
Advancements in Journal of Urology and Nephrology(AJUN)
ISSN: 2689-8616 | DOI: 10.33140/AJUN
Impact Factor: 1.0



Research Article - (2025) Volume 7, Issue 1
Factors Affecting the Early Post-Operative Outcome and Complications of Benign Prostatic Surgery at Algezira Hospital for Renal Diseases and Surgery
2Professor of urology, Department of Surgery (Urology), Faculty of medicine, University of Gezira state, MBBS-MDgeneral surgery, Wadmadani, Sudan
3Consultant at Department of Urology Algezira Hospital for Renal Diseases and Surgery, Department of Surgery (Urology), Faculty of medicine - University of Gezira state, Urology MD – Egypt,Wadmadani, Sudan
Received Date: Nov 29, 2024 / Accepted Date: Dec 16, 2024 / Published Date: Jan 07, 2025
Copyright: ©Â©2025 Haytham Babikir Ahmed Araibi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Araibi, H. B. A., Omran, M., Ahmed, A. A. (2025). Factors Affecting the Early Post-Operative Outcome and Complications of Benign Prostatic Surgery at Algezira Hospital for Renal Diseases and Surgery. Adv J Uro Nephro, 7(1), 01-10.
Abstract
Background and Objectives: Benign prostatic hyperplasia (BPH) predominantly affects males aged 50-70 years. The aim of this study was to identify factors influencing early post-operative outcomes and complications following surgical interventions for BPH.
Methods: This hospital-based, observational, prospective cohort study was conducted at Al Gezira Hospital for Renal Diseases and Surgery between February and August 2022. A total of 120 patients diagnosed with BPH were included in the analysis. Validated scaled questionnaire was used to identify the preoperative parameter and variables, and post-operative outcome and complications. Data analysis was conducted using the Statistical package of social science (SPSS V21.1), and P value was considered significant at (0.05).
Results: The majority of patients were aged over 80 years (36.7%), with a severe International Prostate Symptom Score (IPSS) category (67.5%), and presented with obstructive symptoms (52.5%). Forty-one-point seven percent (41.7%) of the patients underwent surgery due to failure of medical management, and 78.3% underwent transurethral resection of the prostate (TURP). Notably, 14.2% of patients failed to void immediately following catheter removal, 16.7% required blood transfusions, 5.8% experienced clot retention, and 25% developed urethral strictures. Advanced age (p = 0.053), higher IPSS scores, and the presence of irritative symptoms (p = 0.010) were associated with increased likelihood of post-catheterization voiding difficulties. Patients on medical therapy typically had shorter catheterization durations (p = 0.039) and a lower incidence of urethral stricture (p = 0.003). Those undergoing TVP had longer hospital stays, extended catheterization periods (p = 0.00), and a higher frequency of blood transfusions (p = 0.001).
Conclusions and Clinical Implications: The most common post-operative complication was urethral stricture. Preoperative factors such as age, prostate size, and prior medical treatment were significant predictors of post-operative outcomes. These findings suggest that tailored preoperative management based on individual risk factors could improve surgical outcomes.
Keywords
Benign Prostatic Hyperplasia, Preoperative Factors, Postoperative Complications, TURP, TVP, TUIP
Introduction and Literature Review
Introduction
The primary success rates for TURP (Transurethral Resection of the Prostate), TUI (Transurethral Incision of the Prostate), and open prostatectomy are generally high. However, long-term follow-up studies indicate that about 10% of patients may require additional procedures within 5 to 10 years. As the public has greater access to medical information, patients tend to present their complaints earlier than in the past, raising questions about whether these minor issues warrant surgical intervention [1].
Indications
Classic symptoms of "prostatism" may indicate benign prostatic hyperplasia (BPH) and bladder outlet obstruction, leading to surgical recommendations in cases of:
• Refractory urinary retention
• Hydronephrosis and azotemia
• Recurrent urinary infections
• Severe refractory hematuria
• Severe symptoms of outflow obstruction
• Development of vesical stones
Types of Surgical Management
• Open prostatectomy
• TURP
• TUI of the prostate
Outcomes and Complications
Frimodt-Moller et al. found that 85% of BPH patients selected for TURP based on symptoms experienced favorable outcomes. In a recent study, Dorflinger et al. reported no significant difference in maximum flow rates between TURP (19 ml/sec) and TUI (15 ml/sec), with symptom improvement rates of 95% and 93%, respectively. However, retrograde ejaculation occurred in 45% of the TURP group, while none in the TUI group. When comparing TURP and open prostatectomy, over 90% of patients in both groups reported satisfactory results throughout 5 years of follow-up.
