
General Surgery and Clinical Medicine(GSCM)
ISSN: 2836-4961 | DOI: 10.33140/GSCM

Research Article - (2024) Volume 2, Issue 1
Pelvic Exenteration Surgery Outcomes Following Establishment of a Complex Pelvic Surgery Multidisciplinary Tertiary Unit
2Western Sydney University, Campbelltown, NSW, Australia
Received Date: Jan 08, 2024 / Accepted Date: Feb 15, 2024 / Published Date: Feb 28, 2024
Copyright: ©Â©2024 Alicia Mackowski, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Mackowski, A., Limmer, A., Lata, T. J., McCarthy, A., Gilmore, A. (2024). Pelvic Exenteration Surgery Outcomes Following Establishment of a Complex Pelvic Surgery Multidisciplinary Tertiary Unit. Gen Surgery Clin Med, 2(1), 01-07.
Abstract
Background: Pelvic exenteration surgery (PES) is a complex operation associated with significant morbidity. PES requires sub-specialised multidisciplinary input along with expertise in complex pelvic surgery and anatomy. The majority of published data on PES comes from high volume units, however there is emerging evidence of comparable short and long-term outcomes in lower volume units where dedicated multidisciplinary teams are established. This study reports outcomes of PES in a lower volume centre with a collaborative multidisciplinary surgical approach.
Methods: A retrospective review of patients who underwent PES for benign or malignant pathology at Liverpool and Macquarie University Hospitals between September 2015 and June 2022. Descriptive statistics were performed and Kaplan- Meier survival analysis for patients treated for malignancy with curative intent.
Results: A total of 67 patients undergoing pelvic exenteration were included (53.8% female; with mean age 59 years). Indications for PES were colorectal cancer (56.7%), gynaecological cancer (22.4%), other malignancy (9.0%) and complex benign pathology (11.9%). Posterior or total pelvic exenteration was performed in 88.1%. Median hospital stay was 16 days. Clavien-Dindo grade III or IV complications occurred in 34.3%. There were two post-operative deaths (3.0%; one palliative intent). For patients treated with curative intent (n=51), R0 resection margin was achieved in 92.2%, and R1 margin in 7.8%. Estimated five-year disease-free survival was 57.1%, and five-year overall survival was 65.5%.
Conclusion: Short and long-term outcomes of PES in a low volume unit with appropriate multidisciplinary expertise are comparable to published data on pelvic exenteration from higher volume units.
Keywords
Pelvic Exenteration, Pelvic Cancer, Multidisciplinary Care Team, Morbidity, Colorectal Surgery
What does this paper add to the literature?
The majority of published data on PES in Australia has come from a small number of centralised high-volume tertiary services, this paper demonstrates comparable outcomes in a lower volume centre following establishment of a PES service with suitable multidisciplinary expertise.
Introduction
Pelvic exenteration surgery (PES) involves radical en bloc resection of two or more contiguous pelvic organs, with or without resection of adjacent pelvic side wall structures, bone resection, and urinary and/or faecal diversion. Pelvic floor reconstruction with autologous tissue and/or mesh may also be performed [1].
PES is a complex operation associated with significant perioperative morbidity. PES requires sub-specialised multidisciplinary input along with expertise in complex pelvic surgery and anatomy [2].
Centralisation of PES has been shown to improve both perioperative and oncological outcomes, including R0 resection rate [3,4]. While the majority of published data on PES comes from high volume units, there is emerging evidence of comparable short and long-term outcomes in lower volume units with suitable multidisciplinary expertise [1-5].
A multidisciplinary approach to complex pelvic surgery with dedicated Complex Pelvic Surgery Multi-Disciplinary Team (MDT) was established at Liverpool Hospital in September 2015.
The group consists of dedicated radiologists and surgeons from involved disciplines including colorectal, urology, gynaecology, orthopaedics, vascular, plastic and reconstructive surgery. All patients being considered for PES were discussed at both respective oncology MDTs and the Complex Pelvic Surgery MDT.
This retrospective cohort study evaluated the short and medium-term outcomes of PES within a centre with a dedicated collaborative multidisciplinary surgical approach.
Methods
A retrospective study was conducted to evaluate the outcomes of PES at Liverpool Hospital and the affiliated Macquarie University Hospital, New South Wales. Patients were identified from a prospectively collected database. All adult patients (aged 18 years or over) who underwent PES with curative or palliative intent between September 2015 and June 2022 were included. Surgery was performed for malignant disease (including colorectal, anal, gynaecological and urological primary) or benign disease (fistula, endometriosis and pelvic sepsis).
