

Case Report - (2025) Volume 9, Issue 2
Phonetic Piezographic Impression: A Case Report
2Head of the removable prosthodontic department at the D.C.T.C of Casablanca, Director of the national diploma of removable prosthodontics, Morocco
Received Date: Aug 01, 2025 / Accepted Date: Aug 28, 2025 / Published Date: Sep 05, 2025
Copyright: ©2025 Elmoutawakkil Nidal, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Nidal, E., Samira, B. (2025). Phonetic Piezographic Impression: A Case Report. J Oral Dent Health, 9(2), 01-06.
Abstract
In the absence of any implant-based prosthetic solution, whether for anatomical, medical, psychological, or financial reasons, piezography is ideally suited to optimize chewing, phonation, and swallowing functions, and therefore to better psychological integration of the prosthesis.
The aim of this article is to demonstrate through a case report the benefits of phonetic piezographic impression especially in resorbed mandibular ridges.
Keywords
Tourism, Asset Prices, Real Estate, Stock Market, Thailand, Foreign, Direct Investment, Exchange Rate, Economic Growth
Introduction
A slow, progressive, and unavoidable physiological condition, human aging, causes the body to weaken. All tissues are impacted, including the orofacial region.
The existence of local and/or universal diseases exacerbates this ongoing involution of structures and functions. The initiation of bone resorption phenomenon indicates that bone tissue is highly susceptible to the impacts of aging. In dentistry, treating a complete edentulous arch is difficult, particularly when bone resorption is severe. Examples of this include the maxillary and mandibular Sangiuolo Class III and, most commonly, the mandibular Sangiuolo Class IV.
Throughout the entire clinical and laboratory prosthetic process, precise and careful management is necessary for a stable prosthesis that restores the different mandatory processes (phonation, mastication, and swallowing).
In contrast to the maxilla, the mandible's broad support surface is diminished by the tongue's presence as well as resorption, which is exacerbated with age by the migration of the surrounding muscles' insertions after edentulism.
This is why piezography at the mandibular level is of interest.
The goal of piezography is to record the neutral space, which the muscles retain even after losing a tooth. According to research on neutral space registration methods, using them produces more stable dentures. Nonetheless, a few case studies have didactically demonstrated the usefulness of this piezographic registration.
Piezography, a technique used to record shapes by means of pressure, is a method for recording a patient’s denture space related to oral function. This method provides a mandibular denture with a piezographically produced lingual surface, which customizes the contour and precludes overextension. This technique involves introduction of a mouldable material into the mouth to allow unique shaping by various functional muscle forces. Speech is one function that can be employed as a selected variable using this technique [1]. This article aims to demonstrate through a clinical case the interest of piezografic impressions.
Case Report
Patient F.S, 87 years old, suffering from insulin-dependent diabetes and cardiac arrhythmia, had previously a coronary angioplasty using a stent, presented to the removable prosthesis department of the D.C.T.C of Casablanca for complete functional rehabilitation. The extraoral examination shows a concave profile and a reduction of the lower face (Figure 1).

Figure 1: Extraoral Examination
The intraoral examination reveals a toothless maxillary crest adequate in width and height (Classe I Sangiuolo). At the opposit, the mandibule is terminally resorbed (classe III) (Figure 2).
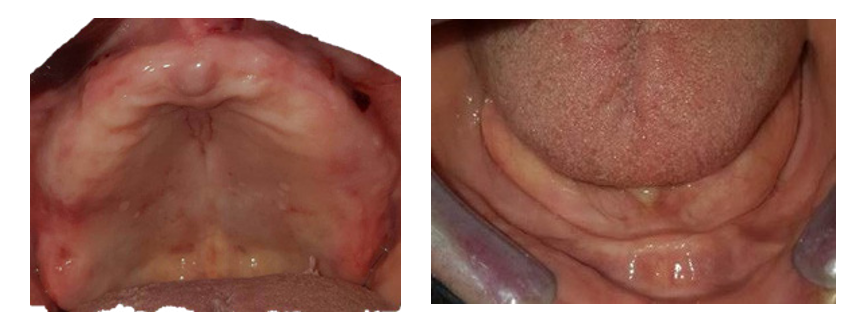
Figure 2: Intraoral Examination
The occlusal examination shows a pseudoprognathism because of the two arches' distinct resorptions: centripetal in the maxilla and centrifugal in the mandible (Figure 3).

