
Advancements in Journal of Urology and Nephrology(AJUN)
ISSN: 2689-8616 | DOI: 10.33140/AJUN
Impact Factor: 1.0



Research Article - (2024) Volume 6, Issue 1
Assessment of the Prevalence and Associated Factors of Chronic Kidney Disease at WURH, West Ethiopia, 2022 G C
2Department of Medicine, Addis Ababa University, Ethiopia
3Department of Medicine, Hayat Medical College, Ethiopia
4Master in Translational Medicine program, Department of Medicine, University of Barcelona, Ethiopia
5Department of Medicine, University of Gondar, Ethiopia
6Department of Internal Medicine, Zewditu Hospital, Ethiopia
7Department of Medicine Yekatite 12 Hospital Medical College, Ethiopia
8Department of Medicine, Haramaya University College of Health and Medical science, Ethiopia
9Department of Medicine, St. Paul’s Hospital Millennium Medical College, Ethiopia
Received Date: Dec 11, 2024 / Accepted Date: Feb 12, 2024 / Published Date: Feb 21, 2024
Copyright: ©Solomon Endale Dagnachew, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Dagnachew, S. E., Berhe, H. A., Tarekegn, T. K., Abdulkadir, S. I., Hailu, K. T., et al. (2024). Assessment of the Prevalence and Associated Factors of Chronic Kidney Disease at WURH, West Ethiopia, 2022 G C. Adv J Uro Nephro, 6(1), 01-10.
Abstract
Background: Chronic kidney disease (CKD) is defined as structural or functional abnormalities of the kidney that persist for at least three months and are manifested by either kidney damage (most frequently detected as persistent albuminuria or proteinuria) or a decreased glomerular filtration rate (GFR), which is < 60 ml/min per 1.73 m2. (1) . Chronic Kidney Disease (CKD) is a worldwide public health problem.
Objective: To determine the prevalence and associated factors of CKD Patients at WURH from November 14-28, 2022.
Methods: An institutional-based cross-sectional study of 208 chronic patients was conducted at WURH, which were found in the East Wollega zone, Nekemte town, Ethiopia between December 2021 to November 2022. All analyses and calculations Were performed using SPSS software (SPSS version 20). Data was presented as the means ±SDs for continuous variables and proportions for categorical variables. Demographic and clinical data were described. P values less than 0.05 at a 95% confidence interval were considered statistically significant.
Result: The magnitude of chronic kidney disease among the study participants was found that 53 (25.5%) of the participants had hypertension, of whom 60.2 had a follow-up, 22 (10.6%) had diabetes, all of whom were on follow-up, and 46 (22.1%) had cardiac problems. Serum creatinine level was determined for 193(92%) participants and 151(72.6%) had normal level while it was raised (>1.2mg/dl) in 42(20.2%). urine dipstick test for proteinuria was done for 109(52.4%) of the participants and the result showed that 40(36.7%) had +1 proteinuria,32(29.4%) had +2 and 21(19.3%) had +3 and above.
Conclusion: The prevalence of CKD in this study concludes that the disease become abundant and needs attention. The magnitude of the disease involves all age categories and is similarly common among males and females. Besides, CKD without any underlying associated factors appears abundant. CKD magnitude among patients with hypertension had statistical significance. Chronic kidney disease is rising at an alarming rate. Therefore, we recommend that relevant prevention, diagnostics, and therapeutic measures must be undertaken in all health facilities.
Keywords
Assessment, Prevalence, Associated Factors, Chronic, Kidney Disease.
Acronyms and Abbreviations
BMI : Body Mass Index
CKD : Chronic Kidney Disease
CVD : Cardiovascular Disorder
CC : Creatinine Clearance
CD : Chronic Disease
DM : Diabetics Mellitus
ESRD : End Stage Renal Disease
HTN : Hypertension
WHO : World Health Organization
Introduction
Background
Chronic kidney disease (CKD) is defined as structural or functional abnormalities of the kidney that persist for at least three months and are manifested by either kidney damage (most frequently detected as persistent albuminuria or proteinuria) or a decreased glomerular filtration rate (GFR), which is < 60 ml/min per 1.73 m2. [1]. Chronic Kidney Disease (CKD) is a worldwide public health problem [2]. Kidney diseases are a leading cause of death in the United States. About 37 million US adults are estimated to have CKD, and most are undiagnosed. 40% of people with severely reduced kidney function (not on dialysis) are not aware of having CKD. Every 24 hours, 360 people begin dialysis treatment for kidney failure [3]. Chronic kidney disease is now recognized as a global public health problem. It is associated with a range of adverse outcomes, including increased all-cause mortality, cardiovascular disease, progression to end-stage renal disease (ESRD), acute kidney injury, anemia, cognitive decline, and overall mortality [4]. The prevalence of CKD varies, and accurate prevalence estimates are difficult to obtain, especially concerning fulfilling the chronicity criterion (reduced eGFR ≥ 90 days). Traditional risk factors for CKD are well described, and non-traditional risk factors such as socio-economic status (SES), health literacy, and rurality are gaining interest [5].
