiology, clinical pharmacology 33: 300.
- Hedberg M, Edlund C, Lindquist L, Rylander M, Nord CE (1992) Purification and characterisation of an imipenem hydrolysing metallo-betalactamase from Bacteroides fragilis.J. Antimicrob. Chemother 29: 105-113.
- Jamal W, Shahin M, Rotimi VO (2010) Surveillance and trends of antimicrobial resistance among clinical isolates of anaerobes in Kuwait hospitals from 2002 to 2007. Anaerobe 16: 1-5.
- Soussy CJ (1997) Current state of antibiotic resistance. Therapeutic Medicine 3: special issue January 24-36.
- Yang Y, Wu P, Livermore DM (1990) Biochemical characterization of a Blactamase that hydrolyses penems and carbapenems from two Serratia marcescens isolates. Antimicrob Agents and Chemother 34: 755-8.
- Krause KM, Serio AW, Kane TR, Connolly LE (2016) Aminoglycosides: an overview. Cold Spring Harbor perspectives in medicine 6: a027029.
- Kahlmeter G (2003) An international survey of the antimicrobial susceptibility of pathogens from uncomplicated urinary tract infections: the ECO-SENS Project. J Antimicrob Chemother 51: 69-76.
- Oliver A, Pérez-Vázquez M, Martínez-Ferrer M, Baquero F, de Rafael L, et al. (1999) Ampicillin-sulbactam and amoxicillin-clavulanate susceptibility testing of Escherichia coli isolates with different β-lactam resistance phenotypes. Antimicrobial agents and chemotherapy 43: 862-867.
- Perez-Moreno MO, Katargina O, Pérez-Moreno M, Carulla M, Rubio C, et al. (2004) Mechanisms of reduced susceptibility to amoxycillin-clavulanic acid in Escherichia coli strains from the health region of Tortosa (Catalonia, Spain). Clinical microbiology and infection 10: 234-241.
- Canton R, Morosini MI, Martin O, De La Maza S, De La Pedrosa EGG (2008) IRT and CMT β-lactamases and inhibitor resistance. Clinical microbiology and infection 14: 53-62.
- Sirot D, Chanal C, Henquell C, Labia R, Sirot J, et al. (1994) Clinical isolates of Escherichia coli producing multiple TEM mutants resistants to B-lactamase inhibitors. J Antimicrob Chemother 33: 1117-1126.
- Bouza E, Cercenado E (2002) Klebsiella and Enterobacter:antibiotic resistance and treatment implications. Seminars inrespiratory infections 17: 215-230.
- Ruppé É, Woerther PL, Barbier F (2015) Mechanisms of antimicrobial resistance in Gram-negative bacilli. Annals of intensive care 5: 21.