Morbidity and Mortality
Mortality rates for TURP and open prostatectomy range from 0.9% to 2.9%. Melchior et al. analyzed over 2,000 patient’s post- transurethral resection, finding that the amount of tissue resected had minimal impact on morbidity and mortality unless more than 60 grams were involved. Perioperative complications were slightly higher in the TURP group compared to open surgery, typically ranging from 2-3%, largely dependent on the urologist's expertise. Blood loss during surgery is generally greater in open prostatectomy cases. O’Conor noted a 4% complication rate for myocardial infarction, congestive heart failure, and pulmonary embolism, compared to 5% for hemorrhage, 3% for incontinence, and 4% for epididymitis. Incontinence due to sphincter damage occurs in about 1% of cases when excessive resection is attempted. Late follow-up studies have shown that 12.8-25% of TURP patients required a second procedure compared to 7% of those who underwent open surgery. Thus, successful surgical treatment of BPH relies on:
1. Appropriate surgical indications
2. Correct technique and procedure for the prostate size Reported rates of impotence post-surgery range from 5% to 40%, influenced by the degree of preoperative erectile dysfunction.
The Effect of Perioperative Parameters on Surgical Outcomes
The relationship between preoperative factors (such as age, prostate size, PR findings, and PSA levels) and postoperative complications is crucial. Common surgical indications include lower urinary tract symptoms, urinary retention, chronic prostatitis, gross hematuria, and bladder stones. Several studies have shown lower rates of acute urinary retention and gross hematuria in patients treated with alpha-adrenergic blockers and 5-alpha-reductase inhibitors. One study indicated that 15.2% of patients experienced complications, while others reported rates around 28%.Late postoperative complications from prostatic surgery can include posterior urethral stricture (which has decreased significantly due to advancements in urethral instrumentation), bladder neck contracture, urinary tract infections, and late postoperative bleeding. Additionally, retrograde ejaculation and erectile dysfunction are known complications of prostatic surgery.
Problem Statement
Despite the significant increase in patients undergoing surgery for benign prostatic conditions, there is a lack of sufficient statistics and studies in Sudan regarding the types of benign prostatic surgeries, their indications, early and late postoperative complications, and any correlations between preoperative factors and postoperative outcomes. This paper aims to illuminate these areas and draw conclusions.
Objectives and Aims
General Objective
The primary goal of this research is to identify factors that may influence early postoperative outcomes and complications associated with various benign prostatic surgeries.
3.2 Specific Objectives
• To gather demographic information about patients diagnosed with BPH.
• To identify preoperative factors that may affect surgical outcomes.
• To detect the early post- operative outcomes and complications (during the first three months period).
• To correlate the different preoperative parameters to these early postoperative outcome and complications.
Research Design and Methods
Study Design:
This study is a hospital-based, observational, prospective cohort design.
Study Area:
The research was conducted at Al Gezira Hospital for Renal Diseases and Surgery, located in Al-Gezira State, Sudan.
Study Duration:
The study was carried out over a period from February to August 2022.
Study Population:
The study population consisted of male patients diagnosed with benign prostatic conditions who underwent surgical intervention.
Inclusion Criteria
The inclusion criteria were as follows:
• Adult males aged 18 years or older.
• Diagnosed with benign prostatic hyperplasia (BPH).
• Underwent surgical treatment for BPH.
Exclusion Criteria
Patients were excluded from the study based on the following criteria:
• Loss to follow-up.
• Refusal to participate in the study.
• A diagnosis of prostate carcinoma.
Sample Size and Selection of Sample
The sample size was calculated using the OpenEpi statistical software. Based on the calculation, the estimated sample size for the study was approximately 154 patients.
Data Collection Tools and Methods
Data were collected using a standardized, validated questionnaire, designed for personal interviews with patients. These interviews were conducted both in the pre-operative period and three months post-operatively. Data were recorded and stored in a Microsoft Excel spreadsheet for analysis.