Glomerular filtration rate (GFR) remains the ideal marker of kidney function. Unfortunately, measuring GFR is time-consuming; therefore, GFR is usually estimated from equations that consider endogenous filtration markers like serum creatinine (S. Cr) and cystatin C (CysC). Other biomarkers, such as albuminuria, may precede kidney function decline and have been demonstrated to have strong associations with disease progression and outcomes [6]. Glomerular filtration is the physiological process of making an ultra-filtrate of blood as it flows through the glomerular capillaries. Glomerular filtration rate (GFR) measures the speed at which substances are filtered from the blood into the urine [7]. Estimated GFR (eGFR) is regarded as an honest laboratory tool to point out abnormality of kidney function which will be calculated from serum creatinine level [8]. In the United States, diabetes and high blood pressure are the leading causes of kidney failure, accounting for 3 out of 4 new cases. Heart Disease, Family history of CKD, and Obesity are other factors [3].
Statement of the Problem
Chronic kidney disease (CKD) has been recognized as a leading public health problem worldwide. CKD directly affects the global burden of morbidity and mortality worldwide. The increase in the prevalence of diabetes mellitus, hypertension, obesity, and aging mainly drives the worldwide growth of this disease. The large number of deaths due to poor access to renal replacement therapy in developing countries persons with CKD have significantly higher rates of morbidity, mortality, hospitalizations, and healthcare utilization [9]. The rapid rise of common risk factors such as diabetes, hypertension, and obesity, especially among people with low incomes, results in even more significant and more profound burdens that developing nations are not equipped to handle [10].
Chronic renal failure (CRF), a non-communicable disorder included in the plan, is ranked 18th among the global causes of death it was ranked 27th in 2011, and the number of deaths from CRF has risen by 82% during that time. It is the third among the top 25 causes of death, next to HIV/AIDS and diabetes [11]. In Ethiopia, data on the burden and determinants of chronic kidney disease (CKD) in the general population is limited. The prevalence of CKD was high in the study area. Only hypertension and age ≥40 years old were significantly associated with CKD. More of the increased prevalence of CKD in the current study remained unexplained and deserves further study [12]. prevalence and related factors of CKD among renal patients that attend public hospitals of Addis Ababa have been studied. CKD prevalence was greater among older persons and persons with diabetes, cardiovascular disease, and hypertension than among persons without these conditions [2].
A study done in Addis Ababa shows that the prevalence of CKD was 22.4%, slightly more than one in five, and one in ten patients who visited the renal unit for renal consultations had CKD. Patients with urinary tract obstruction, hypertension, D.M., CVD, having a family history of CKD, and age (â?»60 years old) were more likely to develop CKD [12].
Significance of the Study
Early screening, Detection, and identification of kidney disease risk groups in Ethiopia are rare. Currently, sudden hearing of kidney failure and death due to CKD and its complications have become common. Therefore, early Detection of CKD risk patients is critical to minimize the burden on the community from it. In addition, the findings will be relevant to policymakers, healthcare providers, and payers who must allocate resources to manage the associated factors and support ongoing efforts to reduce the prevalence of CKD. Moreover, it will help as baseline data for further research in the future.
Literature Review
Prevalence of CKD
Chronic kidney disease (CKD) is an increasingly major global health problem. Globally, the estimated overall prevalence of CKD is 8% to 16%, and this corresponds to nearly 500 million individuals, of whom 78% reside in low- to middle-income countries. CKD is associated with increased risks of mortality and cardiovascular events [13]. kidney disease affects an estimated 37 million people in the U.S. (15% of the adult population; more than 1 in 7 adults [14]. Prevalence of adults with CKD was 5.6% – 5.8%. The cohort's average age (± S.D.) was 75 ± 11 years, 64.6% were female, and the average eGFR was 47.32 ± 11.53 mL/min/1.73m2 [5]. Nearly a quarter (13.2%) of the sub-Saharan population has CKD, while its magnitude among diabetic and hypertensive patients is 24.7% and 34.5%, respectively [15].
Ethiopia, as one of the developing countries, has been showing changes that shift the lifestyle of the people towards urbanization, particularly in recent decades. These rapid changes have led to 4 the emergence of non-communicable chronic diseases like D.M. Recent systematic review shows the prevalence of diabetes in Ethiopia ranged from 2.0% to 6.5% [16]. The pooled estimate of chronic kidney disease among patients with chronic illnesses in Ethiopia is 21.71% (95% confidence interval: 17.67, 25.74 Stage (1-2) prevalence of CKD is 27.2%, (15.6% and 11.6%) respectively. Whereas stage (3-4) prevalence of CKD is 34.1%, (19.4%, and 14.7%) respectively to CKD EPI equation [2]. The overall prevalence of CKD was 20.5% with (16% - 25%) study done in Ambo town [17,18].
