
International Journal of Media and Networks(IJMN)
ISSN: 2995-3286 | DOI: 10.33140/IJMN
Impact Factor: 1.02



Research Article - (2024) Volume 2, Issue 5
Assessment of Bacterial Hand Contamination and Associated Factors Among Food Handlers Working in Catering Establishments of Hosanna Town, Hadiya Zone, South Ethiopia, 2023
2Department head of Medical Laboratory Science, Hossana college of health Science, Ethiopia
3Health Extension team Coordinator, Hossana college of Health Science, Ethiopia
Received Date: May 21, 2024 / Accepted Date: Apr 25, 2024 / Published Date: May 20, 2024
Copyright: ©Â©2024 Ashenafi Woime, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Woime, A., Kedir, R., Girma, A. (2024). Assessment of Bacterial Hand Contamination and Associated Factors Among Food Handlers Working in Catering Establishments of Hosanna Town, Hadiya Zone, South Ethiopia, 2023. Int J Med Net, 2(5), 01-11.
Abstract
Background: Hands are the major source of contamination, which can never be totally free of microorganisms, especially bacteria. Food can become contaminated by dirty hands if there is a lack of proper hygiene among the food handlers when handling food. Human hands are in regular contact with the surrounding environment, and a variety of pathogens can reach the mucous membranes in the mouth, nose, eyes, and genitals of humans through the hands and consequently contribute to foodborne illness outbreaks.
Objective: This study assessed bacterial hand contamination and associated factors among food handlers working in catering establishments in Hossana Town, South Ethiopia.
Method: A community-based cross-sectional study was conducted among food handlers at catering establishments in Hosanna town, Hadiya zone, South Ethiopia, from March 2023 to May 2023. A stratified random sampling technique was employed to allocate study participants into their catering establishment, and then a random sampling technique was applied to recruit participants. After getting signed consent, a structured questionnaire was used to collect data on socio-demographic and potential risk factors. Data was entered using EpiData version 3.1 and analyzed using the SPSS version 20 statistical package, and descriptive statistics were used to describe variables. Chi-square was used to identify factors associated with the outcome variable.
Result: The overall prevalence of bacterial positivity is 18/156 (11.5%), and among the identified bacterial isolates, 10/156 (6.4%) were Staphylococcus aurous, followed by Escherichia coli (5/156 (3.2%)), and 3/156 (1.9%) were Salmonella typhi. The isolated pathogens had associations with those who were not trained in food preparation and handling, those who had no clean nails observed, poor hand washing after sneezing, poor hand washing after touching waste, and those who had no habit of hand washing after latrine usage (defecation) (p < 0.001). The finding implies the need for strengthening the personal hygiene and redressal training of food handlers on personal hygiene guidelines to improve practice during food processing.
Keywords
Bacterial Hand Contamination, Food Handlers, Catering Establishments and Hossana
List of Abbreviations and Acronyms
ATCC -American Type Culture Collection
RPC- Research and Ethics publication Committee
SNNPR- Southern Nation Nationality Peoples’ Region
WHO- World Health Organization
Introduction
Background of the Study
Hands are the major source of contamination, which can never be totally free of microorganism especially bacteria. Food can become contaminated via dirty hands if there is lack of proper hygiene among the food handlers when handling food. Human hands are in regular contact with the surrounding environment and a variety of pathogens can reach the mucous membranes in the mouth, nose, eyes and genitals of human being through the hands and consequently contribute to food borne illness outbreaks. This research was designed to determine the level of bacterial hand contamination and associated factors among food handlers working in different catering establishments of Hossana Town. Total of 156 samples will be collected from the palm of food handlers of 83 Tea/Snack houses, 54 Cafeterias and Restaurants, and 19 Hotel in which each sample obtained will be cultured, bacteria isolated, identified and characterized according to standard procedure.
Statement of the Problem
Just like many other African countries, food borne illnesses are prevalent in Ethiopia and the loss of human life and suffering is enormous. Epidemiologic data related to food-borne diseases are inadequate in Ethiopia. But it can be evidenced that these are very common in the country because of many reasons including poverty, lack of awareness, poor water supply, poor personal hygiene and environmental sanitation, etc. According to the 2016-2017 “Health and Health related Indicators” published by the Planning and Programming Department of the Federal Ministry of Health of Ethiopia, Helminthic infections were the second leading cause of outpatient visits, Dysentery and different parasitic infections were also among the ten top causes of outpatient visits, Dysentery was among the leading causes of hospital admissions and deaths, Typhoid fever, acute diarrheal diseases, bloody diarrhea and anthrax were reported as some of the major causes of outbreaks [1].