Study Variables
The study variables included the following:
• Demographic information of the patients.
• Pre-operative parameters.
• Early and late post-operative outcomes and complications.
Data Analysis
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS), version 21.0. Chi-square tests were used to assess associations, and a p-value of less than 0.05 was considered statistically significant.
Ethical Consideration
The study protocol and methodology were approved by the Ministry of Health (MOH) and the Ethics and Documentation Committee (EDC) of the Sudan Medical Specialization Board. Written informed consent was obtained from all patients participating in the study, and patient confidentiality was ensured by using anonymized identification numbers in place of individual's names.
Results
A total of 120 patients diagnosed with benign prostatic conditions were included in this study. The majority of patients were aged over 80 years (32.7%), engaged in laborious occupations (75.8%), resided in rural areas (70%), and were married to a single wife (74.2%) (Table 1).The preoperative parameters, which were hypothesized to influence early postoperative outcomes, included the following:
• International Prostate Symptom Score (IPSS): The majority of patients (67.5%) fell within the severe symptom category
• Symptom Type: The most prevalent bothersome symptoms were obstructive symptoms (52.5%)
• Medical Treatment: A significant proportion of patients (72.7%) were on medical treatment prior to surgery
• Indication for Surgery: The primary indication for surgery was the failure of medical treatment (41.7%)
• Prostate-Specific Antigen (PSA) Levels: Most patients had a PSA level of less than 4 ng/dl (65%).
• Prostate Size: A prostate size of 60-80 mL was most commonly observed (52.7%)
• Surgical Procedure: The most frequently performed surgical procedure was transurethral resection of the prostate (TURP) (78.3%) (Table 2).
• Regarding early postoperative outcomes and complications (within the first three months), the following findings were observed:
• Length of Hospital Stay: The majority of patients were discharged within three days (70.8%)
• Catheterization Duration: Most patients were catheterized for a period ranging from 4 to 9 days (64.2%)).
• Post-catheter Voiding: Approximately 14.2% of patients were unable to void immediately following catheter removal
• Blood Transfusion: A minority of patients (12.7%) received intraoperative or postoperative blood transfusions
• Clot Retention: About 5.8% of patients experienced clot retention, leading to catheter obstruction, and were managed either conservatively (3.3%) or operatively (2.5%).
• Urethral Stricture: Urethral stricture, diagnosed via ascending/ descending urethrogram or cystoscopy, occurred in 25% of patients (Table 3).
• To assess the relationship between preoperative parameters and subsequent postoperative outcomes and complications, each preoperative variable was analyzed for potential statistical correlations:
• Age: Age was found to influence the inability to void immediately after catheter removal, approaching statistical significance (P = 0.053) (Figure 1).
• IPSS: A higher IPSS was significantly associated with increased frequency of intraoperative or postoperative blood transfusion (P = 0.010) (Table 4).
• Symptom Type: Patients with irritative symptoms were more likely to experience difficulty voiding after catheter removal (P = 0.010) (Figure 2).
• Medical Treatment: Patients on medical treatment had a shorter catheterization period (P = 0.039), (Figure 3) and were less likely to develop urethral stricture (P = 0.003) (Table 5).
• Indication for Surgery: The indication for surgery affected the length of the postoperative hospital stay, with patients undergoing surgery due to failure of medical treatment (FMOT) or urinary retention staying longer (P = 0.019). Additionally, the group undergoing surgery for FMOT and vesical stone was less likely to experience clot retention postoperatively (P = 0.020).
• Prostate Size: Larger prostate size was associated with a longer hospital stay (P = 0.003) (Figure 4) and a higher risk of requiring intraoperative or postoperative blood transfusion (P = 0.006) (Figure 5).
• Type of Surgery: Transvesical prostatectomy (TVP) was associated with a longer hospital stay compared to transurethral resection of the prostate (TURP) or transurethral incision of the prostate (TUIP) (P = 0.00), a longer catheterization period (P = 0.00), and a higher likelihood of requiring blood transfusion during the perioperative period (P = 0.001).
