
International Journal of Diabetes & Metabolic Disorders(IJDMD)
ISSN: 2475-5451 | DOI: 10.33140/IJDMD
Impact Factor: 1.23


Research Article - (2024) Volume 9, Issue 2
Diabetic Retinopathy: Pathophysiology and New Pathways
Received Date: Jun 12, 2024 / Accepted Date: Jul 18, 2024 / Published Date: Jul 26, 2024
Copyright: ©©2024 Nakhoul F. Nakhoul, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Citation: Nakhoul, N. F., Mamdoh, D. (2024). Diabetic Retinopathy: Pathophysiology and New Pathways. Int J Diabetes Metab Disord, 9(2), 01-06.
Abstract
Diabetic retinopathy is one of the most common microvascular complications of diabetes mellitus, which is associated with damage of blood-retinal barrier and ischemia of retinal vasculature. Consequently, there is a decrease in visual acuity due to leakage of retinal vessels and aberrant pathological angiogenesis. Different studies have shown that autophagy & klotho proteins can plays an important role in the pathogenesis of DR,
Type 2 diabetes mellitus, is associated with increased glucose cell toxicity and oxidative stress that can lead to irreversible damage in retina. Autophagy plays a critical role in degradation of damaged intracellular proteins to maintain intracellular homeostasis. The Klotho is a circulating anti-aging hormone with anti-oxidative and anti-inflammatory properties with vascular protective effects. The disturbance of autophagy and klotho pathways are involved in the pathogenesis of diabetic retinopathy, especially the expression of klotho, ATG5 and its collaborator LC3-II. In early stages of diabetic retinopathy, klotho protein expression decreased, and LC3-II/ ATG5 proteins levels are increased.
Laser therapy, anti-VEGF intra-ocular injection, and vitrectomy are the conventional treatments in proliferative retinopathy but their capacity to reverse visual impairment are poor. Recently, different investigators showed that, the new anti-diabetic drugs such as the sodium-glucose transporter 2 inhibitors and the GLP-1 receptor agonists could be protective in early stages of diabetic retinopathy. In this review, we will present the suggested recent new pathways involved in early diabetic retinopathy and the recent anti-diabetic drugs such as the sodium-glucose transporter 2 inhibitors and the GLP-1 receptor agonist used in patients with type 2 diabetes mellitus that can be protective drugs against the progression of diabetic retinopathy.
Keywords
Diabetic Retinopathy, Autophagy, Klotho, SGLT2i, EMPA, GLP1-AR
Introduction
Diabetes mellitus type II (DM TII) affects about 400 million adults worldwide is defined as ever metabolic disorder characterized by high blood glucose and insulin resistance [1,2]. DM type II is associated with increased glucose cell toxicity and oxidative stress that can lead to irreversible damage in several organs, such as the kidney, heart, and retina. Diabetic retinopathy (DN) is a major microvascular complication of diabetes, and causes visual impairment and blindness, being the leading cause of vision loss among adults [3].
Chronic exposure to high blood glucose triggers a chain of biochemical and functional processes leading to micro and macro-vascular damage, which activate pro-inflammatory mediators and oxidative stress pathways, which further amplify the inflammatory signals through multiple pathways such as autophagy and klotho pathways. The resultant chronic activation of inflammatory cascades results in damage to the retinal microvasculature [4,5].
DR is a very common long-term complication of DM type II, defined as a microangiopathy of the retina from which nearly all persons with DM eventually suffer. Two of these complications are diabetic macular edema and proliferative DN. DN is characterized by micro-aneurysms, retinal edema, and hemorrhage with hard exudate [6,7].The other frequent and serious proliferative type is characterized by abnormal growth of small abnormal blood vessels in the eye due to retinal cells hypoxia and increased synthesis of vascular endothelial growth factor (VEGF), neo-vascularization at the disc, vitreous hemorrhages that end in retinal detachment and blindness [8-10].
The risk of developing DR is associated with the duration of DM and HbA1c levels. The progression of DR can be prevented by early diagnosis and better control of glucose plasma levels to near normal HbA1c. The other accompanied major risk factors for the development of DR include systemic arterial hypertension, chronicity of DM, hyperlipidemia, and progression of microalbuminuria. The persistent progression of microalbuminuria among diabetic patients helps in predicting the risk of developing major microvascular complications such as nephropathy, cardiovascular events, and DR [3].