Factors Associated with CKD
Many factors are reported to be associated with the occurrence of CKD. According to survey results from previous reports in two Dutch primary health care centers, it was 27.5% among people with diabetes and 21.1% in hypertensive cholesterol level, body mass index (BMI), uncontrolled blood pressure age > 60, associated with chronic kidney diseases [19,20]. The history of diabetes (18.2%), hypertension, 60%and cardiovascular disease (19.4%) of respondents among kidney patients in public hospitals and crude and adjusted odd ratio of factors associated with CKD of respondents among kidney patients in public hospitals, Addis Ababa [2].
Renal Function Assessment
Most kidney diseases don't have symptoms or findings until later in their course and are detected only when chronic [21]. Early Detection of renal impairment, therefore, it is crucial to ensure measures to prevent or delay disease progression and reduce the risk of adverse outcomes [20]. The KDOQI guidelines recommend screening high-risk populations, which include individuals with Hypertension, Diabetes Mellitus, and those older than 65 years [19].
1. Serum Creatinine: Increased serum creatinine levels often predict kidney dysfunction because the kidneys are the first means for eliminating waste products of metabolism that are no longer needed by the body, such as creatinine, urea, and others. Serum creatinine is a product of phosphocreatine during muscular activity [21]. Serum creatinine remains constant for the average healthy subject between 20 and 70 years of age, with a mean of 0.90 mg/ dL and normal reference interval (0.63–1.16 mg/dL) for (white) men and with a mean of 0.70 mg/dL and average reference interval (0.48–0.93 mg/dL) for (white) women [22].
2. Blood Urea Nitrogen (BUN): Blood urea nitrogen (BUN) was reported to be associated with mortality in heart failure. Patients. An optimal cut-off was calculated at 28 mg/dL, which was associated with adverse Outcome [23].
3. Estimated glomerular filtration rate (eGFR): Glomerular filtration rate (GFR) measures how substances are filtered from the blood into the urine [7]. Several researchers publish many formulas to estimate GFR from serum creatinine and serum cystatin C, but the most studied and widely used formulas in adults are Cock croft –Gault (C-G), Modification of Diet in Renal Disease (MDRD), and Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) study equations [24].
• GFR Estimation by Cockcroft-Gault Formula: The Cockcroft-Gault formula was developed in 1973 using data from 249 men with creatinine clearance (CC) from approximately 30 to 130 mL/ m2. This formula considers three variables that affect GFR (age, weight, and sex) but is not adjusted for body surface area. The C-G formula is:

Where CC is expressed in milliliters per minute, age in years, weight in kilograms, and serum creatinine (Sc) in milligrams per deciliter [25].
4. Proteinuria or Albuminuria: Proteinuria is another type of kidney function test that helps see if the kidneys leak proteins into the urine. Persistent proteinuria is a defining marker of renal injury regardless of estimated GFR, and it identifies increased cardiovascular disease and mortality risks [24]. Urinary protein excretion can be measured as total protein (24-hour urine collection) or albumin to creatinine ratio in a spot urine sample. While an accurate 24-hour urine collection is the "gold standard" for measurement of albuminuria, the measurement of albumin to creatinine ratio in a spot first-morning urine sample is often more practical to obtain and correlates well, but not perfectly with 24-hour urine collections [26]. Measurement of proteinuria with the entire protein/creatinine ratio is a less sensitive method than the spot albumin/creatinine ratio and includes filtered albumin, tubular secreted proteins (Tamm-Horsfall protein), and plasma proteins from other disease processes, such as multiple myeloma and infection [24].
Diagnosis and Staging of CKD
Early Detection and treatment of chronic kidney disease can prevent or minimize complications associated with CKD [27]. CKD diagnosis and staging are a critical step to working out the prognosis, evaluation, and management of CKD [24].