It is known that food handlers are a common source of food borne diseases. The practice of good personal hygiene is essential for anyone who handles food, especially in food and drink establishments where many customers could potentially be affected. A sick food handler with symptoms of diarrhea, eye and ear discharges, skin infections, open cuts and wounds, or coughing should not continue working. They must be treated and be completely recovered before returning to work [2].
Despite the increasing number of food in catering establishments no study has been conducted on bacterial hand contamination and associated risk factors in Hossana Town, Haddiya Zone.
Significance of the Study
Since there is no research done in Hossana town before, this study expected to draw attention to identifications of bacterial hand contamination of food handlers in food establishments. The finding will help concerned body and the owner to give emphasis and to allocate resources to improve the overall repair and sanitary conditions of premises and empowering and equipping food handlers with safe food handling practice working with in the catering establishments.
Literature Review
Food related infections constitute an important public health problem in both developed and developing countries [3]. The problem is severe in developing countries due to difficulties in securing optimal hygienic food handling practices. In developing countries, up to an estimated 70% of cases of diarrheal disease are associated with the consumption of contaminated food [4]. The World Health Organization estimates 16 million new cases and 600,000 deaths of typhoid fever were each year worldwide [5]. Several studies have demonstrated that food handlers harbor S. typhi asymptomatically [6]. One of the historically notorious examples is that of the American cook “Typhoid Mary” (Mary Malon) who was responsible for 7 epidemics of typhoid fever affecting more than 200 persons [7].
Accordingly, food handlers with poor personal hygiene and inadequate knowledge working in food serving establishments could be potential sources of infections of many enteropathogenic bacteria and parasites [8]. Likewise, food handlers who harbor enteropathogenic bacteria may contaminate foods with their feces via their fingers, which in turn lead to food processing, and finally to infection of consumers [9]. Compared to other parts of the hand, the area beneath fingernails harbors many microorganisms and is difficult to clean [10]. More aggravated situations and challenges prevail in Ethiopia where food safety issues are not well understood and have received little attention.
Moreover, the cases of food-borne illnesses are rarely investigated in detail and under reported even if diagnosed in the form of outbreak or individual illness. In addition to these, research in the area of identifying the causative agent and food incriminated is also at its infant stage because of lack of well- developed laboratory system, consumables and reagents for isolation identification and lack of coordinated epidemiological surveillance systems. The aim of this study is therefore, to assess the prevalence of bacterial hand contaminations and associated factors among food handlers in Hossana Town.
Conceptual Framework
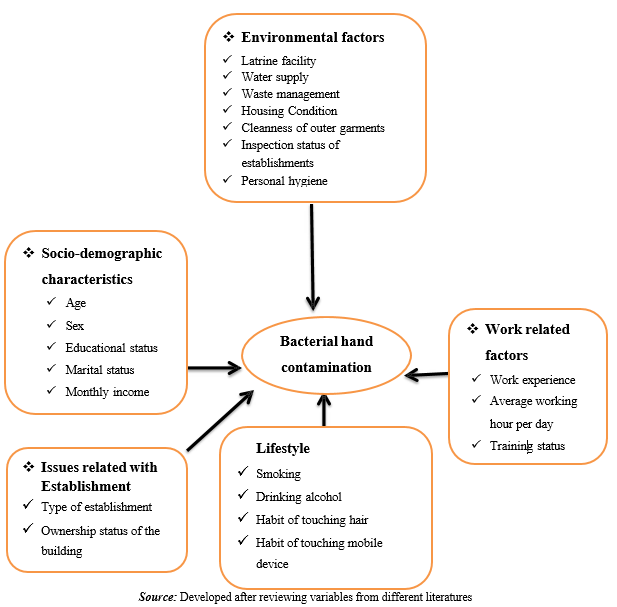
Figure 1: Conceptual Framework Adapted from Literature
Objectives
General Objective
The aim of this study was to assess bacterial hand contamination and its associated factors among food handlers in catering establishments of Hossana town, Haddiya zone, Southern Ethiopia, 2023.
Specific Objectives
1. To assess bacterial hand contamination of food handlers in catering establishments in Hossana town, Haddiya zone, southern Ethiopia
2. To identify factors associated with bacterial hand contamination of food handlers in catering establishments of Hossana town, Haddiya zone, Southern Ethiopia
Methods And Materials
Study Area and Period
The study conducted in Hossana town, South Ethiopia. It is located 232 km from Addis Ababa, capital of Ethiopia and 170 km from Hawassa, capital of SNNPR. The study will be conducted from March, 2023 to May, 2023.
Study Design
Community based cross sectional study design was applied.
