



Research Article - (2022) Volume 7, Issue 2
Hybrid Coronary Revascularization Vs Traditional Coronary Artery Bypass Graft: A Better Revascularization Modality
2Consultant interventional cardiologist Life Care Hospital, UAE
3Consultant cardiac surgeon Burjeel Hospital, UAE
Received Date: May 29, 2022 / Accepted Date: May 30, 2022 / Published Date: Jun 01, 2022
Copyright: ©Sumera Nasim, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Sumera Nasim, Khalid Galal, Waleed Shaker (2022) Hybrid Coronary Revascularization Vs Traditional Coronary Artery Bypass Graft: A Better Revascularization Modality. Cardio Open, 7(2): 248-253.
Abstract
Background: Hybrid coronary revascularization (HCR) represents a minimally invasive revascularization strategy in which the durability of the internal mammary artery to left anterior descending combined with percutaneous coronary intervention with drug eluting stents(DES)to treat remaining lesions in different coronary arteries.
Objective: To compare the complication like bleeding, nephropathy and hospital stay MACCE defined as death, stroke, myocardial infarction (MI), stroke, and repeat revascularization in hospital and one year follow up.
Methods: It was correctional study done UAE in 2018- 2019 patient with multi vessel disease who consented with insurance approval were included and decision for which patient went HCR or CABG arm by heart team, patient underwent HCR we used stage manner first LIMA – LAD followed by multi vessel PCI after 24 hrs. And patient were discharged on day 5 of admission
Results: 15 patients underwent hybrid revascularization bleeding rate was high with OR OF 1.0 with 95% C.I of 0.8-1.3 with p value of 0.03, risk of Nephropathy was higher in HCR group with odd ration 1.2 (0.6-1.5) with p value of 0.04 the mean length was 5 vs 7 Days One stroke in CABG group and MACE was HCR with ODD ratio of 1.2 (95% CI 0.8-1.5 with p value of 0.04 observed till one year no in hospital death one year follow up. Three patients died of MACE in CABG and one patient in HCR group
Keywords
Coronary Arteries Bypass Surgery, Hybrid Revascularization, Percutaneous Coronary Intervention Coronary Artery Disease, Left Internal Mammary Artery, Drug Eluting Stents
Introduction
Hybrid coronary revascularization is a treatment strategy for coronary artery disease (CAD), which offers an alternative to either traditional coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) alone. With the goal being to reduce the risk of the procedure and maximize the bene- fit, hybrid therapy capitalizes on the strengths of each approach. Since first being described by Angelina and colleagues in 1996, Hybrid coronary revascularization (HCR) procedures introduced in 2011 by the American Heart Association/American College of Cardiology Foundation updated guidelines for coronary artery bypass grafting (CABG) surgery [1,2]. The LIMA-LAD graft may be responsible for the majority of the benefit of CABG sur- gery. Whether non-LAD vessels are treated with SVGs or PCI may be less important. This is the premise on which the modern era of hybrid coronary revascularization is based. Advances in both surgical and catheter-based techniques have made hybrid therapy a more attractive option for the treatment of multi-ves- sel CAD. Using one of several minimally invasive techniques, the left anterior descending coronary artery is grafted with the left internal mammary (LIMA), and percutaneous intervention is applied to single or two vessel coronary arteries. In this ap- proach, the well-established survival benefit of the LIMA graft is capitalized upon and, being done with minimally invasive tech- niques, the increased morbidity of a full sternotomy is avoided. Additionally, the use of the LIMA graft confers benefit related to the relief of angina and long-term patency [3]. Newer gener- ation drug eluting stents have continued to improve long-term patency following PCI, to rates similar to or even surpassing that of saphenous vein grafts [4,5]. Smaller series continue to be published some study [6-8]. The advantage elderly patient spe- cially women high-risk patients (recent myocardial infarction, prior stroke, frailty, end-stage renal disease on dialysis) in whom a less invasive approach may reduce the operative time and isch- emic time [9-11].