|
GFR category |
(ml/min/1.73m2) |
Term |
|
G1 |
≥90 |
Normal |
|
G2 |
60-89.9 |
Mildly decreased |
|
G3a |
45-59 |
Mildly to moderately decreased |
|
G3b |
30-44 |
Moderately to Severely decreased |
|
G4 |
15-29 |
Severely decreased |
|
G5 |
<15 |
Kidney failure |
Table 1: GFR Categories in CKD Patients
|
Category |
AER (mg/24hrs) |
ACR (mg/mmol) |
ACR (mg/g) |
Terms |
|
A1 |
<30 |
<3 |
<30 |
Normal or mildly increased |
|
A2 |
30-300 |
3-30 |
30-300 |
Moderately increased |
|
A3 |
>300 |
>30 |
>300 |
Severely increased |
Table 2: Albuminuria Categories in CKD
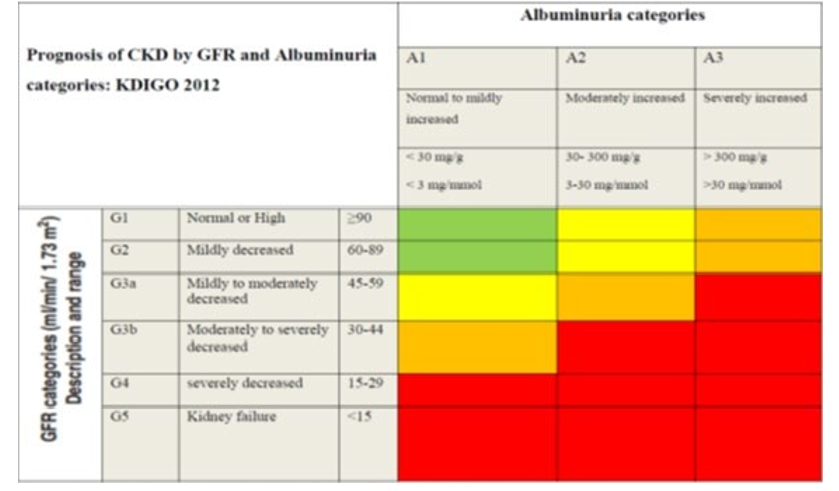
Table 3: A classification of CKD Adopted from KDIO 2021 Guideline
Green: Low Risk (If No Other Markers of Kidney Disease, No CKD), Yellow: Moderately Increased Risk, Orange: High Risk, Red: Very High Risk
Objectives of the Study
General Objective
• To determine the prevalence and associated factors of CKD Patients at WURH from November 14-28, 2022
Specific Objectives
• To determine the prevalence of CKD patients
• To identify the related factors of CKD
Methods And Materials
Study Area and Period
The study was conducted at WURH, in the East Wollega zone, Nekemte town. The town is located 328 km west of Addis Ababa. The astronomical location of this town on the map is 9-degree 04'North latitude and 36-degree 30' North West latitude. Its altitude ranges from 1960-2170 above sea level, and annual rainfall ranges from 1500 mm-2200 mm, which covers the months from April to the beginning of December. WURH provides inpatient and outpatient services in 4 different significant departments and four other specialty clinics that offer outpatient services, like psychiatry, ophthalmology, dermatology, and dental clinics. In the last three years, the hospital served 95348 clients. The hospital is staffed by 31 specialists, 49 G.P.s, 126 Nurses, 28 Midwives, 24 lab personnel, 24 pharmacy personnel,18 other professionals and 303 supportive staff. The study was conducted from November 14-28/2022.
Study Design
This study was an institutional-based cross-sectional study.
Source and Study Population
The source population was any medical patients visiting WURH from December 2021 to November 2022. Medical patients admitted to the WURH medical ward from December 2021 to November 2022 were the study population.
Inclusion and Exclusion Criteria
Inclusion Criteria
Adult Patients managed at the hospital inpatient department in the past year with at least one serum creatinine determined were included.
Exclusion Criteria
Incomplete patient charts. Patients aged less than 18 years
Sample Size Determination
The sample size is determined for the prevalence of CKD by a single proportion formula.
n = (z2p(1-p) )
( w2 )
n= ((1.96)2(0.205) (0.795) )
(0.05×0.05)= 250
Where n = sample size p = taken from a study done at Ambo town (0.205)
w = margin of error/level of precision (0.05)
Z= Reliability coefficient for 95% level of confidence (1.96)
Correction sample size is equal to
n
(1+n/N)= 1+250/1200 = 208
Where n = largest sample size
N = Total medical patients admitted in one year.
Therefore, the final sample size will be 208
Sampling Technique and Procedures
Adult Patients (>18 years of age) admitted to the medical ward are considered study participants. Systematic random sampling was used to recruit the study participants. All realized medical patients in the past year numbered 1-1200, then divided into sample units, 1200÷208. This gives calculated k to be 6. So, every six-patient card was selected, and data was collected until the sample size was fully fulfilled. The first card was determined by lottery method from numbers 1-6. All adult patients have an equal chance to participate in the study.
Data Collection Procedure
Data was collected through a structured questionnaire from patient cards. Before the data collection, data collectors were trained well to have a common understanding of each question. A trained supervisor supervised the data collection. A pretest was done at WURH, and any ambiguity or confusion on the questionnaires was amended.
Study Variables
Dependent Variable (outcome)
• Chronic kidney disease
Independent Variables
• Age, sex, smoking, and alcohol consumption, Knowledge about CKD, family history of CKD, cardiac problems, kidney infection, diabetic and hypertension status.
Operational Definitions of the Variables
Chronic kidney disease is defined as pathological abnormalities or damage markers, including abnormalities in blood or urine tests or GFR < 60 ml/min/`1.73 m2 for ≥ three months. Adult patients: Patients who attend the Medical ward at WURH aged≥ 18 Hypertension; blood pressure ≥ 140/90 mmHg or medical history of Hypertension Proteinuria: Urinary protein excretion more significant than 300 mg/24hrs Smoking Status: Current Smoker: >1 cigarette/day.