Table 1: Patient Distribution According to Demographic Data (N=120)
|
Age Group |
Frequency |
Percentage |
|
<60 years |
33 |
27.5% |
|
61-69 years |
43 |
35.8% |
|
71-80 years |
44 |
36.7% |
|
Total |
120 |
100.0% |
|
Residency |
||
|
Rural |
84 |
70.0% |
|
Urban |
36 |
30.0% |
|
Total |
120 |
100.0% |
|
Occupation |
||
|
Laborer |
91 |
75.8% |
|
Employee |
29 |
24.2% |
|
Total |
120 |
100.0% |
|
Marital status |
||
|
One wife |
89 |
74.2% |
|
Two wives |
29 |
24.2% |
|
Three wives |
2 |
1.7% |
|
Total |
120 |
100.0% |
Table 2: Patient Distribution According to Preoperative Factors (N=120)
|
IPSS |
Frequency |
Percentage |
|
Mild |
1 |
.8% |
|
Moderate |
38 |
31.7% |
|
Severe |
81 |
67.5% |
|
Total |
120 |
100.0 |
|
Bothersome symptoms |
||
|
Irritative |
57 |
47.5% |
|
Obstructive |
63 |
52.5% |
|
Total |
120 |
100.0 |
|
Use of medical treatment |
||
|
YES |
92 |
76.7% |
|
NO |
28 |
23.3% |
|
Total |
120 |
100.0 |
|
Indication for surgery |
||
|
FMOT |
50 |
41.7% |
|
Urine retention |
51 |
42.5% |
|
Vesical stone |
10 |
8.3% |
|
Renal impairment |
9 |
7.5% |
|
PSA level |
120 |
100.0% |
|
<4 ng/dl |
78 |
65.0% |
|
4-10 ng/dl |
25 |
20.8% |
|
>10 ng/dl |
17 |
14.2% |
|
Total |
120 |
100.0% |
|
Prostate size |
||
|
<40 mg |
17 |
14.2% |
|
40-80 mg |
68 |
56.7% |
|
>80 mg |
35 |
29.2% |
|
Total |
120 |
100.0% |
|
Type of surgery |
||
|
TURP |
94 |
78.3% |
|
TVP |
22 |
18.3% |
|
TUIP |
4 |
3.3% |
|
Total |
120 |
100.0% |
Table 3: Patient Distribution According to Postoperative Outcome/Complications (N=120)
|
Length of postoperative hospital stay |
Frequency |
Percentage |
|
<3 days |
85 |
70.8% |
|
3-7 days |
35 |
29.2% |
|
Total |
120 |
100.0% |
|
Length of postoperative catheterization |
||
|
<3 days |
6 |
5.0% |
|
4-9 days |
77 |
64.2% |
|
>10 days |
37 |
30.8% |
|
Total |
120 |
100.0% |
|
Postoperative inability to void |
||
|
YES |
17 |
14.2% |
|
NO |
103 |
85.8% |
|
Total |
120 |
100.0% |
|
Intra/postoperative blood transfusion |
||
|
YES |
20 |
16.7% |
|
NO |
100 |
83.3% |
|
Total |
120 |
100.0% |
|
Clot retention treated with with/without operation |
||
|
NO |
113 |
94.2% |
|
Without operation |
4 |
3.3% |
|
With operation |
3 |
2.5% |
|
Total |
120 |
100.0% |
|
Postoperative urethral stricture |
||
|
YES |
30 |
25.0% |
|
NO |
90 |
75.0% |
|
Total |
120 |
100.0% |
Table 4: Preoperative Factors Affecting the Intra/Postoperative Rate of Blood Transfusion (N=120)/Ipss