Source Population and Study Population
All food handlers from a selected catering establishment in Hossana Town which has license will be study subjects, and all food handlers, who are engaged in food preparation, serving, and cleaning and reported to have never used any antimicrobial in the last 2 weeks and during the study period will be studied.
Study Participants
The study participants were purposively selected from the catering establishment one from Kitchen and one from waiters.
Inclusion and Exclusion Criteria
Inclusion Criteria
All study participant who are worked for at least for 6 months in the establishment and all food handlers who are reported to have never used any antimicrobial in the last 2 weeks and during the study period and working in food catering establishments such as hotels, cafeterias, restaurants, tea/snack house, fruit and juice house will be included in the study. Licensed food establishments included in order to find the actual information for this study and these establishments also expected to provide food service for large people.
Exclusion Criteria
Severely ill participants and those who were on medication excluded from this study. Food handlers in drinking service establishment and non-licensed Street food vendors or hawkers will be excluded. Food handlers working in drinking service establishment excluded because the risk of getting disease caused by bacterial contamination is high in food catering establishments than establishment that give only drinking service. In addition, Food handlers who have skin irritation, eczema, and inflammation will be excluded in the study, and all those people who are not willing to participate in the study will be excluded. Participants with a history of using antibiotic(s) 2 weeks prior to the study were excluded.
Sample Size Determination
The sample size will be calculated using a single population proportion formula
n: unadjusted sample size
z: z value obtained from standard normal distribution value (1.96 corresponding to 95% level of confidence)
p: pre study estimate proportion, 50% because there is no published study which indicates the prevalence in similar setting.
d: margin of error (0.05) Therefore,
Since the total number of the source population is less than 10,000, we used correction formula
Sampling Techniques
According to Hossana Town Trade and Investment bureau (2016) there were 121 tea house, 78 café and restaurants, and 27 hotel. To select representative participants, the final sample size proportionally allocated to each stratum, and food handlers selected using simple random sampling technique. As a result, one food handler selected randomly from each catering establishment. Accordingly, 83, 54 and 19 participants included from selected tea house, café and restaurant and hotels respectively for the study.
Sampling Procedures
From each strata the catering establishment was selected randomly and the data collectors prepared a frame based on the strata,
Data Collection Tools and Procedures
A pre-tested structured questionnaire was used to collect data relating to socio-demographic characteristics, and personal hygiene practices of food handlers, life style and behavioral, work related factors. The questionnaire developed from validated tools (14-16) and prepared in English and translated in to Amharic and observational checklist also used to get supplement data. Five sanitarians and four medical laboratory professionals was selected for data collection. Before starting any meal preparation activity including hand washing (if any), participant’s hands were sampled for microbial testing. Notification not given in advance, and extra hand hygiene not allowed during data collection.
Laboratory Data
Sample Collection and Transport and Inoculation
Sterile cotton swabs (Puritan Low-Lint Cylindrical Tip) were prepared and dipped into saline-containing sterile test tubes to collect samples from the fingernails and palm of the hand. Using these moistened cotton swabs, fingernail contents were collected from both hands of each subject by rubbing all over the surface under the nails. These samples were kept with normal saline in a test tube and transported to Hosanna College of health science laboratory by cold chain about 40C. The swab was simultaneously inoculated on MacConkey agar for the growth of gram negative bacteria and manitol Salt agar for staphylococcal bacteria. Then the remaining sample subjected for gram staining to get clue information about the gram reaction. All samples were cultured on same day of collection.
Bacterial identification
All of the samples were inoculated onto MacConkey agar (Oxoid, Hampshire, UK) and Manitol salt agar (Oxoid, Hampshire, UK) After 24 h of incubation at 37 0C, colony characteristics of the isolates and gram stain were performed then the species of the bacteria were identified following standard procedures using biochemical tests such as catalase, Coagulase, indole, motility, triple sugar iron agar, citrate, and urea.
Study Variables
Dependent Variable
Bacterial hand contamination.
Independent variables
Socio-Demographic Characteristics
• Age
• Sex
• Educational status
• Marital status
• Monthly Income
Issues Related with Establishment
• Type of establishment
• Ownership status of the building
Lifestyle and Behavioral Factors
• Smoking • Drinking alcohol
• Habit of touching hair and or nostrils
• Habit of touching mobile device
Work-Related Factors
• Work experience
• Average working hour per day
• Training status
Environmental Factors
• Latrine facility
• Water supply
• Waste management
• Housing Condition
• Cleanness of outer garments
• Inspection status of establishments
• Personal hygiene
Operational Definition of Selected Variables
Bacterial Hand Contamination: presence of one or more potential food borne bacterial hand contaminants
Food Borne Diseases - intoxication, infection, or illness contracted by the consumption of contaminated food
Food Handler - a person who is engaged in the process of food preparing, serving, and cleaning etc.