Methodology
Total 15 patients were enrolled in a study their baseline charac- teristic collected by electronic medical records showed in Table 1 patients who underwent HCR with surgical LIMA grafting to the LAD combined with PCI to non-LAD vessels (hybrid group). The selection of HCR or CABG for revascularization was at the discretion of the clinical site cardiologist and surgeon. Comparative effectiveness trial of HCR and CABG were used in this observational study to compare clinical outcomes with Hybrid vs CABG.
Inclusion Criteria
• Elderly patient specially women
• High-risk patients (recent myocardial infarction, prior stroke, frailty, end-stage renal disease on dialysis
• Nephropathy A GFR of 50 ml/min.
• Patients who have left vein disease wit multiverse will ex- cluded for HRS
• Patient with low heart function EF as measured by echo <35%
Exclusion criteria
• Patient with concomitant left main disease with other coro- nary artery disease
• Patient with three vessel disease with long diffuse disease
• Patient have valvular heart disease with multi vessel CAD
• GFR below 30ml/min.
Statistical Analysis
Data was entered in SPSS version 24 base line characteristics were compared by using independent T test and chis-square test with p value less then<0.5 was considered significant and for outcome variable multiple variate logistic regression analysis by calculating ODD ration with 95% confidence interval with p val- ue less the 0.05 was consider significant
Intervention
HCR was defined as a planned surgical revascularization of the LAD combined with percutaneous revascularization of at least one non-LAD target and stenting of other lesions by PCI with DES was done after 24 hrs. Conventional CABG was performed by all the surgical venous and arterial conduit
Outcome Measures
The primary outcome was the incidence of MACC bleeding, ne- phropathy hospital stay defined as death, stroke, myocardial in- farction (MI), or repeat revascularization at 12 months following the initial procedure described in Table 2.
Table 2: In Hospital Outcomes Measurement in Two Groups
|
Outcome |
HRS |
CABG |
ODD ratio |
P value |
|
Bleeding |
5 |
3 |
1.2 (95% C.I 0.9-1.5) |
0.4 |
|
stroke |
no |
I |
2 (95% CI 1-3) |
0.6 |
|
Mean hospital stay |
5 days |
12 days |
OR 1.1(95% C.I0.9-1.4) |
0.01 |
|
Nephropathy |
3 |
1 |
1,0(95% C.I 0.9-1.5) |
0.03 |
|
RE MI |
3 |
1 |
1.0(95%C. I of 0.7-1,6) |
0.05 |
|
Repeat revascularization |
3 |
i |
1,2(95% C.I 0,8-1.5) |
0.04 |
|
Death |
o |
o |
NA |
NA |
Results
In HCR more elderly more patient which have high risk features like prior stroke MI in CABG group more patient with diffuse CAD more obese and more patient having peripheral vascular disease no gender difference in both groups and interesting 14 patients were Asian Expect Racial difference in CAD needs to be further trials is the contribution of genetics play a role in high CAD in UAE.
Selection of Patient in Both Groups
Heart team interventional cardiologist 2 and 2 cardiac surgeon and Cath lab nurse did selection.