|
IPSS |
Intraoperative postoperative blood transfusion |
Total |
P value |
|||
|
|
|
|
YES |
NO |
1 |
|
|
Mild |
Count |
1 |
0 |
1.0 |
|
|
|
Expected Count |
.2 |
.8 |
38 |
P= 0.010 |
||
|
Moderate |
Count |
2 |
36 |
38.0 |
|
|
|
Expected Count |
6.3 |
31.7 |
81 |
|
||
|
|
Severe |
Count |
17 |
64 |
81.0 |
|
|
Expected Count |
13.5 |
67.5 |
120 |
|
||
|
Total |
Count |
20 |
100 |
120.0 |
|
|
|
Expected Count |
20.0 |
100.0 |
|
|
||
Table 5: Preoperative Factor Affecting the Postoperative Rate of Urethral Stricture (N=120)/ Medical Treatment
|
On medications |
Postoperative urethral stricture |
Total |
P value |
|||
|
YES |
NO |
|||||
|
|
YES |
Count |
17 |
75 |
92 |
|
|
Expected Count |
23.0 |
69.0 |
92.0 |
P= 0.003 |
||
|
NO |
Count |
13 |
15 |
28 |
|
|
|
Expected Count |
7.0 |
21.0 |
28.0 |
|
||
|
Total |
Count |
30 |
90 |
120 |
|
|
|
Expected Count |
30.0 |
90.0 |
120.0 |
|
||
|
|
YES |
Count |
17 |
75 |
92 |
|
|
Expected Count |
23.0 |
69.0 |
92.0 |
P= 0.003 |
||
|
NO |
Count |
13 |
15 |
28 |
|
|
|
Expected Count |
7.0 |
21.0 |
28.0 |
|
||
|
Total |
Count |
30 |
90 |
120 |
|
|
|
Expected Count |
30.0 |
90.0 |
120.0 |
|
||
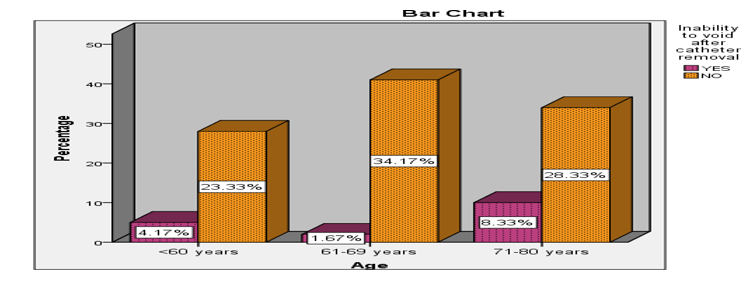
Figure 1: Showing Preoperative Factors Affecting Inability to Void Immediately After Catheter Removal (N=120)/Age
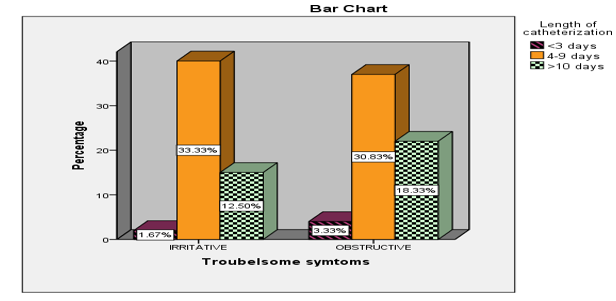
Figure 2: Showing Preoperative Factors Affecting Inability to Void Immediately After Catheter Removal (N=120)/Predominant Symptom
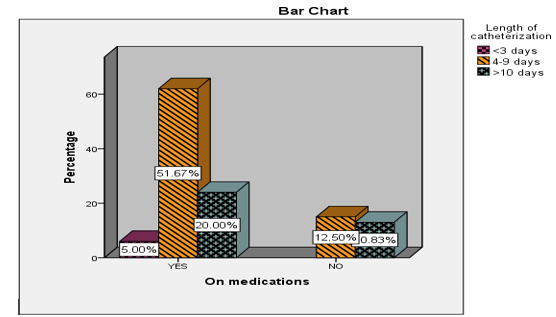
Figure 3: Showing Preoperative Factors Affecting the Length of Postoperative Catheterization (N=120)/ Medical Treatment
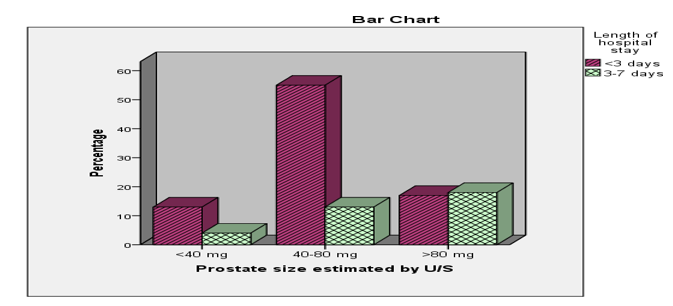
Figure 4: Showing preoperativeFactors Affecting the Length of Postoperative Hospital Stay (n=120)/Prostate Size
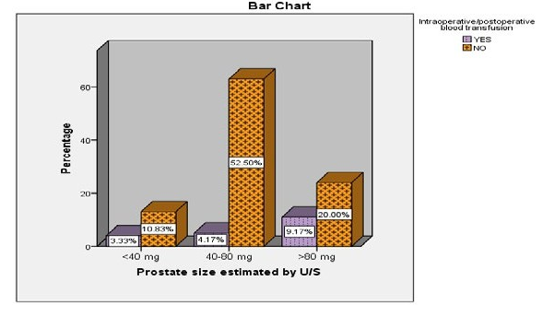
Figure 5: Showing Preoperative Factors Affecting the Intra/Postoperative Rate of Blood Transfusion (N=120)/Prostate Size
Discussion
This study demonstrated that the majority of the study population was in the age group of 70–80 years (32.7%), which is consistent with findings from other studies, such as Doll et al. (mean age 70 ± 8 years), and Reich et al. (median age 71.7 ± 27.7 years) [2,3]. This finding is slightly higher than that reported by TascÃÂ?± et al. (mean age 65 ± 2.9 years) [4].