Potential Food Borne Bacterial contaminants – bacterial pathogens that can cause food contamination or spoilage
Personal Hygiene - refers to those protection measures primarily with the responsibility of the individual, which promote and limit the spread of infectious disease, like hand washing using soap and water, keep body clean etc.
Data Quality Management
To manage the quality of the work SOP strictly followed during processing of each sample. All the instruments used for sample processing checked for proper functioning as far quality control strains of S. aureus (ATCC 6538) was used. Data consistency and completeness will be made all the way during data collection, data entry and analysis. Culture Medias was prepared based on the manufactures instruction. The sterility of culture media was checked by incubating 3% of the batch at 35 – 37 oc overnight. Those Media which showed any growth was discarded.
Data Processing and Analysis
The data was entered into Epidata version 3.1 and analyzed by using SPSS version 20 (Copyright (c) SPSS Inc., 1997-2007, Polar Engineering and Consulting.) computer software. Data will be organized, summarized, and presented in simple descriptive Statistical methods. Chi-square test was used for checking any possible association between various categorical variables, and p-value<0.05 considered as significant.
Ethical Consideration
Ethical clearance obtained from Hossana College of Health Sciences Research and Ethics publication Committee (RPC) to conduct the study, and permission to conduct the was obtained from Hossana Town municipality council. Further Permission also obtained from the owners of the Catering establishments and written consent was obtained from each study participants. Confidentiality of the data maintained by making the data collectors aware not to record any identification information found on the card. For those who are carrier of permanent intrinsic pathogens appropriate referral linkage will be suggested
Dissemination Plan
The finding of the study will be disseminated to different stakeholders such as Hossana Town Trade and Investment bureau, Municipality, and other relevant offices.
Results
Characteristics of Study Participants
A total of 156 individuals participated in this study, with a response rate of 100%. Among them, 53.8% were female and 48.8% were aged between 20-24 years (mean age 22.92 + 4.67 years and median 22 years). The majorities (69.2%) of the participants were single and 65.4% were completed primary school, followed by secondary school (23.1%). More than half of participants 56.4% were included from Café and restaurants and 34% were from Tea and breakfast. The majority were 64.1% of the study participants were engaged in waiter and 34% were worked in food preparation in kitchen. The majority of food handlers (77.6%) had 1–2 years of work experience. Out of the total participants, 15.5% were certified for training in food handling and preparation and 62.7% had previously undergone a medical check- up including stool examination (Table 1)
|
Socio-demo variables |
Category |
Frequency (n=156) |
Valid Percent |
|
Marital status |
single |
108 |
69.2 |
|
Married |
48 |
30.8 |
|
|
Educational level |
Illiterate |
8 |
5.1 |
|
Primary (grade 1-6) |
102 |
65.4 |
|
|
Secondary (9-10) |
36 |
23.1 |
|
|
Diploma & above |
10 |
6.4 |
|
|
Preparing food |
Type of work |
53 |
34.0 |
|
waitering |
100 |
64.1 |
|
|
Washing |
3 |
1.9 |
|
|
Type of catering |
Hotel |
15 |
9.6 |
|
Café and Restourant |
88 |
56.4 |
|
|
Tea and break fast |
53 |
34.0 |
|
|
sex |
Male |
72 |
46.2 |
|
Female |
84 |
53.8 |
|
|
Age groups |
< 20 years |
64 |
41.0 |
|
20- 24 |
72 |
48.8 |
|
|
>25 |
17 |
10.2 |
|
|
Total |
156 |
100 |
|
Table 1: Socio-Demographic Characteristics of Study Participants
Prevalence of Isolated Bacteria from Hand Swabs of Food Handlers
The overall prevalence of bacterial positivity is 18/156 (11.5%) and among the identified bacterial isolates 10/156 (6.4%) were Staphylococcus aurous followed by Escherichia coli 5/156 (3.2%) and 3/156 (1.9%) were Salmonella typhi as shown in table 2.
|
Bacteria |
Number |
Percent |
|
E.coli |
5 |
3.2 |
|
S.aurous |
10 |
6.4 |
|
S.typhi |
3 |
1.9 |
|
No bacteria identified" |
138 |
88.5 |
|
Total |
156 |
100 |
Table 2: Prevalence of Isolated Bacteria Among Food Handlers in Catering Establishment
Among the all bacterial isolates positivity 11/72 (3.5%) were males and 14/108 (13.9%) were single. Among all positivity 7/64 (10.9%) were less than 20 years old and 15/102 (14.7%) were completed primary education as summarized in table 3.