All patients were discussed preoperatively at a Complex Pelvic Surgery MDT and cancer-specific specialised MDT, and again following PES. Demographic, oncological, operative, histopathological, morbidity and mortality data were obtained from the electronic medical record. Histopathology reports were produced by a consultant pathologist and reviewed at the MDT meeting.
Definitions
Resections were classified using PelvEx collaboration definitions as total pelvic exenteration (resection of the rectum, pelvic reproductive organs and bladder, regional lymph nodes and peritoneum), anterior pelvic exenteration (resection of the reproductive organs and bladder with preservation of the rectum) and posterior pelvic exenteration (resection of the reproductive organs and rectum with preservation of the bladder) [2]. Requirement for resection of additional bone and/or pelvic side wall structures was also recorded.
Preoperative clinical stage and postoperative pathological stage was reported as per the American Joint Committee on Cancer (AJCC) 8th edition.
Histopathological resection margins were classified as R0 (clear circumferential resection margin (CRM) of >1mm), R1 (presence of microscopic residual disease defined as CRM of ≤1mm) or R2 (presence of macroscopic residual disease).
Complications occurring within 30 days of surgery were classified using the Clavien-Dindo classification. Major complication was defined as a Clavien-Dindo grade III or IV event. Prolonged hospital length of stay was defined as greater than 14 days.
Endpoints
The primary endpoints evaluated were hospital length of stay, major complication rate within 30 days, need for reintervention (radiological or surgical), 30-day mortality, overall survival (OS) and disease-free survival (DFS).
Statistical Analysis
Data were analysed using SPSS version 27.0 (IBM Corp, Armonk, New York, USA). Descriptive statistics were performed including mean/median and range for continuous variables and frequency and percentage for categorical variables. Normality of continuous data was assessed with the Shapiro-Wilk test. Survival analysis was performed using Kaplan-Meier analysis for all patients treated for malignancy with curative intent. Ethics approval was obtained from the South Western Sydney Local Health District Human Research Ethics Committee, approval number 2022/ETH01875.
Results
Patient Characteristics
A total of 67 pelvic exenterations were performed within the study period; including 36 females (53.8%) with mean age 59 years (range 27 – 79 years). Patient baseline characteristics are shown in Table 1. Fifty-nine patients had surgery for malignant disease (88.1%), with colorectal cancer representing the most common tumour type (56.7%) followed by gynaecological cancer (22.4%). Of the malignant cases, 45 were for primary disease (76.3%) and 14 were for recurrent disease (23.7%). Treatment intent was curative in 51 patients (86.4%) and palliative in eight patients (13.6%). The median follow-up time was 26 months (range 1-80 months).
|
|
n (%) |
|
Sex |
|
|
Male |
31 (46.3) |
|
Female |
36 (53.8) |
|
Age (years)† |
58.7 (27-79) |
|
BMI (kg/m2)‡ |
25.6 (14.7-39.9) |
|
ASA (American Society of Anaesthesiologists) score |
|
|
I |
0 (0.0) |
|
II |
13 (19.4) |
|
III |
49 (73.1) |
|
IV |
5 (7.5) |
|
Pathology type |
|
|
Colorectal cancer |
38 (56.7) |
|
Gynaecological cancer |
15 (22.4) |
|
Other malignancy |
6 (9.0) |
|
Benign pathology (fistula, endometriosis) |
8 (11.9) |
|
Malignant disease |
|
|
Primary |
45 (76.3) |
|
Recurrent |
14 (23.7) |
|
Treatment intent |
|
|
Curative |
51 (86.4) |
|
Palliative |
8 (13.6) |
|
Pre-treatment AJCC stage grouping§ |
|
|
I |
2 (5.3) |
|
II |
8 (21.1) |
|
III |
18 (47.4) |
|
IV |
10 (26.3) |
|
Neoadjuvant treatment§ |
|
|
Long course chemo-radiotherapy |
25 (65.8) |
|
Short course radiotherapy |
1 (2.6) |
|
Did not receive neoadjuvant treatment |
12 (31.6) |
|
Adjuvant treatment |
|
|
Yes |
32 (54.2) |
|
No |
27 (45.8) |
†Expressed as mean (range)
‡Expressed as median (range)
§For patients with rectal adenocarcinoma (n=38)
Table 1: Patient Characteristics
Procedure Characteristics
Table 2 demonstrates perioperative data. Total and posterior exenterations were the most prevalent type of PES performed, accounting for 88.1% of cases. A high proportion of cases required either pelvic sidewall dissection and/or bone resection (62.7% and 23.9% respectively). Tissue flap reconstruction was performed in Table 2 demonstrates perioperative data. Total and posterior exenterations were the most prevalent type of PES performed, accounting for 88.1% of cases. A high proportion of cases required either pelvic sidewall dissection and/or bone resection (62.7% and 49.2% of cases with omental flap (31.3%) being performed most commonly. Median operative time was 12 hours (range 5-21 hours).