Several preoperative factors that may influence early postoperative outcomes were identified in this study:
• International Prostate Symptom Score (IPSS): The majority of patients (67.5%) were classified in the severe symptom category (IPSS 20-35), a finding consistent with Gratzke et al. (mean IPSS 20.7 ± 7.6) [5]. This severity likely contributes to the failure of medical treatment, making these patients candidates for surgery.
• Symptom Profile: Obstructive symptoms were more prevalent (52.5%) compared to irritative symptoms (47.5%), which contrasts with the findings of Doll et al. (67% obstructive vs. 77% irritative symptoms) [2].
• Medical Treatment: A substantial proportion of patients (72.7%) were on medical treatment, indicating that medical therapy alone may not always prevent the need for surgical intervention in BPH patients.
• Indications for Surgery: The most common indications for surgery were failure of medical treatment (41.7%) and acute urinary retention (42.5%). A smaller proportion of patients underwent surgery due to vesical stones (8.3%) or renal function impairment (7.5%), which aligns with findings by Doll et al [2].
• Prostate-Specific Antigen (PSA): The majority of patients (65%) had a PSA level of < 4 ng/dl, consistent with the data reported by TascÃÂ?± et al. (mean PSA 3.9 ± 0.9 ng/dl) [4].
• Prostate Size: A prostate size between 60-80 mL was observed in 52.7% of the study population, which is in line with the findings of TascÃÂ?± et al. (62.4 ± 12 mL) [4], although slightly larger than the prostate size reported by Bach et al. (57.1 ± 34.4 mL) [6].
• Renal Function: Preoperative renal function was within normal limits in 88.3% of patients, a finding comparable to that reported by Doll et al. [2].
• Regarding early postoperative outcomes (within the first 3 months), the following observations were made:
• Hospital Stay: The mean length of hospital stay was similar to the findings of Bach et al. (3.8 ± 2.4 days) [6] and TascÃÂ?± et al. (29 ± 1.2 hours) [4], but was longer compared to the ranges reported by Doll et al., where the median stay was 1-7 days, with a few cases exceeding 15 days [2].
• Catheterization Duration: The mean catheterization time was longer than that reported by TascÃÂ?± et al. (24 ± 2.3 hours) [4].
• Blood Transfusion: In this study, 12.7% of patients required intraoperative or postoperative blood transfusion, a figure comparable to the 24% reported by Doll et al. [2] but lower than the 7.5% reported by Gratzke et al. [5].
• Clot Retention and Obstruction: The incidence of clot retention and catheter obstruction (5%) was similar to that reported by Bach et al. [6], but lower than the 11% observed by Doll et al. [2].
• Urethral Stricture/Bladder Neck Stenosis: The incidence of urethral stricture or bladder neck stenosis (25%) was higher than previously reported in the literature, where rates typically range from 2.2% to 9.8%. This could be explained by the fact that most surgeries at our institution are performed by trainee registrars, which may result in longer operative times and potentially higher complication rates. Longer catheterization may also contribute to this increase rate of stricture formation. Hoffmann et al. suggested that meatal stenosis occurs due to the disproportionate size relationship between the urethral and surgical instruments, while bulbar urethral stricture may result from current leaks during the procedure. TascÃÂ?± et al[4]. reported a posterior urethral stricture rate of 3.2% and bladder neck stenosis of 1.08%.