Distribution of Isolated Bacteria Among Different Variables
With regard to hand-washing practices, 80.2% of food handlers reported that they had a habit of hand-washing after using the toilet. And also, most of the food handlers reported that they had a habit of hand-washing after touching different parts of their body (hair, nose, and ears) between handling food items table 4.
Pathogen prevalence and associated risk factors As shown in Table 4, 18 (11.5%) of the hand swab specimens tested positive for bacterial isolates. S.aourus (n = 10; 6.4%) had a higher frequency compared to E.coli (n = 5; 3.2%) and S.typhi (n= 3 (1.9%), while no pathogen was isolated from the swabs of 148 (88.5%) participants. Different factors were assessed for a possible association with pathogen infections among the study participants (Tables 2 and 4). The highest proportion of infection was seen among the age group of < 20 years no statistically significant as shown in Table 3.
All of the isolated pathogens were from those who were not trained in food preparation and handling. As illustrated in Table 4, the isolation rate of potential food-borne bacteria in swab samples was relatively higher among food handlers who had served for more than 8 hours (n = 15; 15.7%, P = 0.095) and higher among those who had no clean nail observed (n = 13; 35.5%) and statistically significant as shown table 4.
Regarding the habit of hand-washing after defecation, 80.2% had habit of hand washing after defecation. Among them 1.6% were positive and 98.4% were negative for pathogens. Among the respondents who had no habit of hand-washing after defecation (19.8% of the study population), 51.6% were positive and 48.4% were negative for pathogens. Therefore, the highest bacterial infection rate was observed in participants who had no habit of hand washing after latrine usage (defecation) and it is statistically significant (p < 0.001) (Table 4).
|
Variables |
Bacterial positivity |
P value |
|||
|
Negative |
Positive |
Total |
|||
|
Sex |
Male |
61 |
11(3.5%) |
72 |
0.176 |
|
Female |
77 |
7(3.4%) |
84 |
||
|
Marital status |
Single |
94 |
14(13.9%) |
108 |
0.404 |
|
Married |
44 |
4 (8.3%) |
48 |
||
|
Age group |
<20 Years |
57 |
7(10.9%) |
64 |
0.301 |
|
20-24 Years |
66 |
11(14.3%) |
77 |
||
|
>25 years |
14 |
0 (0%) |
14 |
||
|
Educational level |
Illiterate |
8 |
0(6.4%) |
8 |
0.294 |
|
Primary |
87 |
15(14.7%) |
102 |
||
|
Secondary |
33 |
3(8.3%) |
36 |
||
|
Diploma & above |
10 |
0 |
10 |
||
|
Type of catering |
Hotel |
15 |
0 |
15 |
0.336 |
|
Café and Restaurant |
77 |
11 (12.5%) |
88 |
||
|
Tea & breakfast |
46 |
7 (13.5%) |
53 |
||
|
Type of task |
Food preparation |
49 |
4 (7.5%) |
53 |
0.008 |
|
Waiter |
88 |
12 (12.0%) |
100 |
||
|
Washing dish |
1 |
2 (66.7%) |
3 |
||
|
Total |
|
148 |
18(11.5%) |
156 |
|
Table 3: The Distribution of Bacterial Positivity By Socio-Demographic Variables Using Chi-Square
|
Variables |
Category |
Bacterial positivity |
P value |
||
|
Negative |
Positive |
Total |
|||
|
Smoking |
Yes |
2 |
0 |
2 |
0.607 |
|
No |
136 |
18 |
154 |
||
|
Alcohol drinking |
Yes |
12 |
1(7.7%) |
13 |
0.650 |
|
No |
126 |
17 (11.9%) |
143 |
||
|
Respondent trend of touching hair or nose during food preparation |
Yes |
6 |
0 |
6 |
0.367 |
|
No |
132 |
18 (12%) |
150 |
||
|
Respondent trend of touching mobile phone during food preparation |
Yes |
33 |
3 (8.3%) |
36 |
|
|
No |
105 |
15 (12.5) |
120 |
||
|
Work load |
< 8hrs |
40 |
3 (7%) |
43 |
0.097 |
|
8-12hrs |
81 |
15(15.7%) |
96 |
||
|
>12hrs |
17 |
0 |
17 |
||
|
Training |
Yes |
27 |
1 (3.6%) |
28 |
0.145 |
|
No |
111 |
17 (13.3%) |
128 |
||
|
Awareness on food born disease |
Yes |
87 |
3 (3.3%) |
90 |
<0.001 |
|
No |
51 |
15 (22.7%) |
66 |
||
|
Hand washing after toilet |
Yes |
123 |
2 (1.6) |
125 |
<0.001 |
|
No |
15 |
16 (51.6%) |
31 |
||
|
Hand washing before starting food preparation |
Yes |
127 |
6 (4.5%) |
|
<0.001 |
|
|
No |
11 |
12 (52.2%) |
|
|
|
Hand washing after sneezing |
Yes |
124 |
6 (4.6%) |
130 |
<0.001 |
|
No |
14 |
12(46.2%) |
26 |
||
|
Hand washing after touching waste |
Yes |
129 |
5(3.7%) |
|
<0.001 |
|
No |
9 |
13(59.1%) |
|
||
|