|
|
n (%) |
|
Pelvic exenteration type |
|
|
Total pelvic exenteration |
32 (47.8) |
|
Posterior pelvic exenteration |
27 (40.3) |
|
Anterior pelvic exenteration |
3 (4.5) |
|
Other pelvic exenteration |
5 (7.5) |
|
Sidewall involvement |
42 (62.7) |
|
Bone resection |
16 (23.9) |
|
Flap used |
|
|
VRAM |
5 (7.5) |
|
Omental |
21 (31.3) |
|
Other |
7 (10.4) |
|
Operative time (hours)† |
12 (5 – 21) |
|
ICU stay |
58 (86.6) |
|
Hospital length of stay (days)† |
16 (4 – 65) |
†Expressed as median (range)
Table 2: Perioperative Data
Outcomes
Median hospital length of stay was 16 days (range 5 to 65 days). Complications occurred in 70.1% of patients overall (n=47). Major complications (defined as Clavien-Dindo score of III or IV) occurred in 34.3% of patients (n=23). These included pelvic collections (11.9%), urinary tract obstruction or leak (10.4%), perineal wound failure (7.5%), pelvic bleeding (1.5%) and anastomotic leak (1.5%). Re-intervention was required in 21 patients (31.3%); radiological in 11 and surgical in 10. There were two post-operative deaths within 30 days (3.0%); one due to progressive urinary tract obstruction and associated renal failure following PES with palliative intent, the other an unexpected sudden death following discharge home of unclear cause.
Of the 51 patients treated with curative intent, an R0 resection was achieved in 92.2% of patients (n=47) and an R1 resection in 7.8% (n=4). No patients had an R2 resection. Other histological data is shown in Table 3. Over a mean follow up time of 45 months, 20 developed malignant disease recurrence (39.2%) and there were nine mortalities (17.6%). Estimated five-year DFS was 57.1% (Figure 1) and five-year OS was 65.5% (Figure 2).
|
|
n (%) |
|
Postoperative complications (Clavien-Dindo grade) |
|
|
I |
9 (13.4) |
|
II |
15 (22.4) |
|
IIIa |
8 (11.9) |
|
IIIb |
8 (11.9) |
|
IVa |
3 (4.5) |
|
IVb |
2 (3.0) |
|
V |
2 (3.0) |
|
Major complications (Clavien-Dindo grade III or IV) |
|
|
Perineal wound failure |
5 (7.5) |
|
Pelvic or intra-abdominal collection |
8 (11.9) |
|
Urinary tract obstruction, leak or fistula |
7 (10.4) |
|
Small bowel obstruction |
2 (3.0) |
|
Pelvic bleeding |
1 (1.5) |
|
Anastomotic leak |
1 (1.5) |
|
Resection margin (intent: cure) |
|
|
R0 (>1mm) |
47 (92.2) |
|
R1 (0.1-1mm) |
4 (7.8) |
|
R2 (<0.1mm) |
0 (0.0) |
|
Histological grade |
|
|
Well differentiated |
8 (13.6) |
|
Moderately differentiated |
23 (39.0) |
|
Poorly differentiated |
14 (237) |
|
Not reported |
14 (23.7) |
|
Pathological T stage† |
|
|
T0/Tis |
1 (2.6) |
|
T1 |
1 (2.6) |
|
T2 |
6 (15.8) |
|
T3 |
10 (26.3) |
|
T4a |
9 (23.7) |
|
T4b |
9 (23.7) |
|
Not reported |
2 (5.3) |
|
Pathological N stage† |
|
|
N0 |
28 (73.7) |
|
N1 |
7 (18.4) |
|
N2 |
3 (7.9) |
|
Lymph nodes† |
|
|
Total nodes (median) |
23 |
|
Positive nodes (median) |
0 |
†For patients with rectal adenocarcinoma (n=38)
Table 3: Postoperative Outcomes
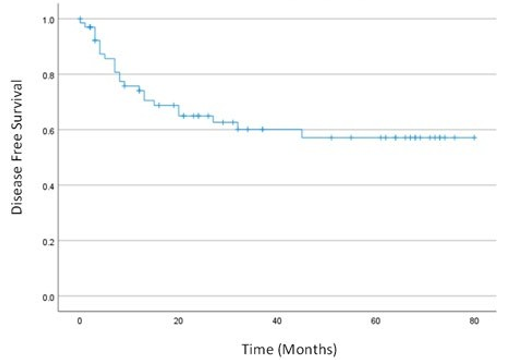
Figure 1: Kaplan-Meier estimate of disease-free survival of patients who underwent pelvic exenteration with curative intent (n=59).