Data Analysis Procedures
All analyses and calculations Were performed using SPSS software (SPSS version 20). Data was presented as the means ±SDs for continuous variables and proportions for categorical variables. Demographic and clinical data were described. The odds ratio (OR) between the factors and CKD was calculated using binary logistic regression analysis for critical demographic data, BMI, and clinical cases, which are well-known risk factors for CKD. P values less than 0.05 at a 95% confidence interval were considered statistically significant. Finally, a multivariate analysis model was used to identify the factors associated with the development of chronic kidney disease.
Data Quality Assurance Procedures
The data collectors were medical interns assigned to the group. There was a Supervisor from the department of Internal medicine. The supervisor gave orientation for data collectors. Orientation was given to the supervisor separately on supervising the data collectors, checking for completed questionnaires, and correcting any mistakes or problems.
Ethical Consideration
Permission for the study was obtained from the Ethics Committee of the School of Public Health, Wollega University. Ethics approval also from the Wollega University Hospital internal research review board. Names are not used, and confidentiality is maintained by keeping data collection forms locked in a secure cabinet.
Dissemination of the Result
The study result will be submitted to the University Referral Hospital and Wollega University Institute of Health Sciences Department of Public Health.
Result
Socio-Demographic Characteristics
A total of 208 patient charts were addressed in the study, with a 100% response rate. Of the participants, 96 (46.2%) were males and 112 (53.8%) were females. Of the participants, 90(43.3%) were over 47 years old. Study participants are predominantly from rural areas (57.7%) and 88(42.3%).
|
Characteristics |
Frequency |
Percent |
|
|
sex |
Male |
96 |
46.2 |
|
Female |
112 |
53.8 |
|
|
Age |
18-34 |
50 |
24.0 |
|
35-41 |
43 |
20.7 |
|
|
41-47 |
25 |
12.0 |
|
|
>47 |
90 |
43.3 |
|
|
Residence area |
Urban |
88 |
42.3 |
|
Rural |
120 |
57.7 |
|
Table 4: Socio-Demographic Characteristics of Adult Patients in WURH Inpatient Ward, 2022
Clinical Characteristics of Participants
It was found that 53 (25.5%) of the participants had hypertension, of whom 60.2 had a follow-up, 22 (10.6%) had diabetes, all of whom were on follow-up, and 46 (22.1%) had cardiac problems. Serum creatinine level was determined for 193(92%) participants and 151(72.6%) had normal level while it was raised (>1.2mg/ dl) in 42(20.2%). urine dipstick test for proteinuria was done for 109(52.4%) of the participants and the result showed that 40(36.7%) had +1 proteinuria, 32(29.4%) had +2 and 21(19.3%) had +3 and above.
|
C.K. vs Proteinuria |
Chronic kidney disease |
Total |
||
|
yes |
No |
|||
|
protienuria |
trace |
0 |
16 |
16 |
|
0.0% |
100.0% |
100.0% |
||
|
+1 |
1 |
39 |
40 |
|
|
2.5% |
97.5% |
100.0% |
||
|
+2 |
12 |
20 |
32 |
|
|
37.5% |
62.5% |
100.0% |
||
|
+3 |
13 |
8 |
21 |
|
|
61.9% |
38.1% |
100.0% |
||
|
Total |
26 |
83 |
109 |
|
|
23.9% |
76.1% |
100.0% |
||
Table 5: Proteinuria in Adult Patients Admitted to WURH Medical Ward, 2022
In our study, abdominal ultrasound was done for 179(86.1%) of the participants, of whom 20 (11.2%) had evidence of decreased kidney size while average size in others (88.8%). Evidence of anemia (hemoglobin level) was determined for the participants and summarized in the table below.