Figure 3: Occlusal Examination

Figure 4: Radiological examination
Significant mandibular ridge resorption is seen on radiological evaluation, particularly in the posterior regions (Figure 4).
Given the patient's general condition and limited financial resources, we opted for conventional full dentures. Conventional primary impressions were made using snow-white plaster, and cast models were used to create individual trays (Figure 5).
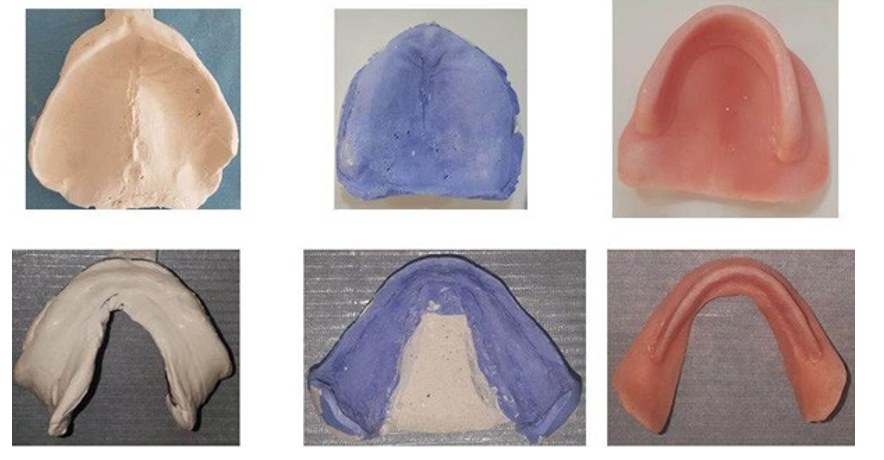
Figure 5: Primary Impressions Casts and Individual Trays
After construction of special trays, they are tried in the patient’s mouth and checked for proper extension and adaptation on the alveolar ridges. In the maxilla, the complete peripheral seal was saved by border molding using a thermoplastic paste (Kerr® paste), the final impression was then carried out using a medium- viscosity polether (Impregum®).
The phonetic piezographic mandibular impression was made as follows. After the peripheral lingual seal was registered, the individual thin tray was coated with the polysulfide on the eminences, using maximum opening, swallowing and tongue mobilization movements. Then, the patient was asked to swallow and to pronounce the posterior modelling phonemes ‘sis’ and ‘so’. The anterior sector was modeled by pronouncing the phonemes ‘se’, ‘te’, and ‘de’ and by swallowing. To have a better registration of the bearing surfaces, the entire recording was surfaced with polysulfide, performing all the movements executed in the previous steps. Thus, the piezographic impression was obtained (Figure 6). Casting this piezographic impression produced a piezographic model (Figure 7).

Figure 6: Functional Impressio
After making precision grooves in the vestibular and lingual areas of the secondary cast, two silicon keys were made, one vestibular and one lingual (Figure 8).
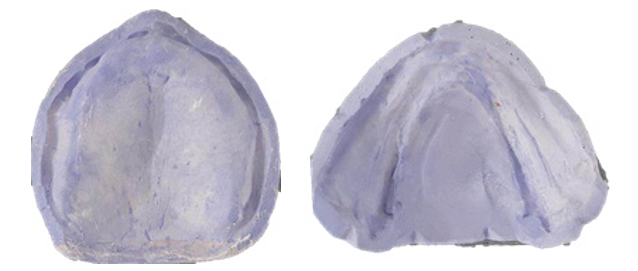
Figure 7: Secondary Plaster Casts
 |
Figure 8: Secondary Casts with Silicon Keys
These two keys delimited the piezographic prosthetic space, and the prosthetic teeth were mounted with reference to these keys. The assembly of the maxillary prosthetic teeth was then undertaken. It should be noted that when recording the occlusion, only the maxillary occlusal rim was modified, given that the occlusion plane was marked during the mandibular piezographic recording.
After fitting the teeth on wax (Figure 10), the prostheses were polymerized then placed in the mouth with a minimum of edge trimming and occlusal balancing. The patient was satisfied with the result. A post-prosthetic maintenance program was then set following consultation with the patient.

Figure 9: Occlusal Rims and Bite Registration
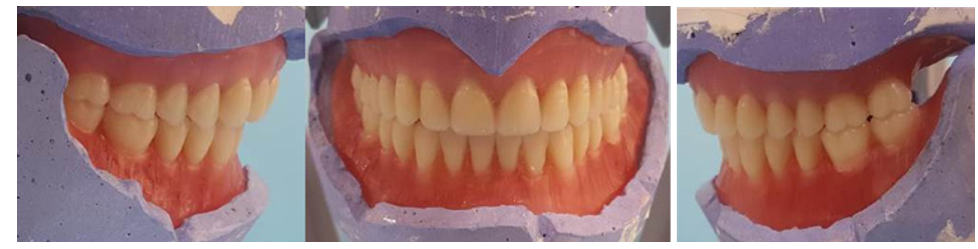
Figure 10: Teeth Mounting