HCR Group
• NSTEMI n 3 patients AWMI 2 patients
• Coronary anatomy coronary total LAD obstruction (CTO) discrete lesion LCX and RCA and EF 35% first underwent lima to LAD mini key hole surgery remain if remained sta- ble after 24 hrs., PCI of LCX and RCA was done with DES
• Mean EF 38%
• No procedure complication
• Contrast used was 70 cc patient
• Total hospital stay was 4 days
• Use of GP 11b/111a inhibitors in 3 patients
• Bleeding complication at side of PCI 3 patients
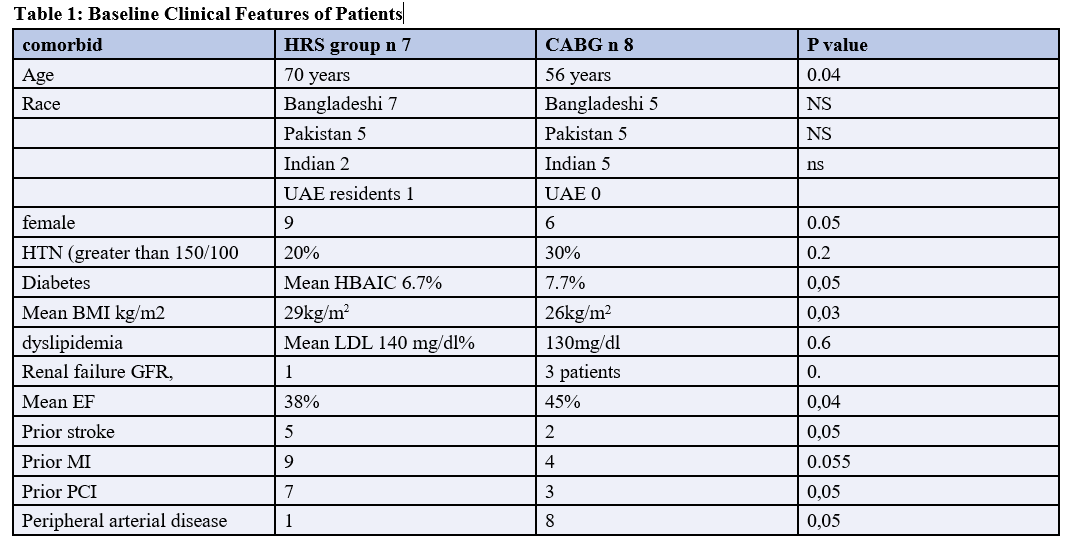
one case of HCR was described this patient presented with acute AWMI coronary anatomy showed osteal LAD with short left main underwent LIMA to LAD and long lesion with 99% RCA EF 40% procedure was uncomplicated hospital stay was 8 days Pic of HRS (123).
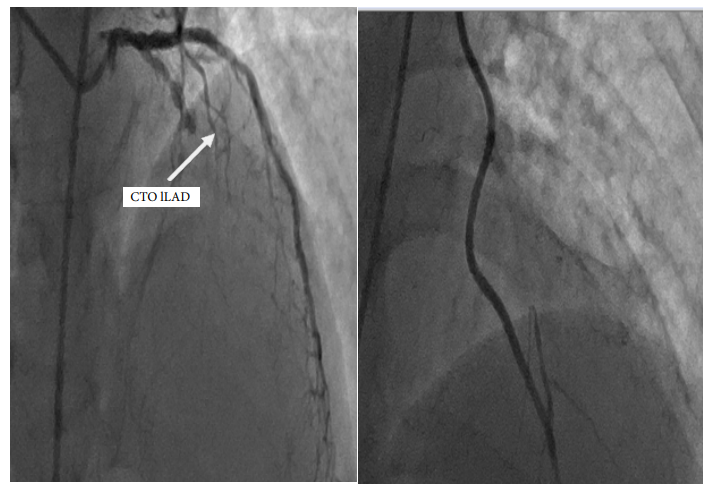
Figure 1: Pre and post procedure with LIMA CTO LAD

Figure 2: Pre and Post PCI OF RCA
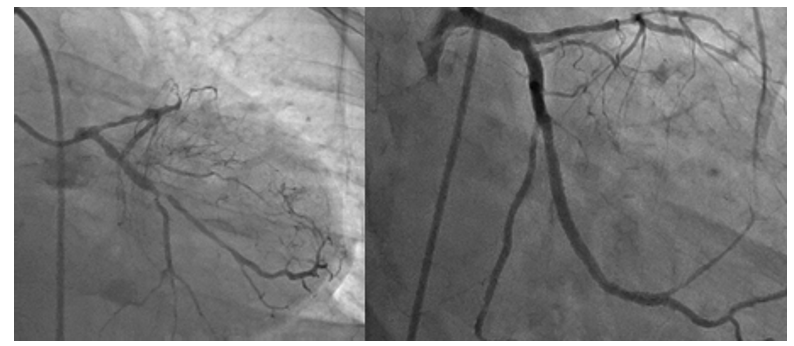
Figure 3: Pre and Post Staged PCI OF LCX
CABG Group
• 3 patients with NSTEMI 5 with unstable angina
• Coronary anatomy 3 patients had LM disease 3 had diffuse three vessel disease
• Mean EF >40
• Bleeding complications in three patients because of reopen- ing
• Use of GP11B/111a and dual ant plates in 4
• No procedure complication
• Mean Hospital stay was 12 days
In Hospital HCR group has more bleeding lesser mean hospital stay but more Repeat revascularization because of high-risk pro- file of patient acute AWMI low EF use of GPII/IIIa inhibitors. Better patient satisfaction and low cost In CABG one patient required reopening because of bleeding that lengthen mean stay one stroke no inpatient mortality one patient need repeat revas- cularization. One-year follow up 3 patients in CABG died of MACE in HCR patient 2 developed nephropathy but not requir- ing dialysis MACE in two patient required repeat revasculariza- tion one patient died of MI.