|
Hemoglobin Level |
Frequency |
Percent |
|
<=7g/dl |
37 |
17.8 |
|
7-9.9g/dl |
12 |
5.8 |
|
10-11.9g/dl |
20 |
9.6 |
|
>=12g/dl |
139 |
66.8 |
|
Total |
208 |
100.0 |
Table 6: Hemoglobin Level of Adult Patients Admitted to WURH Medical Ward, 2022
Prevalence of CKD
From the total number of participants, the assessed prevalence of CKD was 29 (13.9%). of real CKD cases, only one person had dialysis. Prevalence of CKD by age group was higher among >47 years (44.8%) and 35-41 years (20.6%), 18-34years (20.6%) ,41-47(13.8%). Gender results illustrate that CKD is almost similar for both sexes, male (48.3%) and female (51.7%). CKD cases related to 10 (45.5%%) cases of Diabetic mellitus and 5 (17.2 %) of patients with cardiac problems. CKD prevalence was 3.4% in kidney infection, and 21(72.4%) of CKD patients had hypertension. Table 4 stage of CKD patients admitted to WURH medical ward, 2022
|
Stage of CKD |
What was eGFR |
Total |
|
||||||
|
>=90 |
60-90 |
45-59 |
30-44 |
15-30 |
<15 |
|
|||
|
hronic kidney disease |
yes |
Count |
|
2 |
6 |
6 |
7 |
8 |
29 |
|
% CKD |
6.9% |
20.7% |
20.7% |
24.1% |
27.6% |
100.0% |
|||
Table 7: Stage of CKD Patients Admitted to WURH Medical Ward 2022
|
Variables |
with CKD (N=29) |
without CKD (N=179) |
|
HTN |
||
|
yes |
21(39.6%) |
32(60.4%) |
|
No |
8(5.2%) |
147(94.8%) |
|
D.M. |
||
|
Yes |
10(45.5%) |
12(54.5%) |
|
No |
19(10.2%) |
167(89.8%) |
|
Cardiac Problem |
||
|
Yes |
5(10.9%) |
41(89.1%) |
|
No |
24(14.8%) |
138(85.2%) |
Table 8: Clinical Characteristics of CKD among those Admitted to WURH Medical Ward 2022
Associated Factors for CKD
Bivariate and multivariate logistic regression was performed to examine the relationship between CKD and the independent variables (age, sex, smoking status, alcohol drinking status, family history of CKD, BMI, HTN, D.M., cardiac problem, kidney infection history, and knowledge of kidney function and disease. CKD cases with hypertension were 5% (AOR =95%CI 0.052, (0.014,0.195), P=0.04) more likely to be associated with chronic kidney disease than patients without HTN. In comparison, D.M. patients were 7% AOR [95% CI] 0.073(0.017,0.31) more associated than patients without D.M.
Besides, no statistically significant differences were seen with CKD participants about age COR [95% CI] 0.939[0.682, 1.293], sex COR [95% CI] 1.104 [0.503, 2.422]. Smoking use COR [95% CI] 2.66[0.871, 8.126], alcohol drinking COR [95% CI] 1.487 [0.514, 4.299], family history COR [95% CI] 8.6[0.25, 1.08] and cardiac had COR [95% CI] 0 .701[0.252, 1.954].
|
Variables |
CKD |
COR 95% CI |
P-value |
|
|
YES |
NO |
|||
|
AGE |
||||
|
18-34 |
6 |
44 |
1.238(.439,3.488) |
.967 |
|
35-41 |
6 |
37 |
1.041(.367,2.957) |
.686 |
|
41-47 |
4 |
21 |
.886(.262,3.003) |
.940 |
|
>47 |
13 |
77 |
1 |
|
|
SEX |
||||
|
Male |
14 |
82 |
1.104(0.503,2.422) |
0.805 |
|
Female |
15 |
97 |
1 |
|
|
Smoking status |
||||
|
Yes |
5 |
13 |
2.66(0.871,8.126) |
0.08 |
|
No |
24 |
166 |
1 |
|
|
Alcohol use |
||||
|
Yes |
5 |
22 |
1.467(0.514,4.299) |
0.0464 |
|
No |
24 |
157 |
1 |
|
|
HTN |
||||
|
Yes |
21 |
8 |
12.059(4.905,29.648) |
0.00 |
|
No |
32 |
147 |
1 |
|
|
D.M. |
||||
|
Yes |
10 |
19 |
7.325(2.793,19.208) |
0.00 |
|
No |
12 |
167 |
1 |
|
|
Cardiac Problem |
||||
|
Yes |
5 |
24 |
0.701(0.252,1.954) |
0.0497 |
|
No |
41 |
138 |
1 |
|
Table 9: Bivariate Logistic Regression Predictors of CKD Patients Admitted to WURH Medical Ward 2022
Multivariate Analysis
After incorporating all significant (p<0.20) in addition to age and sex, which are relevant biological variables in the bivariate analysis, multivariate logistic regression was performed to identify risk factors independently associated with CKD. The multiple logistic regression model included the following variables: HTN and D.M. were significantly associated with the occurrence of chronic kidney disease. In multivariate analysis, HTN and D.M. developed the disease at a statistically significant P value < 0.05. (AOR = 0.036, 95% CI 0.007, 0.175, P<0.00) and (AOR =0.011; 95% CI 0.002, 0.054; P<0.00).
