


Research Article - (2022) Volume 7, Issue 3
The Study of the Duration of Management of a Malnourished Child using Cow Milk
2Food Biotechnology department, Institut d’ Enseignement Superieur de Ruhengeri, P.O. Box 155 Ruhenge, Rwanda
3Department of Eastern Medicine, Government College University Faisalabad, Pakistan
4Department of Biochemistry, Damietta University, Egypt
5UNHCR Rwanda, Senior WASH assistant, Netherlands Institute for Housing and Urban Development Studies, P.O. Box 1935 3000 BX Rotterdam-, Netherlands
6Biomedical Laboratory Science department, Institut d’ Enseignement, Superieur de Ruhengeri, P.O. Box 155 Ruhengeri, Rwanda
7Monitoring and Evaluation, Learning Department, Quality Improvement Advisor, Intrahealth International/USAID Ingobyi Activity, Rwanda
Received Date: Jun 23, 2022 / Accepted Date: Jun 30, 2022 / Published Date: Jul 12, 2022
Copyright: ©Nizeyimana Fidele, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Nizeyimana Fidele, Dusabumuremyi Jean Claude, Muhammad Akram, Walaa Fikry Elbossaty, Singirankabo Vital, Yadufashije Callixte, Jean Marie Vianney Nkurikiyintwali (2022). The study of the duration of management of a malnourished child using cow milk. Adv Nutr Food Sci, 7(3), 237-244.
Abstract
The objective of the study was to determine the duration of managing a malnourished child using cow milk as supplement. The study was uncontrolled before and after study. The study was quantitative and was conducted in Musanze health center radiation zone. The study evaluated children who were in nutrition study follow up commissioned by UNICEF & Access To Health Project in 2016. This children research follow up was created under UNICEF & Access To Health Project fund for the study of their duration in management. Quantitative method was used. The non-probability sampling was used and a purposive technique was adopted. Data were collected on 57 malnourished children admitted in nutrition service at Musanze health center where 21 were in severe malnutrition while 36 were in moderate malnutrition. All malnourished children were given seven liters of caw milk per week per each child, during their follow up period. The Weight-for-Age and the Mid-Upper Arm Circumference were used to screen children. The study showed that when caw milk is used as the only supplement for the treatment of a malnourished child , the duration of taking a child from severe malnutrition to good nutrition took approximately double (7months) compared to World Health organization (WHO) nutrition care protocol (4months). Many children showed positive nutritional status evolutions but there was some who showed a negative evolution by staying in severe or moderate malnutrition. Family conflict and chronic illness are among the main causes of negative evolution in nutritional status. The other underlying cause is the situation of hunger in families having malnourished children. The supplement of cow milk is not enough as it takes longer period than the period expected by WHO. Therefore, balanced diet together with the supplement of cow milk, SOSOMA, RTUF can change nutrition status.
Keywords
Malnutrition, Severe Malnutrition, Moderate Malnutrition, Malnutrition Management
Introduction
In 2016, Rwanda wishes to move from the very expensive mal-nutrition care protocol which mainly composed with the supple-ment of SOSOMA and RTUF to the malnourished child, with milk which was abundant in the country. In this light, UNICEF & Access To Health Project called for proposal to do uncontrolled before and after study research to evaluate the duration of manage¬ment of a malnourished child using cow milk in a bid to find rec¬ommendations in changing the national malnutrition management care protocol.
Background
Severe acute malnutrition (SAM) is defined as the ratio between weight and height of less than 3, and a middle upper arm circum-ference is less than 115mm. Since 2000, the efforts of the World Health Organization (WHO) and UNICEF have made it possible to standardize the management of acute malnutrition, which has contributed to reducing infection rates and preventing complica-tions. Where the use of nutritional supplements and consumption of cow’s milk improved conditions.
Severe acute malnutrition and diarrhea are the leading causes of death in children. Diarrhea reduces the absorption of nutrients and fluids while severe acute malnutrition creates weak fluids and ho¬meostasis.
Malnutrition includes a broad spectrum of nutritional impairments, including intrauterine growth restriction, stunting, wasting, sub-optimal breastfeeding and deficiencies of micronutrients such as vitamin A and zinc (Black et al., 2013). In addition, malnutrition is associated with many factors in community and is highly observed in different people of different life styles. These include children under five years of age, pregnant women, and elderlies (WHO, WFP, UNSCN & UNICEF, 2007) or bad nourishment is observed when a person has inadequate intake of protein, energy and mi¬cronutrients, and frequent infections & diseases. It is in this re¬gard, the bad nutrition is more about quality than quantity of food (WHO, 2009) ; Institute of Medicine, 1995). Even if people get enough to eat, they will become malnourished if the food does not provide the proper amounts of micronutrients: vitamins and min-erals to meet daily nutritional requirements. This study focused on malnutrition status of children under five years. This form of mal¬nutrition is manifested when using anthropometric methods. One among others is mid up arm circumference (MUAC). The method indicates different malnutrition status as follow: severe, moderate, those who are at risk of malnutrition and adequately nourished as it has reported (Onis, Yip & Mei, 1997). There are several measures in place in both developed and developing worlds that are used to manage any form of malnutrition. Some of them include zinc sup¬plementation, vaccination against measles for the children, supple¬mentary food of maternal milk for the child of less than 24 months and supplementary food for a child less than 6 months when the mother die during delivery or in case of a complete lack of breast milk for the mother as approved by World Health Organization (WHO, 2015).