Figure 11: Denture’s Insertio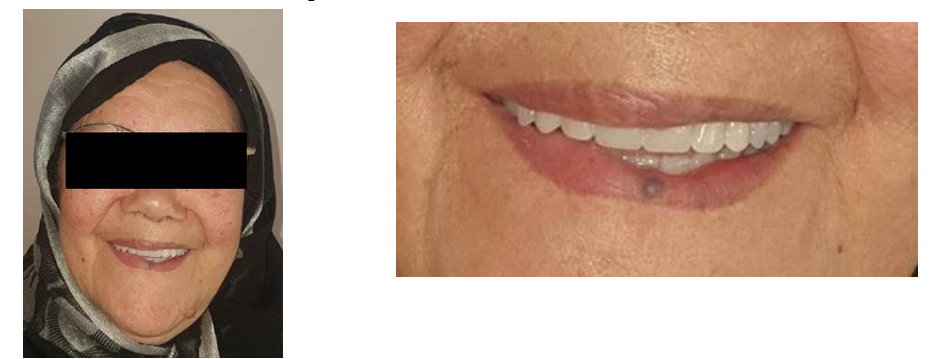
Figure 12: Improvement of The Patient's Aesthetics
Discussion
Significant bone resorption may occur in patients who have not received prosthetic restoration for a long time.
In several cases, implantology is not an option, and creating a stable and reliable denture is challenging. Piezographic techniques play a significant role in ensuring the integrity and stability of dentures in a neutral space; guiding the prosthetic construction.
The neutral space is the area between the muscles of the buccinator- labial strap and the tongue, where the forces exerted by the latter are neutralized and where the prosthesis finds the maximum of stability and retention.9 Klein defines piezography as “a technique that allows the molding of a plastic mass by intrinsic pressures, generated by the periprosthetic muscle masses [1,2].
Piezography was used to record denture space by means of the speech function of each patient. The phonemes used this technique are “sees”, “so”, “sa”, “me”, “moo”, “pe” “the”, and “te” repeatedly. Each language has special sound and the phonemes can be changed depending on the language of the patient. With pronunciation of the phonemes we can see how the superficial muscles of the face are contracted. “S” mobilizes the tongue and consequently moulds the lingual aspect of the piezography. With “ee” the modiolus and buccinators-labial clinch pull backward and the cheek moulds the buccal aspect of the register. The vowels “O” & “U” compensate the retrusive action of the sound “ee”, the lips and modiolus moulds the buccal aspect in the anterior zone. The “a” act in the lateral portion intermediately between the “ee” and “O”. The sound “M” moulds more energetically the anterior buccal aspect. The phoneme “D” in its first stage puts the tongue lingually on the alveolar ridge and the anterior upper teeth, but immediately a very quick downward movement takes place in the tongue and mandible.
When the tongue falls down, it moulds the anterior inferior lingual aspect of the register.
Klein invented the phonetic piezographic technique by pronouncing the phonemes ‘sis’ and ‘so’ in the posterior sector; then the phonemes ‘se’, ‘te’ and ‘de’ in the anterior sector.
However, the mixed technique with additional swallowing movements results in stable prostheses by stabilizing and centering the impression. Other movements can be used during this recording according to certain authors such as chewing, sucking, lip pinching, laughing and smiling. It is therefore preferable to combine all these techniques to obtain a more stable denture when performing all manducatory functions [3].
Several studies have highlighted the advantages of exploiting the neutral zone through piezography.
In 1965, Stromerg and Hichey demonstrated a better adaptation of piezographic prostheses compared to those made using conventional techniques [4]. Mubashir et al. concluded from their study that patient satisfaction with prostheses made using the neutral zone concept is higher than with conventional techniques [5].
Conclusion
Full dentures, particularly in the mandible, constitute a problem due to patients' frequent dissatisfaction with their stability. The primary worry raised is a lack of retention and stability, which leads to reduced masticatory function and, as a result, treatment failure. This issue is exacerbated in the context of mandibular ridge atrophy. As the alveolar ridge resorbs, the sites of muscle attachment are brought onto or near the crest, resulting in the elimination of the vestibular sulcus and a narrowing of the residual ridge's width. Piezographic recording determines the space to be occupied by the prosthesis by providing the necessary space for the tongue, as well as the lip and cheek muscles, in order to achieve proper balance without dislodging the prosthesis.
References
- Bekri, S., Labidi, A., Saadellaoui, I., Mabrouk, Y., & Mansour,L. (2024). Application of piezography in the treatment of total mandibular edentulism in the elderly: case report. PROTETYKA STOMATOLOGICZNA, 74(3), 255-262.
- Klein P. (1993). Piézographie et prothèse adjointe. Encycl Med Chir Stomatol, 23-325.
- Klein, P. (1985). Que peut-on attendre de la piézographie, dans la réhabilitation esthétique de l’édentation totale. Rev Fr Odonto Stomatol, 14(4), 285-90.
- Stromberg, W. R., & Hickey, J. C. (1965). Comparison of physiologically and manually formed denture bases. The Journal of Prosthetic Dentistry, 15(2), 213-226.
- SHARIF, M., AZAD, A. A., & AHMAD, S. (2013). COMPARISON OF PATIENT'S SATISFACTION LEVEL WITH COMPLETE DENTURES FABRICATED BY NEUTRAL ZONE TECHNIQUE AND CONVENTIONAL TECHNIQUE. Pakistan Oral & Dental Journal, 33(1).