|
Variables |
CKD |
COR 95% CI |
AOR 95%CI |
P-value |
|
|
YES |
NO |
||||
|
AGE |
|||||
|
18-34 |
6 |
44 |
1.238(.439,3.488) |
0.442(0.095,2.055) |
.298 |
|
35-41 |
6 |
37 |
1.041(.367,2.957) |
1.602(0.235,10.901) |
.63 |
|
41-47 |
4 |
21 |
.886(.262,3.003) |
0,439(0.09,2.151) |
.310 |
|
>47 |
13 |
77 |
1 |
1 |
|
|
SEX |
|||||
|
Male |
14 |
82 |
1.104(0.503,2.422) |
1.052(0.321,3.446) |
0.933 |
|
Female |
15 |
97 |
1 |
1 |
|
|
Smoking status |
|||||
|
Yes |
5 |
13 |
2.66(0.871,8.126) |
0.351(0.033,3.789) |
0.388 |
|
No |
24 |
166 |
1 |
1 |
|
|
Alcohol use |
|||||
|
Yes |
5 |
22 |
1.467(0.514,4.299) |
12.711(0.506,319.2) |
0.122 |
|
No |
24 |
157 |
1 |
1 |
|
|
HTN |
|||||
|
Yes |
21 |
8 |
12.059(4.905,29.648) |
0.052(0.014,0.195) |
0.00 |
|
No |
32 |
147 |
1 |
1 |
|
|
D.M. |
|||||
|
Yes |
10 |
19 |
7.325(2.793,19.208) |
0.073(0.017,0.31) |
0.00 |
|
No |
12 |
167 |
1 |
1 |
|
|
Cardiac Problem |
|||||
|
Yes |
5 |
24 |
0.701(0.252,1.954) |
1.693(0.360,7.982) |
0.504) |
|
No |
41 |
138 |
1 |
1 |
|
Table 10: Multivariate Regression Analysis of Factors Associated with CKD Patients Admitted to WURH Medical Ward 2022
Discussions
Prevalence of CKD
In this hospital-based quantitative cross-sectional study, CKD prevalence and associated factors among patients admitted to the medical ward were assessed. This study revealed that the prevalence of CKD was 13.9 %. The prevalence of CKD in Studies from world and sub-Saharan Africa encompasses 8 to 16% and 13.2% respectively [15,17]. It was almost comparable with these findings.
Associated Factors for CKD
This study illustrates CKD is Co-morbid with chronic illness, particularly hypertension and D.M. CKD cases with hypertension were 5% higher than without hypertension (AOR =95%CI 0.052, (0.014,0.195), P=0.04). Among 29 CKD patients, 21 (72.4%) had hypertension. This is higher than study one in Addis Ababa, which was 60% (2). This may be due to the data being collected from patient charts, while a study in Addis was by interview. D.M. patients were 7% AOR [95% CI] 0.073(0.017,0.31), more associated with CKD than those without it, and 45.5% of CKD patients had D.M. These studies revealed more association between them than the study done at two Dutch primary health care centers [21]. This study's multivariate analysis result shows kidney infection, BMI, age, smoking, and sex had no statistically significant association, according to our research. This may be a need for complete documentation.
Strengths and Limitations of the Study
Strength
• The study can show the load of the disease.
• The study can contain multiple variables to see the associated factors.
Limitation
A facility-based study affects the reliability of the prevalence of CKD obtained, so it needs a population-based study.
• The study populations were patient cards, which can affect the accuracy of some data.
• With single-facility results, it can be not easy to generalize.
Conclusion
The prevalence of CKD in this study concludes that the disease become abundant and needs attention. The magnitude of the illness involves all age categories and is similarly common among males and females. Besides, CKD without any underlying associated factors appears abundant. CKD magnitude among patients with hypertension had statistical significance. Chronic kidney disease is rising at an alarming rate. Therefore, we recommend that relevant prevention, diagnostics, and therapeutic measures must be undertaken in all health facilities.
Recommendation
According to our findings, Hypertension and D.M. were significantly associated with CKD. Facing this, we recommend health professionals improve primary care treatment and follow¬up of patients with hypertension, and the D.M. Ministry of Health must take assignment on the increment of Levels of awareness and knowledge among patients and providers must regard CKD and its many consequences. Periodic medical evaluation of the society must be advocated for early management and Detection by health professionals and key informants.
References
- Brosius 3rd, F. C. (2006). American Heart Association Kidney and Cardiovascular Disease Council; Council on High Blood Pressure Research; Council on Cardiovascular Disease in the Young; Council on Epidemiology and Prevention; Quality of Care and Outcomes Research Interdisciplinary Working Group: Detection of chronic kidney disease in patients with or at increased risk of cardiovascular disease: a science advisory from the American Heart Association Kidney And Cardiovascular Disease Council; the Councils on High Blood Pressure Circulation, 114(10), 1083-1087.
- Kore, C., & Yohannes, H. M. (2018). Prevalence of chronic kidney disease and associated factors among patients with kidney problems public hospitals in Addis Ababa, Ethiopia. JKidney, 4(01), 1-5.
- Johnson, N. B., Hayes, L. D., Brown, K., Hoo, E. C., & Ethier,K. A. (2014). CDC National Health Report: leading causes of morbidity and mortality and associated behavioral risk and protective factors—United States, 2005–2013.
- Ferguson, T. S., Tulloch-Reid, M. K., Younger-Coleman,N. O., Wright-Pascoe, R. A., Boyne, M. S., Soyibo, A. K., & Wilks, R. J. (2015). Prevalence of chronic kidney disease among patients attending a specialist diabetes clinic in Jamaica. The West Indian medical journal, 64(3), 201.
- So, B. H. (2018). Chronic kidney disease: determining chronicity, prevalence, variation and survival in a community chronic kidney disease (CKD) cohort (Doctoral dissertation, University of Glasgow).