The use of the recent anti-vascular endothelial growth factor (anti-VEGF) injections are the standard treatment for many patients with DR. This routine treatment, improves visual acuity in about 40% of patients. Others needs laser therapy in non-responsive cases. Most therapies target the late proliferative stage of the disease, at a time when retinal structure is hardly damaged [13]. Until today our understanding and ability to successfully treat DM patients and stabilize the HbA1c with new drugs such as the sodium-glucose transporter 2 inhibitors (SGLT2Is) and GLP1-AR is not clear totally [14]. The new medications that delay the progression of diabetic nephropathy and heart failure can also change dramatically the progression of DR.
Pathogenesis
Vascular Endothelial Growth Factor (VEGF)
Studies published support a role of vascular endothelial growth factor (VEGF) in the pathogenesis of proliferative DR. VEGF-induced angiogenesis and increased permeability as a response to microvascular ischemia and hypoxia in the retina and ocular fluid. Elevated levels of VEGF, increasing vascular permeability, and decreased retinal blood flow, appear in diabetic patients before the onset of DR12,13. Andy Levy and his group found a small percentage of patients with protective Haptoglobin (Hp 1-1) do not develop any evidence of DR even after many years of diabetes, due to decreased VEGF in these patients12. A wide variety of cytokines and metabolites, such as AGEs, IGF-1, insulin, and angiotensin II are elevated in diabetic patients and have been suggested to promote DR via stimulation of VEGF.
Klotho
As we mentioned above, DM is a group of metabolic diseases characterized by high blood glucose levels (hyperglycemia) and caused by defects in insulin secretion or resistance with consequent organ damage. The most common form is type 2 DM (T2DM), which accounts for 90% of diagnosed diabetes cases. Chronic hyperglycemia can involve different vital organs, and cause micro, and macro-vascular complications such as s diabetic nephropathy (DN) and retinopathy (DR). More, hyperglycemia triggers pro-inflammatory mediators, which activate oxidative stress pathways with increased production of free reactive oxygen species and further amplify the inflammatory signal through another multiple pathway [15,16].
Klotho is a novel antiaging gene encoding a protein with multiple pleiotropic effects. The klotho family of proteins consists of three members: Klotho α-klotho, β-klotho, and γ-klotho [20]. The α-klotho gene is highly expressed in the kidneys and retina and is affected by pathophysiological conditions including chronic hypertension, oxidative stress, and diabetes mellitus (DM). α-Klotho protein exists in two forms: a single-pass transmembrane protein and a secreted protein. The secreted form is involved in important biological processes including suppression of oxidative stress [18,17]. Klotho is a circulating anti-aging hormone with anti-oxidative and anti-inflammatory properties that has demonstrated vascular protective effects in animal studies. Recent data suggests that low levels of circulating Klotho predict an increased risk of progression of cardiovascular and renal disease. Previous studies showed that the KL gene had a critical function for retinal health. In people with type 2 diabetes, lower circulating levels of the vascular protective hormone Klotho are associated with an increased risk of progression of DR. Klotho may be a novel biomarker and potential treatment target for diabetic retinal disease. The role of Klotho in predicting the progression of DR has not been studied and is currently unknown [19,20].
Some studies have shown that serum KL level was lower in diabetes patients than in healthy participants and decreased gradually among the patients without DR, nonâ?proliferative DR, and proliferative DR subgroups. Their data suggested that KL protein was probably a potential protective factor against retinopathy in type 2 diabetes patients [22]. Our group by Nakhoul et al [13]. showed in BTBR mouse strain with the ob/ob leptin-deficiency mutation that develops spontaneously severe T2 DM, a significantly decreased retinal αKL protein expression levels in diabetic mice than control, which restored to near normal with the new anti-diabetic sodium-glucose-transport 2 inhibitor (SGLT2i) Empagliflozin treatment compared to DM mice. Our results suggest that α-KL protein can be involved in the pathogenesis of DR, and could probably be a potential protective factor against retinopathy developing in T2DM patient [23].