touching food by your bare hand during waitery |
Yes |
69 |
4 (5.5%) |
73 |
0.026 |
|
No |
69 |
14 (16.9%) |
83 |
||
|
Hand washing area clean |
Yes |
114 |
4(3.8%) |
118 |
<0.001 |
|
No |
24 |
14 (36.8%) |
38 |
||
|
Clean nail |
Yes |
114 |
5 |
|
<0.001 |
|
No |
24 |
13(35.1%) |
|
||
|
Total |
|
148 |
18 |
156 |
Table 4: The Distribution of Bacterial Positivity by Different Variables Using Chi-Square
Discussion
Food handlers are an important vehicle for microorganisms, and improper handling practices may cause food contamination and consequently food-borne diseases, which pose a potential risk to public health [11]. Published information about food- borne pathogens among food handlers is scarce in Ethiopia. Therefore, this study was undertaken to assess the prevalence and associated factors of bacterial isolates among food handlers in catering establishments at Hossana town in the south Ethiopia. Hand swab cultures of 18 (11.5%) food handlers were positive for pathogenic bacterial species. This finding is similar to those of previous studies performed in Ethiopia from Arba Minch, Ethiopia which the reported isolation rate was 10% [12]. However, the result is higher than to those reported from Gondar 3.1%, and 3.5% in Addis Ababa and the finding was lower than studies from Abuja, Nigeria (62.6%) and Omdurman, Sudan (30.1%) [8,13,15]. The discrepancies may be due to differences in technique of pathogen isolation, the type of study participant, and the sample size. This rate of detection in the present study indicates that the hygiene conditions of the food handlers were challenged, due to the isolation of enteric pathogens like Salmonella and E.coli from the hand swab cultures. Good hygiene practices, both personal and in food handling, are the basis of preventing the transmission of pathogens from food handling personnel to consumers [13]. Hand swab cultures revealed the isolation of Salmonella typhi from 1.9%, E. coli 3.2% and S.aurous 6.4% of food handlers in the present study. This figure is comparable to that reported among food handlers at Gondar University cafeteria (2.7%) by Mulat, D. et al., (2013), at Gondar town by Andargie et al. (2008) (3.1%), and at Arba Minch University by Mohammedaman, M., & Getaneh, A. (2016), (3%) [8,13]. The present study demonstrated a higher rate of isolation compared to reports from Hawassa, Ethiopia (0.4%), Sudan (1.3%), and Jordan (1.4%) [15-17]. This may be due to differences in technique, the type of study participants, and the sample size.
Conclusion
• A total of 156 individuals participated in this study, with a response rate of 100%.
• The overall prevalence of bacterial positivity is 18/156 (11.5%) and among the identified bacterial isolates 10/156 (6.4%) were Staphylococcus aurous followed by Escherichia coli 5/156 (3.2%) and 3/156 (1.9%) were Salmonella typhi.
• The isolated pathogens had association from those who were not trained in food preparation and handling, those who had no clean nail observed (n = 13; 35.5%), Poor Hand washing after sneezing, Poor Hand washing after touching waste and who had no habit of hand washing after latrine usage (defecation) (p < 0.001)
Recommendations
• The Survey finding Imphy the need for strengthening the Personal Hygiene and refreshment training of Food handlers on Personal Hygiene guidelines to improve practice during food processing.
• Promote optimal hand washing at critical times and hand washing facilities located near the latrine
• Hosanna town health unit office should inspect and intervene the health and health related problems of food and drinks establishment
• Urban Health Extension Workers should increase their effort to create awareness on personal Hygiene during food preparation and handling through information, Education and communication food and drinks establishment workers.
• Promising effort must be started by the Municipality, Zonal health department, kebele administrative and Urban health extension workers by strengthening and organizing more effective and strengthening supervision, control and providing awareness creation activities to the community and food and drink establishment.