Discussion
Types of Hybrid Revascularization -stage hybrid: CABG/PCI performed in a hybrid room and in one setting, staged by min- utes or days the appeal of the latter is multifold: improved lo-gistics, lower cost, and better patient satisfaction [12,13]. As in our study, PCI before CABG allows aggressive stunting be- cause if a complication arises or PCI is unsuccessful, CABG can be performed later. Main disadvantage: Performing PCI in an unprotected environment without the benefit of a LIMA-LAD graft and later performing CABG under aggressive antiplate- let agents. PCI after CABG Avoids ant platelet-related bleed- ing complications CABG has advantage-protected environment with a LIMA-LAD graft LIMA graft patency can be verified at the time of PCI. Disadvantage: In the event of PCI complication/ failure, however, a second, higher-risk operation needs to be per- formed. The latter should be rare, however, as emergent CABG after PCI has a low incidence (<1%) Halkos, et al recently pub- lished Study what may be the largest series to date, in which 147 patients who underwent hybrid revascularization between 2003 and 2010 were compared in a 4:1 ratio to patients undergoing multi-vessel off-pump CABG [14]. According to ClinicalTrials. gov, the Hybrid Revascularization Observational Study, funded by the National Heart Lung and Blood Institute, has recently been completed [15]. The largest observational study to date,14 with planned enrollment of over 6000 patients, this study was intended to inform the design of a pivotal comparative effective- ness trial and more optimally identify the population for whom hybrid therapy may be the better option. Primary outcomes are a composite of death, stroke, MI, or repeat revascularization with follow up over 18 to 21 months. To date, no data was published from this study. As noted previously, the numerous studies that have been published to date vary in the surgical and interven- tional followed by PCI techniques, as well as patient selection, anti-platelet strategies and one-stop vs staged approaches as in our study use of gp11/111b inhibitors and antiplatelet were not started as we do LIMA to LAD with PCI, the location of the lesion in the proximal LAD has been identified as an indepen- dent risk factor for in-stent rest enosis with rates between 19% and 44% [16-18]. As occurred in our study with osteal LCX re- quiring Repeat PCI the LIMA–LAD graft has excellent patency rates, which correlates with increased event-free survival. 5-year patency rate ranges between 92% and 99% and at 10 years be- tween 95% and 98%.
With PCI, the location of the lesion in the proximal LAD has been identified as an independent risk factor for in-stent rest eno- sis with rates between 19% and 44%. The LIMA–LAD graft has excellent patency rates, which correlates with increased event- free survival. 5-year patency rate ranges between 92% and 99% and at 10 years between 95% and 98%. In control trial 104 pa- tients with average 18 months follow-up Hybrid significantly reduced in-hospital time and transfusion rate Lower MACCE rate 99% vs. 90.4â?»than Off-pump after 18 months follow-up as described by PR Moreno 2020 JACC Review showed less MACE as our finding. HRS technique has advantages in elderly similar fining described in journal of Geriatric [19-23].
Limitation of our Study
This was observational study with only six patients because its novel technique and lot of cost we need large randomized trial for efficacy hybrid revascularization.
Strength of the Study
It introduced the patient’s alternative option for patients, which are high risk for surgery, are benefited from HRS and more pa- tient satisfaction less MACE and shorter stay.