- Lopez-Giacoman, S., & Madero, M. (2015). Biomarkers in chronic kidney disease, from kidney function to kidney damage. World journal of nephrology, 4(1), 57.
- Onwubuya, E. I., Ukibe, N. R., Kalu, O. A., Ukibe, S. N., & Obasi, I. J. (2018). Assessment of kidney function, estimated glomerular filtration rate and body mass index in HIV seropositive subjects on antiretroviral therapy in Nnewi. Int J Pharm Pharm Sci, 10, 44-9.
- Levey, A. S., Becker, C., & Inker, L. A. (2015). Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: a systematic review. Jama, 313(8), 837-846.
- Lv, J. C., & Zhang, L. X. (2019). Prevalence and disease burden of chronic kidney disease. Renal fibrosis: mechanisms and therapies, 3-15.
- Natalia, A., Giovänio, V., Angela, M., Geraldo, P. (2014). Prevalence and factors associated with chronic renal failure among hospitalized patients in a university hospital in the city of São Paulo, Brazil.
- Perico, N., & Remuzzi, G. (2014). Chronic kidney disease in sub-Saharan Africa: a public health priority. The Lancet Global Health, 2(3), e124-e125.
- Kebede, K. M., Abateneh, D. D., Teferi, M. B., & Asres, A. (2022). Chronic kidney disease and associated factors among adult population in Southwest Ethiopia. Plos one, 17(3), e0264611.
- Stanifer, J. W., Muiru, A., Jafar, T. H., & Patel, U. D. (2016). Chronic kidney disease in low-and middle-income countries. Nephrology Dialysis Transplantation, 31(6), 868-874.
- Cruz, D. A DIETITIANS’PERSPECTIVE: UNDOCUMENT-ED PATIENTS WITH CHRONIC KIDNEY DISEASE.
- Hailu, H. E., Dinku, B., Wondimu, J., & Girma, B. (2022). Prevalence and Associated Factors of Chronic KidneyDisease Among Diabetic and Hypertensive Patients at Ambo Town Public Hospitals of West Shewa Zone, Oromia Region, Ethiopia.
- Bishu, K. G., Jenkins, C., Yebyo, H. G., Atsbha, M., Wubayehu, T., & Gebregziabher, M. (2019). Diabetes in Ethiopia: a systematic review of prevalence, risk factors, complications, and cost. Obesity Medicine, 15, 100132.
- Animaw, Z., Melese, A., Demelash, H., Seyoum, G., & Abebe,(2021). Intestinal parasitic infections and associated factors among pregnant women in Ethiopia: a systematic review and meta-analysis. BMC Pregnancy and Childbirth, 21(1), 1-13.
- Hailu, H. E., Dinku, B., Wondimu, J., & Girma, B. (2022). Prevalence and Associated Factors of Chronic Kidney Disease Among Diabetic and Hypertensive Patients at Ambo Town Public Hospitals of West Shewa Zone, Oromia Region, Ethiopia.
- Milik, A., & Hrynkiewicz, E. (2014). On translation of LD, IL and SFC given according to IEC-61131 for hardware synthesis of reconfigurable logic controller. IFAC Proceedings Volumes, 47(3), 4477-4483.
- Fiseha, T., Mengesha, T., Girma, R., Kebede, E., & Gebreweld,(2019). Estimation of renal function in adult outpatientswith normal serum creatinine. BMC Research Notes, 12, 1-6.
- Bargnoux, A. S., Kuster, N., Cavalier, E., Piéroni, L., Souweine, J. S., Delanaye, P., & Cristol, J. P. (2018). Serum creatinine: advantages and pitfalls. J Lab Precis Med, 3(8), 71.
- Delanaye, P., Cavalier, E., & Pottel, H. (2017). Serum creatinine: not so simple! Nephron, 136(4), 302-308.
- Arihan, O., Wernly, B., Lichtenauer, M., Franz, M., Kabisch, B., Muessig, J., ... & Jung, C. (2018). Blood Urea Nitrogen (BUN) is independently associated with mortality in critically ill patients admitted to ICU. PloS one, 13(1), e0191697.
- Gaitonde, D. Y., Cook, D. L., & Rivera, I. M. (2017). Chronic kidney disease: detection and evaluation. American family physician, 96(12), 776-783.
- Berns, J. S. (2015). Improving care of patients with CKD: The 2015 National Kidney Foundation presidential address. American Journal of Kidney Diseases, 66(4), 547-551.
- Harison 21 th ed,2022
- Kumela Goro, K., Desalegn Wolide, A., Kerga Dibaba, F., Gashe Fufa, F., Wakjira Garedow, A., Edilu Tufa, B., & Mulisa Bobasa, E. (2019). Patient awareness, prevalence, and risk factors of chronic kidney disease among diabetes mellitus and hypertensive patients at Jimma University Medical Center, Ethiopia. BioMed Research International, 2019.