Acknowledgements
My special gratitude and heartfelt thank goes to Hossana Health Science College Research and Publication Core Process for facilitation of this research paper. I would like to thank my advisors Mr. Rebie Kedir and Mr. Andualem Girma for their unreserved help in the process of this paper. I would like also to thank Shemsedin Mohammed for his support during data collection. Finally I also thank all the respondents who were participated in this study, data collectors and Hosanna Municipal council.
References
- FMOH, Health and Health Related Indicators, Planning and Programming Department, 2016/2017
- World Health Organization. (1992). WHO Commission on Health and Environment: report of the Panel on Food and Agriculture (No. WHO/EHE/92.2). World Health Organization.
- Jacob, M., & World Health Organization. (1989). Safe food handling: a training guide for managers in food service establishments. World Health Organization.
- World Health Organization. (2000). Foodborne disease: a focus for health education. World Health Organization.
- World Health Organization. (2003). Manual for the laboratory identification and antimicrobial susceptibility testing of bacterial pathogens of public health importance in the developing world: Haemophilus influenzae, Neisseria meningitidis, Streptococcus pneumoniae, Neisseria gonorrhoea, Salmonella serotype Typhi, Shigella, and Vibrio cholerae (No. WHO/CDS/CSR/RMD/2003.6). World Health Organization.
- Senthilkumar, B., & Prabakaran, G. (2005). Multidrug resistant Salmonella typhi in asymptomatic typhoid carriers among food handlers in Namakkal district, Tamil Nadu. Indian Journal of Medical Microbiology, 23(2), 92-94.
- Parikh, U. N., & Murti, P. (1987). Salmonella carriers in foodhandlers in Bombay. Indian Journal of Public Health, 31(4), 217-220.
- Andargie, G., Kassu, A., Moges, F., Tiruneh, M., & Huruy,K. (2008). Prevalence of bacteria and intestinal parasites among food-handlers in Gondar town, northwest Ethiopia. Journal of health, population, and nutrition, 26(4), 451.
- Käferstein, F., & Abdussalam, M. (1999). Food safety in the 21st century. Bulletin of the World Health Organization, 77(4), 347.
- Lin, C. M., Wu, F. M., Kim, H. K., Doyle, M. P., Michaels,B. S., & Williams, L. K. (2003). A comparison of hand washing techniques to remove Escherichia coli and caliciviruses under natural or artificial fingernails. Journal of food protection, 66(12), 2296-2301.
- Tsegaye, A., Haymanot, T., Beyene, W., & Jemal, B.. Assessment of bacterial hand contamination and associated factors among food handlers working in the student cafeterias of Jimma University Main Campus, Jimma, South West Ethiopia. Journal of Community Medicine & Health Education, 2015, 5(4), 345.
- Aklilu, A., Kahase, D., Dessalegn, M., Tarekegn, N., Gebremichael, S., Zenebe, S., ... & Mama, M. (2015). Prevalence of intestinal parasites, salmonella and shigella among apparently health food handlers of Addis Ababa University student’s cafeteria, Addis Ababa, Ethiopia. BMC research notes, 8, 1-6.
- Mama, M., & Alemu, G. (2016). Prevalence, antimicrobial susceptibility patterns and associated risk factors of Shigella and Salmonella among food handlers in Arba Minch University, South Ethiopia. BMC infectious diseases, 16, 1-7.
- Ifeadike, C. O., Ironkwe, O. C., Adogu, P. O. U., Nnebue,C. C., Emelumadu, O. F., Nwabueze, S. A., & Ubajaka, C.F. (2012). Prevalence and pattern of bacteria and intestinal parasites among food handlers in the Federal Capital Territory of Nigeria. Nigerian Medical Journal, 53(3), 166- 171.
- Saeed, H. A., & Hamid, H. H. (2010). Bacteriological and parasitological assessment of food handlers in the Omdurman area of Sudan. Journal of Microbiology, Immunology and Infection, 43(1), 70-73.
- Dagnew, M., Tiruneh, M., Moges, F., & Gizachew, M. (2013). Bacterial profile and antimicrobial susceptibility pattern among food handlers at Gondar University Cafeteria, Northwest Ethiopia. J Infect Dis Ther, 1(105), 2332-0877.
- Desta, M., Asrat, D., Woldeamanuel, Y., & Nigusie, D. (2014). Prevalence of intestinal parasites and Salmonella and Shigella among food handlers at food service establishments in the main campus and Health Sciences College of Hawassa University, Hawassa, Ethiopia. The Ethiopian Journal of Health Development, 28(1), PDF- PDF.