List Of Abbreviations
CAD: Coronary Artery Disease
PCI: Percutaneous Coronary Intervention
HRS: Hybrid Revascularization
LIMA: Left Internal Memory Artery
LCX: Left Circumflex Artery
RCA: Right Coronary Artery
LAD: Left Anterior Descending Artery
CTO: Chronic Total Occlusion
DES: Drug Eluting Stents
GFR: Glomerular Filtration rate ml/min
Conclusion
In this study, we found hybrid revascularization has more bene- fits less MACE, patient satisfaction and decrease stay in hospital and one-year follow up compared to CABG patients. We need larger scale studies, training of heart team for hybrid revascu- larization and more centers should be open for hybrid revascu- larization, population should be benefited with because CABG refusal is high so death from coronary disease is also is no one cause of death in patients with multivessel disease with low heart function will be reduced the one factor which need atten-tion as this study was done in UAE where insurance covered the procedure but in Pakistan this issue needs to be discussed health policy maker.
References
- Angelini, G. (1996). Integrated left small thoracotomy and angioplasty for multivessel coronary artery revasculariza- tion. Lancet, 347, 757-758.
- Hillis, L. D., Smith, P. K., Anderson, J. L., Bittl, J. A., Bridges, C. R., & et al. (2011). Association Task Force on Practice Guidelines 2011 ACCF/AHA Guideline for Coro- nary Artery Bypass Graft Surgery: Executive Summary: A Report of the American College of Cardiology Foundation/ American Heart. Circulation, 124, 2610-2642.
- Loop, F. D., Lytle, B. W., Cosgrove, D. M., Stewart, R. W., Goormastic, M., & et al. (1986). Influence of the in- ternal-mammary-artery graft on 10-year survival and other cardiac events. New England Journal of Medicine, 314(1), 1-6.
- Modrau, I. S., Nielsen, P. H., Nielsen, D. V., Christiansen, E. H., Hoffmann, T., & et al. (2020). Outcome of hybrid com- pared to conventional revascularization in multivessel coro- nary artery disease: A matched-group comparison of 3-year outcome following hybrid myocardial revascularization, conventional coronary artery bypass grafting, and percuta- neous coronary intervention. Scandinavian Cardiovascular Journal, 54(6), 376-382.
- Yan, T. D., Padang, R., Poh, C., Cao, C., Wilson, M. K., & et al. (2011). Drug-eluting stents versus coronary artery bypass grafting for the treatment of coronary artery disease: a meta-analysis of randomized and nonrandomized stud- ies. The Journal of Thoracic and Cardiovascular Surgery, 141(5), 1134-1144.
- Puskas, J. D., Williams, W. H., Mahoney, E. M., Huber, P. R., Block, P. C., & et al. (2004). Off-pump vs convention- al coronary artery bypass grafting: early and 1-year graft patency, cost, and quality-of-life outcomes: a randomized trial. JAMA, 291(15), 1841-1849.
- Narasimhan, S., Srinivas, V. S., & DeRose, J. J. (2011). Hybrid coronary revascularization: a review. Cardiology in review, 19(3), 101-107.
- De Cannière, D., Jansens, J. L., Goldschmidt-Clermont, P., Barvais, L., Decroly, P., & et al. (2001). Combination of minimally invasive coronary bypass and percutaneous transluminal coronary angioplasty in the treatment of dou- ble-vessel coronary disease: two-year follow-up of a new hybrid procedure compared with “on-pump” double bypass grafting. American Heart Journal, 142(4), 563-570.
- Harskamp, R. E., Bagai, A., Halkos, M. E., Rao, S. V., Ba- chinsky, W. B., & et al. (2014). Clinical outcomes after hy- brid coronary revascularization versus coronary artery by- pass surgery: a meta-analysis of 1,190 patients. American heart journal, 167(4), 585-592.
- Modrau, I. S., Nielsen, P. H., Bøtker, H. E., Christiansen,E. H., Krusell, L. R., & et al. (2015). Feasibility and early safety of hybrid coronary revascularisation combining off- pump coronary surgery through J-hemisternotomy with per- cutaneous coronary intervention. Eurointervention: Journal of Europcr in Collaboration with the Working Group onInterventional Cardiology of the European Society of Car-diology, 10(10), e1-6.