Autophagy Proteins (Atg5/LC3)
As we mentioned before, DR is a microvascular complication of diabetes and a major cause of vision loss around the world, and 50 to 80% of patients with type 2 diabetes will have DR within 20 to 25 years. DR is characterized by the release of pro-inflammatory cytokines and the adhesion of leukocytes to retinal capillaries in the early stages of DR. Inflammation, oxidative stress, and the recent proteins Klotho and autophagy, are the major causative factors involved in the pathogenesis of DR [24,25]. Hyperglycemia leads to mitochondrial electron transport chain dysfunction ending in a rise in reactive oxygen species (ROS) generation and oxidative stress. Increased generation of ROS directly or indirectly induces inflammation that contributes to the retinal cell layer damage and development of early DR. Moreover, oxidative stress can also alter the expression of the main player, the VEGF, that accelerates neo-vascularization in the retina, and consequently activates other metabolic pathways involved in the development of DR such as polyol pathway, advanced glycation product (AGE) formation, protein kinase C (PKC) pathway, and the autophagy pathway [Fig.1]
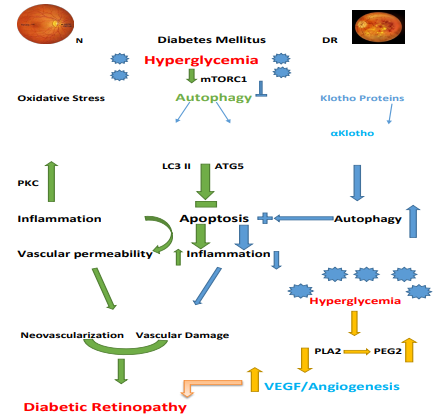
Figure 1: Schematic Overview of Pathogenic Mechanisms Leading to the Sight-Threatening Endpoints of Diabetic Retinopathy.
DR arises through a complex interplay between inflammation and vascular damage those results from hyperglycaemia-induced metabolic stress. Hyperglycemia stimulate mTORC1 that stimulate autophagy in early stages. Klotho protein α trigger the autophagy and apoptosis. Klotho proteins (α) decreased in the CGL cells of the retina. Neurological dysfunction with lekostasis and hypoperfusion.
Autophagy is essential for retinal development and vision formation. Autophagy is a well-coordinated multi-step process regulated by autophagy-related gene (Atg). Initially, a phagophore forms around cytoplasmic components that are then sequestered by a double membrane, which forms the autophagosome. The autophagosome subsequently fuses with the lysosome to form an autolysosome; the enclosed contents are then degraded. Autophagy can be measured by microtubule-associated proteins 1A/1B light chain 3B (LC3-II 3B) and Atg5 protein expression. In the course of autophagy, the (LC3-I) is transformed to LC3-II, which permits the combination of the protein to autophagosome membranes with Atg5 protein. So, light chain 3 (LC3) and ATG5 are key autophagy proteins, which have a central role in the pathogenesis of DM vascular complications [26,27].
Autophagy increases in the early stages of diabetic retina patients (Hyperglycemic milieu) and is regulated by endoplasmic reticulum (ER) stress, oxidative stress, and inflammation-related pathways.
Under mild stress, autophagy activity can lead to cell survival while during severe stress, dysregulated autophagy results in massive cell death and may have a role in initiation and exacerbation of DR [29]. Some published data by Jacqueline et al, 29 showed that diabetic conditions induce activation of autophagy followed by dysfunction, leading to cellular death. In their previously published work addressing the mechanism by which Muller cells exposed to high glucose release high amounts of VEFG and trigger increased apoptosis, it was shown that the autophagic process was defective in Muller cells among diabetic conditions. Xinxiao Gao and his group found that Atg16L1 may be a potential biomarker for the diagnosis and prognosis of DR [30]. It may serve as a potential therapeutic target blocking and slowing DR progression. On the other side, Nakhoul et al. found a significant increase in LC3 protein expression in the retinal GCL in diabetic mice and downregulated to basal levels by EMPA (SGLT2I) treatment [31].
Early in diabetes, loss of vascular autoregulation can lead to nutrient and oxygen deprivation of the inner retina. While defective blood flow is an early indicator of retinal dysfunction during diabetes. As the severity of diabetic retinopathy progresses, capillary non-perfusion leads to retinal ischemia, which, in turn, causes upregulation of pro-angiogenic cytokines that drive pathological intra-retinal and intravitreal neovascularization.