• Additionally, the following associations between preoperative parameters and postoperative outcomes were observed:
• Age: Age was associated with the inability to void immediately after catheter removal (P = 0.053).
• IPSS: A higher preoperative IPSS was significantly correlated with a higher frequency of intraoperative or postoperative blood transfusion (P = 0.010).
• Symptom Type: Patients with predominantly irritative symptoms were more likely to be unable to void after catheter removal (P = 0.010).
• Medical Treatment: Patients not on medical treatment had a longer catheterization period (P = 0.039) and were more likely to develop urethral stricture (P = 0.003).
• Indication for Surgery: Patients undergoing surgery for failure of medical treatment or urinary retention tended to have longer hospital stays (P = 0.019), while those undergoing surgery for failure of medical treatment and vesical stones were less likely to develop clot retention (P = 0.020).
• Prostate Size: Larger prostate size was associated with longer hospital stays (P = 0.003)and increased risk of intraoperative or postoperative blood transfusion (P = 0.006).
• Surgical Approach: TVP was associated with longer hospital stays (P = 0.00), longer catheterization periods (P = 0.00), and a higher likelihood of receiving blood transfusions (P = 0.001).
Limitations
1. The study was conducted at a single institution, limiting the generalizability of the findings to national or international populations.
2. Financial constraints limited the ability to investigate additional factors that may play a role in predicting postoperative outcomes, such as urodynamic studies, flow studies, or post-void residual volume measurements.
3. Intraoperative findings and events may serve as more significant predictors of postoperative complications than the preoperative parameters examined in this study, suggesting potential areas for future research.
Conclusion
The majority of BPH patients who underwent surgical intervention, particularly transurethral resection of the prostate (TURP), were older, with severe symptoms, and had previously undergone medical treatment. The most frequent postoperative complication was urethral stricture. Factors such as age, IPSS, predominant symptoms, prostate size, and medical treatment, indication for surgery, and type of surgery were found to influence postoperative outcomes and complications [7,23].
Acknowledgements
I am grateful to all of those with whom I have had the pleasure to work during this project. Special thanks to my great supervisor, prof: Mustafa Omran, for his patience, dedication and continuous support and advices, without which, this work could not see the light. My gratitude extended to all the family of the department of urology at GHRDS, who supported me during this study period. and to the members of the ethical Committee who provided me with extensive personal and professional guidance and taught me a great deal about scientific research.
References
- Berry, S. J., Coffey, D. S., Walsh, P. C., & Ewing, L. L. (1984). The development of human benign prostatic hyperplasia with age. The Journal of urology, 132(3), 474-479.
- Doll, H., Black, N. A., McPherson, K., Flood, A. B., Williams,G. B., & Smith, J. C. (1992). Mortality, morbidity and complications following transurethral resection of the prostate for benign prostatic hypertrophy. The Journal of urology, 147(6), 1566-1573.
- Reich, O., Gratzke, C., Bachmann, A., Seitz, M., Schlenker, B., Hermanek, P., ... & Urology Section of the Bavarian Working Group for Quality Assurance†. (2008). Morbidity, mortality and early outcome of transurethral resection of the prostate: a prospective multicenter evaluation of 10,654 patients. The Journal of urology, 180(1), 246-249.
- Tascı, A. I., Ilbey, Y. O., Tugcu, V., Cicekler, O., Cevik, C., &Zoroglu, F. (2011). Transurethral resection of the prostate with monopolar resectoscope: single-surgeon experience and long-term results of after 3589 procedures. Urology, 78(5), 1151-1155.
- Gratzke, C., Schlenker, B., Seitz, M., Karl, A., Hermanek, P., Lack, N., ... & Reich, O. (2007). Complications and early postoperative outcome after open prostatectomy in patients with benign prostatic enlargement: results of a prospective multicenter study. The Journal of urology, 177(4), 1419-1422.