Figure 2: Kaplan Meier estimate of overall survival of patients who underwent pelvic exenteration with curative intent (n=59).
Discussion
Since the establishment of a dedicated MDT for complex pelvic surgery and PES service in September 2015, a total of 67 PES procedures have been performed. The majority of procedures were for primary locally advanced colorectal cancer with high complexity of cases as evidenced by high requirement for pelvic side wall dissection, bone resection and/or flap reconstruction. Despite this patients had acceptable short-term major complication rate and mortality rate. Oncological outcomes including R0 resection rates, five-year DFS and five-year OS compare favourably with published results.
Other published studies on PES have reported comparable outcomes to those within this study. In a similar sized cohort study of 61 patients over a five-year period, Dickfos et al (Brisbane, 2018) demonstrated that radical resection pelvic surgery can be safely performed with acceptable results during the establishment phase of a dedicated tertiary service [5]. In their reviewed cases including 34 locally advanced, 25 recurrent pelvic tumours and two non-neoplastic pathologies, there was a 91.5% R0 resection rate, 52.5% overall complication rate, 26.2% rate of Clavien-Dindo IIIb complications, 3.3% 30-day mortality and 8% 12-month mortality rate [5]. Traeger et al (Adelaide, 2022) in their cohort of 113 patients (between 2008 and 2021) also demonstrated improvement in outcomes post development of a dedicated pelvic exenteration service, including higher rates of R0 resection (93.9% versus 84.2%) and lower rates of Clavien-Dindo grade IV complications (8.5 versus 31.3%) [6]. Internationally, a Danish study of 90 patients undergoing PES between 2001 and 2010 (50 for primary advanced rectal cancer and 40 for locally recurrent rectal cancer) reported R0 resection rates of 68% for primary advanced (PARC) and 38% for locally recurrent rectal cancer (LRRC), major complication rate of 62% and 60% respectively, in hospital mortality of 2.2% overall, and 5-year DFS of 46% for PARC and 17% for LRRC [7]. Oncological outcomes in this study including R0 resection rates, DFS and OS compare favourably with these published results.
Varying definitions of a major complication between studies makes it difficult to directly compare the results of this study with published results. The PelvEx Collaborative, which also defined major complications as Clavien-Dindo classification III or IV, reported that out of 1184 patients undergoing PES for locally recurrent rectal cancer, one third had a major complication and one fifth required either radiological or surgical re-intervention [8]. In comparison, this study had a smaller cohort size and included eight patients who underwent PES with palliative intent, yet had a similar major complication rate of 34.3% and rate of reintervention of 31.3%. The role of palliative PES remains reserved for select patients where the benefits of palliative resection (such as fungating tumours, disabling pain or uncontrolled fistulas) may outweigh the potential morbidity of PES [9]. Patients within this study who underwent PES with palliative intent were carefully selected and underwent a comprehensive MDT evaluation process prior to proceeding to surgery.
Clear operative margins (R0) following PES have been proven to be critical to improving survival [8-10]. In many centres, expected inability to achieve an R0 margin is regarded as a contraindication to PES [5]. Surgical technical planning is crucial to achieving clear margins and dedicated pre-operative MDT review, along with interdisciplinary communication with gastrointestinal pathologists, have been suggested as important factors in achieving these outcomes [11]. Worldwide R0 resection rates for PES are reported to be 79.9% [12]. The higher R0 resection rates within this study (92.2%) may be due to a higher proportion of primary to recurrent cancers, and the unit’s emphasis on careful pre-operative surgical planning and interdisciplinary communication during processing and assessment of pathology specimens within the Complex Pelvic Surgery MDT setting [13].