Recent Treatments
Ophthalmologists must follow diabetic patients with early stages of DR rigorously. Traditional therapies for DR include laser therapy, anti-VEGF, and vitrectomy. Other risk factors should be treated early and simultaneously with conventional drugs to control hyperglycemia, arterial hypertension, and hyperlipidemia. For patients with macular edema, recent sophisticated anti-vascular endothelial growth factor (anti-VEGF) drugs are in use to eliminate macular edema and improve vision. The worst cases are patients with fundus hemorrhage or proliferative vitreoretinopathy, for whom vitrectomy is the preferred treatment 3.
New therapies that target the early phase of diabetic retinopathy urgently needed to prevent the onset or slow the progression of diabetic retinopathy and, ultimately, blindness. A recent new anti-diabetic class of drugs has developed; the most in use in diabetic patients are the different sodium-glucose cotransporter type 2 inhibitors (SGLT2i) which mainly expressed in the kidney. Inhibition of the SGLT2 by the new antidiabetic drug (Empagliflozin) lowers plasma glucose levels mainly by increasing urinary and lower HbA1c. Apart from the glucose-lowering effect, there are other pleiotropic effects that lower body weight systolic blood pressure, reduce albuminuria, and stabilize the glomerular filtration rate (GFR). Recent advances showed the protective effects of these SGLT2Is in patients with diabetic retinopathy, by targeting the αKL and autophagy proteins in retinal layers cells [36,37].
GLP-1RA Such as Liraglutide can alleviate autophagy, which induced by oxidative stress; this protective effect is likely through the GLP-1R-ERK1/2-HDAC6 signaling pathway. Fan et al. showed that GLP-1 receptor agonists could alleviate retinal vascular leakage by protecting the blood-retinal barrier and reducing retinal vascular permeability in diabetic rats.14 However, the molecular mechanism of GLP-1RA treatment in DR not yet clarified, but increasing evidence indicates that GLP-1 has antioxidant effects. Recently Nanoparticles as a carrier for preventing and treating DR have shown some advantages in early diagnosis, carrying therapeutic drugs in targeting the retinal epithelial cells, to pass through the blood-retina barrier (BRB).35 More research needed to prove their efficacy in the early stages of DR.
Discussion
DR is the leading cause of blindness in the general population worldwide. Under diabetic conditions, hyperglycemia and the resulting glucose toxicity are the driving forces for inflammatory processes in the retina. Hyperglycemia activates oxidative stress and concomitantly increases reactive oxygen species release; all leading to injury to the retinal layer cells [1-5]. The deterioration in retinal function in PDR is irreversible and early diagnosis and treatments are needed.
It appears that Klotho and autophagy proteins may be involved in several physiological processes that can affect the generation and progression of DR. There is limited information on Klotho and autophagy pathways in the pathogenesis of DR [17-22]. In one recent cross-sectional study by Baolan Ji et al [36]. 4 in 60 patients with diabetes (of whom 33 had diabetic retinopathy), the authors observed that more advanced stages of diabetic retinopathy were associated with lower circulating αKlotho protein levels. Furthermore, Liu et al., 2018, also revealed that α-Klotho levels were significantly lower in patients with T2DM vs. non-diabetic controls, which supports these findings [38]. Moreover, a previous study demonstrated that serum Klotho levels were significantly lower in patients with HbA1c levels of ≥ 6.5 %, compared to in patients with HbA1c levels of 6.5% [38]. In our recent research, we found a decreased retinal αKL in the T2DM mice model. Klotho levels in mice with T2DM significantly decreased and restored by EMPA [31].
Others have shown that α-Klotho levels negatively correlated with the development of albuminuria (early-stage nephropathy) in patients with T2DM, which is consistent with the findings of several other studies. Down-regulation of α-Klotho in patients with diabetes reduces the inhibition of insulin and IGF-1 signaling pathways. The effects of high glucose on decreased klotho protein levels in retinal GCL is followed by excessively stimulated autophagy in retinal cells with increased LC3 protein levels, which may cause autophagy death cells, which may lead to advanced stages of DR and loss of vision. Therefore, preventing excessively stimulated autophagy at early stages by new treatments using nanotechnology systems may be of benefit to patients with DR [36-38]. More research needed to investigate the protective effects of the new anti-diabetic drugs as SGLT2Is and GLP-1RA, with the support of the nanoparticles as carriers in the early phases of DR.