- Hu, S., Li, Q., Gao, P., Xiong, H., Zheng, Z., & et al. (2011). Simultaneous hybrid revascularization versus off-pump coronary artery bypass for multivessel coronary artery dis- ease. The Annals of thoracic surgery, 91(2), 432-438.
- Kon, Z. N., Brown, E. N., Tran, R., Joshi, A., Reicher, B., & et al. (2008). Simultaneous hybrid coronary revascular- ization reduces postoperative morbidity compared with re- sults from conventional off-pump coronary artery bypass. The Journal of thoracic and cardiovascular surgery, 135(2), 367-375.
- Halkos, M. E., Vassiliades, T. A., Douglas, J. S., Morris, D. C., Rab, S. T., & et al. (2011). Hybrid coronary revascu- larization versus off-pump coronary artery bypass grafting for the treatment of multivessel coronary artery disease. The Annals of Thoracic Surgery, 92(5), 1695-1702.
- Katz, M. R., Van Praet, F., de Canniere, D., Murphy, D., Si- wek, L., & et al. (2006). Integrated coronary revasculariza- tion: percutaneous coronary intervention plus robotic totally endoscopic coronary artery bypass. Circulation, 114(1_sup- plement), I-473-I-476.
- Bonatti, J., Schachner, T., Bonaros, N., Jonetzko, P., Öh- linger, A., & et al. (2008). Simultaneous hybrid coronary revascularization using totally endoscopic left internal mammary artery bypass grafting and placement of rapamy- cin eluting stents in the same interventional session. Cardi- ology, 110(2), 92-95.
- Dixon, L. K., Akberali, U., Di Tommaso, E., George, S., Johnson, T., & et al. (2022). Hybrid coronary revasculariza- tion versus coronary artery bypass grafting for multivessel coronary artery disease: A systematic review and meta-anal- ysis. International Journal of Cardiology, 359: 20-27.
- Wang, C., Li, P., Zhang, F., Li, J., & Kong, Q. (2021). Is hy- brid coronary revascularization really beneficial in the longterm. European Journal of Cardio-Thoracic Surgery, 60(5), 1158-1166.
- Van den Eynde, J., Bennett, J., McCutcheon, K., Adriaens- sens, T., Desmet, W., & et al. (2021). Heart team 2.0: A de- cision tree for minimally invasive and hybrid myocardial re- vascularization. Trends in Cardiovascular Medicine, 31(6), 382-391.
- Tajstra, M., Hrapkowicz, T., Hawranek, M., Filipiak, K., Gierlotka, M., & et al. (2018). Hybrid coronary revascular- ization in selected patients with multivessel disease: 5-year clinical outcomes of the prospective randomized pilot study. JACC: Cardiovascular Interventions, 11(9), 847-852.
- Basman, C., Hemli, J. M., Kim, M. C., Seetharam, K., Brin-ster, D. R., Pirelli, L., ... & Patel, N. C. (2020). Longâ?term survival in tripleâ?vessel disease: Hybrid coronary revas- cularization compared to contemporary revascularization methods. Journal of Cardiac Surgery, 35(10), 2710-2718.
- Hannan, E. L., Yi-Feng, W. U., Cozzens, K., Tamis-Hol- land, J., Ling, F. S., & et al. (2021). Hybrid coronary re- vascularization vs percutaneous coronary interventions for multivessel coronary artery disease. Journal of Geriatric Cardiology: JGC, 18(3), 159-167.
- Moreno, P. R., Stone, G. W., Gonzalez-Lengua, C. A., & Puskas, J. D. (2020). The hybrid coronary approach for op- timal revascularization: JACC review topic of the week. Journal of the American College of Cardiology, 76(3), 321- 333.
- Esteves, V., Oliveira, M. A., Feitosa, F. S., Mariani Jr, J., Campos, C. M., & et al. (2021). Late clinical outcomes of myocardial hybrid revascularization versus coronary artery bypass grafting for complex tripleâ?vessel disease: Longâ? term followâ?up of the randomized MERGING clinical trial. Catheterization and Cardiovascular Interventions, 97(2), 259-264.