Limitations of this study include its retrospective nature, despite data being prospectively recorded, leading to potential for bias and missing data. Additionally, comparison of local outcomes to other published data is limited by the heterogeneity of the cohort of patients undergoing pelvic exenteration, including differences in patient characteristics, rates of neoadjuvant therapy, procedure performed (proportion of total, anterior and posterior exenterations, rate of bone resection and pelvic side wall dissection) and tumour histology.
In conclusion, the results of this study indicate that PES can be safely performed in a lower volume unit with a collaborative multidisciplinary team and careful pre-operative planning of surgical resection margins. Short-term outcomes are comparable to other published data with this data demonstrating favourable indicators of long-term oncological outcomes such as R0 resection rates.
Acknowledgements
A preprint of this article has been posted at https://www. researchsquare.com/article/rs-3455761/v113.
References
- Humphries, E. L., Kroon, H. M., Dudi-Venkata, N. N., Thomas, M. L., Moore, J. W., & Sammour, T. (2019). Short-and long-term outcomes of selective pelvic exenteration surgery in a low-volume specialized tertiary setting. ANZ Journal of Surgery, 89(6), E226-E230.
- "Minimum standards of pelvic exenterative practice: PelvEx Collaborative guideline." British Journal of Surgery 109, no. 12 (2022): 1251-1263.
- Jalloul, R. J., Nick, A. M., Munsell, M. F., Westin, S. N., Ramirez, P. T., Frumovitz, M., & Soliman, P. T. (2018). The influence of surgeon volume on outcomes after pelvic exenteration for a gynecologic cancer. Journal of gynecologic oncology, 29(5).
- Drami, I., Lord, A. C., Sarmah, P., Baker, R. P., Daniels, I. R., Boyle, K., ... & Jenkins, J. T. (2022). Preoperative assessment and optimisation for pelvic exenteration in locally advanced and recurrent rectal cancer: A review. European Journal of Surgical Oncology, 48(11), 2250-2257.
- Dickfos, M., Tan, S. B., Stevenson, A. R., Harris, C. A., Esler, R., Peters, M., & Taylor, D. G. (2018). Development of a pelvic exenteration service at a tertiary referral centre. ANZ Journal of Surgery, 88(7-8), E583-E588.
- Traeger, L., Bedrikovetski, S., Oehler, M. K., Cho, J., Wagstaff, M., Harbison, J., ... & Sammour, T. (2022). Shortâ?ÂÂterm outcomes following development of a dedicated pelvic exenteration service in a tertiary centre. ANZ Journal of Surgery, 92(10), 2620-2627.
- Nielsen, M. B., Rasmussen, P. C., Lindegaard, J. C., & Laurberg, S. (2012). A 10â?ÂÂyear experience of total pelvic exenteration for primary advanced and locally recurrent rectal cancer based on a prospective database. Colorectal Disease, 14(9), 1076-1083.
- "Factors affecting outcomes following pelvic exenteration for locally recurrent rectal cancer." Journal of British Surgery 105, no. 6 (2018): 650-657.
- Koh, C. E., Solomon, M. J., Brown, K. G., Austin, K., Byrne,C. M., Lee, P., & Young, J. M. (2017). The evolution of pelvic exenteration practice at a single center: lessons learned from over 500 cases. Diseases of the Colon & Rectum, 60(6), 627-635.
- Steffens, D., Solomon, M. J., Young, J. M., Koh, C., Venchiarutti, R. L., Lee, P., & Austin, K. (2018). Cohort study of long-term survival and quality of life following pelvic exenteration. BJS open, 2(5), 328-335.
- van Ramshorst GH, O’Shannassy S, Brown WE, Kench JG, Solomon MJ. A qualitative study of the development of a multidisciplinary case conference review methodology to reduce involved margins in pelvic exenteration surgery for recurrent rectal cancer. Colorectal Disease. 2018 Nov 1;20(11):1004–13.
- Kelly, M. E., Glynn, R., Aalbers, A. G., Alberda, W., Antoniou, A., Austin, K. K., ... & Winter, D. C. (2019). Surgical and Survival Outcomes Following Pelvic Exenteration for Locally Advanced Primary Rectal Cancer Results from an International Collaboration.
- Mackowski, A., Limmer, A., Lata, T. J., McCarthy, A., & Gilmore, A. (2023). Pelvic exenteration surgery outcomes following establishment of a Complex Pelvic Surgery multidisciplinary tertiary unit.