References
- Zheng, Y., Ley, S. H., & Hu, F. B. (2018). Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nature reviews endocrinology, 14(2), 88-98.
- Chung, I. M., Rajakumar, G., Subramanian, U., Venkidasamy, B., Khanna, V. G., & Thiruvengadam, M. (2020). Insights on the current status and advancement of diabetes mellitus type 2 and to avert complications: An overview. Biotechnology and applied biochemistry, 67(6), 920-928.
- Diabetes Control and Complications Trial Research Group. (1995). The relationship of glycemic exposure (HbA1c) to the risk of development and progression of retinopathy in the diabetes control and complications trial. Diabetes, 44(8), 968-983.
- Leasher, J. L., Bourne, R. R., Flaxman, S. R., Jonas, J. B., Keeffe, J., Naidoo, K., ... & Vision Loss Expert Group of the Global Burden of Disease Study. (2016). Global estimates on the number of people blind or visually impaired by diabetic retinopathy: a meta-analysis from 1990 to 2010. Diabetes care, 39(9), 1643-1649.
- Antonetti, D. A., Klein, R., & Gardner, T. W. (2012). Mechanisms of disease diabetic retinopathy. New England Journal of Medicine, 366(13), 1227-1239.
- Cheung, N., Mitchell, P., & Wong, T. Y. Diabetic retinopathy.Lancet [Internet]. 2010 Jul 10; 376 (9735): 124–36.
- Tan, T. E., & Wong, T. Y. (2023). Diabetic retinopathy: Looking forward to 2030. Frontiers in Endocrinology, 13, 1077669.
- Lin, K. Y., Hsih, W. H., Lin, Y. B., Wen, C. Y., & Chang, T. J.(2021). Update in the epidemiology, risk factors, screening, and treatment of diabetic retinopathy. Journal of diabetes investigation, 12(8), 1322-1325.
- Wan, T. T., Li, X. F., Sun, Y. M., Li, Y. B., & Su, Y. (2015).Recent advances in understanding the biochemical and molecular mechanism of diabetic retinopathy. Biomedicine & pharmacotherapy, 74, 145-147.
- Ting, D. S. W., & Wong, T. Y. (2017). Proliferative diabetic retinopathy: laser or eye injection? Lancet (London, England), 389(10085), 2165-2166.
- Lin, K. Y., Hsih, W. H., Lin, Y. B., Wen, C. Y., & Chang, T. J.(2021). Update in the epidemiology, risk factors, screening, and treatment of diabetic retinopathy. Journal of diabetes investigation, 12(8), 1322-1325.
- Marsh S, Nakhoul F; Skorecki K, et al. Hypoxic induction of vascular endothelial growth factor is markedly decreased in diabetic individuals who do not develop retinopathy. Diabetes Care 2000; 23(9):1375–1380.
- Cheung N, Wong IY, Wong TY. Ocular anti-VEGF therapy for diabetic retinopathy: overview of clinical efficacy and evolving applications. Diabetes Care. 2014 Apr; 37(4):900-5.
- Xiangsheng C, Jingjing L, Mingzhu W, et al. GLP-1 Treatment Improves Diabetic Retinopathy by Alleviating Autophagy through GLP-1R-ERK1/2-HDAC6 Signaling Pathway.
- Kollias AN, Ulbig MW. Diabetic retinopathy: Early diagnosis and effective treatment. Dtsch Arztebl Int. 2010 Feb; 107(5):75-83;
- Ghamdi AHA. Clinical Predictors of Diabetic Retinopathy Progression; a Systematic Review.Curr Diabetes Rev. 2020; 16(3):242-247.
- Matsumura Y, Aizawa H, Shiraki-Iida T, et al. Identification of the human klotho gene and its two transcripts encoding membrane and secreted klotho protein. Biochem Biophys Res Commun 1998; 242: 626–630.
- Monica J, John Y, Nady G, et al. Klotho Regulates Retinal Pigment Epithelial Functions and Protects Against Oxidative Stress. The Journal of Neuroscience, October 9, 2013.
- Prud'homme GJ, Kurt M, Wang Q. Pathobiology of the Klotho Antiaging Protein and Therapeutic Considerations. .Front Aging. 2022 Jul 12; 3: 931331.