- Bach, T., Wölbling, F., Gross, A. J., Netsch, C., Tauber, S., Pottek, T., ... & Brunken, C. (2017). Prospective assessment of perioperative course in 2648 patients after surgical treatment of benign prostatic obstruction. World journal of urology, 35, 285-292.
- Janknegt, R. A. (1989). Surgical management for benign prostatic hyperplasia: indications, techniques, and results. The Prostate, 15(S2), 79-93.
- Shepard, R. L., Kraus, S. E., Babayan, R. K., & Siroky, M. B. (1987). The role of ammonia toxicity in the post transurethral prostatectomy syndrome. British journal of urology, 60(4), 349-351.
- Dørflinger, T., Øster, M., Larsen, J. F., Walter, S., & Krarup, T. (1989). Transurethral Prostatectomy or Incision of tie Prostate in the Treatment of Prostatism Caused by Small Benign Prostates. The Journal of Urology, 141(1), 195-196.
- Graversen, P. H., Gasser, T. C., Larsen, E. H., Dørflinger, T., & Bruskewitz, R. C. (1987). Transurethral incisions of the prostate under local anaesthesia in high-risk patients: a pilot study. Scandinavian journal of urology and nephrology. Supplementum, 104, 87-90.
- Meyhoff, H. H., & Nordling, J. (1986). Long term results of transurethral and transvesical prostatectomy: A randomized study. Scandinavian journal of urology and nephrology, 20(1), 27-33.
- Chilton, C. P., Morgan, R. J., England, H. R., Paris, A. M.I., & Blandy, J. P. (1978). A critical evaluation of the results of transurethral resection of the prostate. British Journal of Urology, 50(7), 542-546.
- Melchior, J., Valk, W. L., Foret, J. D., & Mebust, W. K. (1974). Transurethral prostatectomy: computerized analysis of 2,223 consecutive cases. The Journal of urology, 112(5), 634-642.
- Wennberg, J. E., Mulley, A. G., Hanley, D., Timothy,R. P., Fowler, F. J., Roos, N. P., ... & Malenka, D. (1988). An assessment of prostatectomy for benign urinary tract obstruction: geographic variations and the evaluation of medical care outcomes. Jama, 259(20), 3027-3030.
- Roos, N. P., & Ramsey, E. W. (1987). A population-based study of prostatectomy: outcomes associated with differing surgical approaches. The Journal of urology, 137(6), 1184- 1188.
- Mebust, W. K., Holtgrewe, H. L., Cockett, A. T. K., Peters,P. C., Bueschen, A. J., Carlton Jr, C. E., ... & Witherington,R. (1989). Transurethral prostatectomy: immediate and postoperative complications. A cooperative study of 13 participating institutions evaluating 3,885 patients. The Journal of urology, 141(2), 243-247.
- Jardin, A., Bensadoun, H., Delauche-Cavallier, M. C., Attatli, P., & The, B. A. (1991). Alfuzosin for treatment of benign prostatic hypertrophy. The Lancet, 337(8755), 1457-1461.
- Miller, M. I., & Puchner, P. J. (1998). Effects of finasteride on hematuria associated with benign prostatic hyperplasia: long- term follow-up. Urology, 51(2), 237-240.
- SIEBER, P. R., ROMMEL, F. M., HUFFNAGLE, H. W., BRESLIN, J. A., AGUSTA, V. E., & HARPSTER, L. E.(1998). The treatment of gross hematuria secondary to prostatic bleeding with finasteride. The Journal of urology, 159(4), 1232-1233.
- JD, M. (1998). The effect of finasteride on the risk of acute urinary retention and the need for surgical treatment among men with benign prostatic hyperplasia. N. Engl. J. Med., 338, 557-563.
- Borboroglu, P. G., Kane, C. J., Ward, J. F., Roberts, J. L., & Sands, J. P. (1999). Immediate and postoperative complications of transurethral prostatectomy in the 1990s. The Journal of urology, 162(4), 1307-1310.
- Black, N., Petticrew, M., Ginzler, M., Flood, A., Smith, J., Williams, G., ... &Mcpherson, K. (1991). Do doctors and patients agree?: Views of the outcome of transurethral resection of the prostate. International journal of technology assessment in health care, 7(4), 533-544.
- Resektion, T. (2005). und transurethraleInzision (TUIP) der Prostata. Endoskopischeurologie, 49.