- Araya Gebreyesus, A. G., Kelemework Adane, K. A., Letemichael Negash, L. N., TsehayeAsmelash, T.A., Shwaye Belay, S. B., Megbaru Alemu, M. A., & Muthupandian Saravanan, M. S. (2014). Prevalence of Salmonella typhi and intestinal parasites among food handlers in Mekelle University student cafeteria, Mekelle, Ethiopia.
- Bayeh Abera, B. A., Fantahun Biadegelgen, F. B., & Belaye Bezabih, B. B. (2010). Prevalence of Salmonella typhi and intestinal parasites among food handlers in Bahir Dar Town, Northwest Ethiopia.
- Fagernes, M., & Lingaas, E. (2011). Factors interfering with the microflora on hands: a regression analysis of samples from 465 healthcare workers. Journal of advanced nursing, 67(2), 297-307.
- Traub-Dargatz, J. L., Weese, J. S., Rousseau, J. D., Dunowska, M., Morley, P. S., & Dargatz, D. A. (2006). Pilot study to evaluate 3 hygiene protocols on the reduction of bacterial load on the hands of veterinary staff performing routine equine physical examinations. The Canadian Veterinary Journal, 47(7), 671.
- Voigt, J., Health surveillance and management procedures of food handling personnel. Report of a WHO Consultation. World Health Organization, 1990, 34, 474.
Annexes
Annex I.
Media Used to Isolate the Bacteria from Swabs
A. Mannitol Salt Agar
Composition per liter:
NaCl..................................................................75.0g
Agar..................................................................15.0g
D-Mannitol........................................................10.0g
Pancreatic digest of casein...............................5.0g
Peptic digest of animal tissue............................5.0g
Beef extract.......................................................1.0g
Phenol Red........................................................0.025g
PH 7.4 ± 0.2 at 25°C
Preparation of Medium: Add components to distilled/deionized water and bring volume to 1.0L. Mix thoroughly. Gently heat while stirring and bring to boiling. Distribute into tubes or flasks. Autoclave for 15 min at 15 psi pressure 121°C. Pour into sterile Petri dishes or leave in tubes.
Use: For the selective isolation, cultivation, and enumeration of staphylococci from clinical and nonclinical specimens. Mannitol-utilizing organisms turn the medium yellow.
B. Deoxycholate Citrate Agar
Composition per liter:
Sodium citrate...........................................50.0g
Agar 15......................................................0g
Lactose......................................................10.0g
Beef extract................................................5.0g
Peptone......................................................5.0g
Na2S2O3•5H2O.........................................5.0g
Sodium deoxycholate.................................2.5g
Ferric citrate................................................1.0g
Neutral Red.................................................0.025g
PH 7.3 ± 0.2 at 25°C
Preparation of Medium: Add components to distilled/deionized water and bring volume to 1.0L. Mix thoroughly. Gently heat and bring to boiling. Do not autoclave. Cool to 45°–50°C. Pour into sterile Petri dishes. Dry the agar surface before use. Use: For the selective isolation and cultivation of enteric pathogens, especially Salmonella and Shigella species.
C. Mac Conkey Agar
MacConkey Agar: Demonstrates the ability of a gram negative bacterium to metabolize Lactose. MacConkey agar is both a selective and differential medium frequently used in culture testing. It contains crystal violet dye and bile salts, both of which inhibit the growth of most gram-positive bacteria. It contains lactose (a sugar) and neutral red indicator (a pH indicator which is yellow in a neutral solution, but turns pink to red in an acidic environment), which allow for differentiation. On MacConkey agar, Escherichia coli and Enterobacter aerogenes would ferment the lactose producing acid and would form colonies pink to red in color. On the same medium, Salmonella, Shigella, and Pseudomonas species would not ferment the lactose and would form off-white colonies. The red colored colonies show that acid was produced from lactose, meaning the bacteria could utilize lactose as a carbon source.
Composition per liter:
Pancreatic digest of gelatin. 17.0g
Agar............................................................13.5g
Lactose.......................................................10.0g
NaCl............................................................5.0g
Bile salts......................................................1.5g
Pancreatic digest of casein.........................1.5g
Peptic digest of animal tissue......................1.5g
Neutral Red..................................................0.03g
Crystal Violet. 1.0mg
PH 7.1 ± 0.2 at 25°C
Preparation of Medium: Add components to distilled/deionized water and bring volume to 1.0L. Mix thoroughly. Gently heat while stirring until boiling. Autoclave for 15 min at 15 psi pressure 121°C. Pour into sterile Petri dishes or distribute into sterile tubes.
Use: For the selective isolation, cultivation, and differentiation of coli forms and enteric pathogens based on the ability to ferment lactose. Lactose-fermenting organisms appear as red to pink colonies. Lactose-non fermenting organisms appear as colorless or transparent colonies.