- Reish NJ, Maltare A, McKeown AS, et al. The Age-Regulating Protein Klotho Is Vital to Sustain Retinal Function. Invest Ophthalmol Vis Sci. 2013; 54:6675–6685.
- Mencke R, Hillebrands JL. The role of the anti-aging protein Klotho in vascular physiology and pathophysiology. Ageing Res Rev 2017; 35: 124–146.
- Slominski B, Ryba-Stanislawowska M, Skrzypkowska M, et al. The KL-VS polymorphism of the KLOTHO gene is protective against retinopathy incidence in patients with type 1 diabetes. Biochim Biophys Acta 2018; 1864: 758–763.
- Nakhoul N, Ertracht O, Igbariye A, et al. Potential Protective Effect of Empagliflozin on αKlotho/ Autophagy Protein LC3 in Diabetic Retinopathy: Evidence from Diabetic Mice Model. Diabetes Obes Int J,2022.
- Eskelinen EL and Saftig P: Autophagy: A lysosomal degradation pathway with a central role in health and disease. Biochim Biophys Acta 1793: 664-673, 2009.
- Boya P, Esteban-Martinez L, Serrano-Puebla A, et al. Autophagy in the eye: Development, degeneration, and aging. Prog Retin Eye Res 55: 206-245, 2016.
- Rosa MD, Distefano G, Gagliano C, et al. : Autophagy in Diabetic Retinopathy. Curr Neuropharmacol 14: 810-825,2016.
- Ding Y, and Choi ME. Autophagy in diabetic nephropathy. Journal of Endocrinology, (2015) 224, R15–R30.
- Sihao Ye, Yuhan Zhang, Xin Wang, Xu Liang, Mingan Wei, Rongrong Zong, Zuguo Liu and Qian Chen. Autophagy positively regulates Wnt signaling in mice with diabetic retinopathy. Experimental and Therapeutic Medicine 22: 1164, 2021.
- Jacqueline M. Lopes de Faria and Marcella Neves Dátilo. Deficient Autophagy Contributes to the Development of Diabetic Retinopathy. The Eye and Foot in Diabetes
- Xinxiao Gao, Yunhui Du, Wayne Bond Lau, Yu Li, Siquan Zhu, Xin-Liang Ma. Atg16L1 as a novel biomarker and autophagy gene for diabetic retinopathy. J Diabetes Res. 2021; 2021: 5398645.
- Mohamed Q, Gillies MC, and Wong TY: Management of diabetic retinopathy: a systematic review. JAMA. 2007; 298:902-916.
- Fante RJ, Gardner TW, Sundstrom JM. Current and future management of diabetic retinopathy: a personalized evidence-based approach. Diabetes Manag (Lond) 2013;3: 481–494.
- Rosberger DF. Diabetic retinopathy: current concepts and emerging therapy. Endocrinol Metab Clin North Am 2013; 42:721–745.\
- Yuxin Liu, Na Wu. Progress of Nanotechnology in Diabetic Retinopathy Treatment. International Journal of Nanomedicine 2021:16 1391–1403.
- Baolan Ji, Huili Wei, Yao Ding, Huimin Liang, Lu Yao, Hang Wang, Hua Qu, Huacong Deng. Protective potential of klotho protein on diabetic retinopathy: Evidence from clinical and in vitro studies. J Diabetes Investig 2020; 11: 162–169.
- Maria Kokkinaki, Mones Abu-Asab, Nishantha Gunawardena, Gerard Ahern, Monica Javidnia, John Young, and Nady Golestaneh. Kloto Regulates Retinal Pigment epithelial Functions and Protects against Oxidative Stress. The Journal of Neuroscience, October 9, 2013 • 33(41):16346 –16359
- Lingling Zhang and Tianming Liu. Low levels of circulating anti-aging hormone Klotho predict the onset and progression of diabetic retinopathy. Diabetes & Vascular Disease Research, November-December 2020: 1–4.
- Sridevi Devaraj, Basir Syed, Alexander Chien, Ishwarlal Jialal. Validation of an immunoassay for soluble Klotho protein: decreased levels in diabetes and increased levels in chronic kidney disease. Am J Clin Pathol 2012 Mar; 137(3):479-85