Scientific evidence points to a link between dairy products and growth in children, and many scientists and policy groups are now calling for the inclusion of dairy products in these foods specifical¬ly designed to treat child malnutrition.
For the former measure, WHO suggested the supplementation dos¬es of zinc based on ages: 10 mg/day during 10 days for children un¬der 6 months and 20 mg/day during 10-14 days for children greater than 6 months of age. However, the optimal dose of zinc for the children affected by malnutrition is still not clear defined as it was suggested by WHO recommends 2-4 mg/kg of zinc per day while the international consultative group recommends 10 mg per day (Izing, 2004; Lazzerini & Ronfani, 2012). A study conducted on strategies of supplementation of zinc is revealed that the stronger dose of 6 mg/kg/day in relation to 1.5 mg/kg/day was found to be associated with a high mortality with risk ratio of 4, 53 (Doherty et al., 1998). In addition, zinc can be also provided in therapeutic food as follow: food with F-75: 2, 0 zinc mg by 100 ml and F-100: 2, 3 mg zinc by 100 ml (WHO, 2007). This dose contained in ther¬apeutic food is in conformity with of WHO specification which al¬lows the ingestion of zinc 2-3 mg/kg/day. The supplementation of zinc can vary or be suggested based on other associated diseases to malnutrition. For instance, 20 mg/kg/day is given to children with diarrhea and for a child weighing six kilograms receiving 130 ml/ kg/day of F-75, is receiving a total of 15, 6 mg zinc per day (WHO, 2017) . Even though the bioavailability of zinc can be modified by concomitants through administration of other trace elements, it is not easy to manage zinc to the children living with acute mal¬nutrition. Furthermore, the zinc supplemented during the normal nutritional rehabilitation can lead to high dose that may negatively affect the child under consideration and therefore, it is not advised (Sommer, 2015).
A part from zinc supplementation, vaccination against measles for the children with severe malnutrition during the nutritional reha¬bilitation is next. This vaccine is provided in different ages of chil¬dren as it was highlighted by WHO (2005) where the vaccine is only given to children of 9-15 months when the child has not been already immunized and to those of greater than 15 months of age when child has been immunized in less than 15 months of age. In addition, when the vaccination is recommended, it should be made at the time of the admission in nutrition cares center with a second dose to the exit in order to save the gravity in period of incubation of the measles and to partially protect against the nosocomial mea¬sles, among others (Ministry of Health Republic of Kenya, 2009; Health E-FMo, 2007). For the children treated as outpatient, the initial dose can be omitted and only one vaccination must be man-aged after a nutritional rehabilitation of one month (WHO, 2013). Many studies were conducted on interaction between nutritional status and vaccine response to children and revealed the positive impact of vaccination against measles especially in severe mal¬nutrition (Wesley et al., 1979; Ekunwe, 1985; Greenwood et al., 1986; Kizito et al., 2013). Contrarily, some studies did not show the interaction between malnutrition and the immune response in the vaccination of measles especially to the children who were af¬fected by the kwashiorkor and marasmus of different degrees de¬fined by weight-for-age (Savy, Edmond & Fine, 2009).
In addition, the vaccination of measles is indicated as it was ob-served by the study conducted by (Kurubi. et al., 2009; Mahomva. Moyo & Mbengeranwa, 1997). For management of malnutrition using vaccination, WHO recommends two doses of measles vac¬cination to all children and the minimal length of time between the vaccinations could be 1 month (WHO, 2009). In this regard, at least one of the vaccinations must be managed after 9 months and its efficiency is from the intake time to onwards. Figure.1 shows the summarized WHO instructions for vaccination against mea¬sles.

Figure 1: Flow chart of vaccination against measles for children living with malnutrition in hospitalization or in management at Com-munity level (WHO, 2005)
The malnutrition in children under five years was found to be managed by supplementary food of maternal milk for the child of less than 24 months. This approach also is based on child age. For example for child of 6 months of age receives 2-3 spoons of por¬ridge 2-3 times per day, child of 6-9 months receives 2-3 spoons of simple meal 1/2 of the cup of porridge 2-3 times per day, child of 9-12months: 1/2 of the cup of porridge and a simple meal 3-4 times per day while one of 12-24 months receives 3/4 of the cup of porridge and a simple meal 3-4 times per day (WHO, 2005). The later approach is the food supplementation for a child less than 6 months when the mother dies during delivery or in case of a complete lack of breast milk for the mother. When a mother dies during delivery, a child is fed with an infant formula reserved for both children less than 6 months and those of their mothers completely lack breast milk. In order to feed those children under this approach, the formulas below are in place and used based on the quantity of milk required by a child per day. For a child of 0-7 days, Q= (ND-1)*10 gr. Where Q is the quantity of milk required by a child, ND is number of days of life. For a child of one week to 4 months, Q =(CW+ 200 gr)/10. Where CW in the child weight in gram. When the child is above 4 months, the ordinal cow milk can be given (WHO, 2005).
This study also indicates the treatment of malnourished children based on the ages. When a child is of 0 to 5 months and screened for malnutrition based on information related to properly nursing a child, loss of weight and sufficient maternal milk of mother for child and be classified in moderate or severe malnutrition, a moth¬er of the child is advised or recommended to nurse the child many times as required and to eat balanced diet by also focusing on food rich in vitamin A as it stimulates the milk production (WHO, 2007). In addition, depending on the severity of malnutrition, a child can be referred in pediatrics service at the hospital because the child cannot be treated at the health center level (Ministry of Health Republic of Rwanda, 2009). For the child of 6-59 months of age depending on malnutrition status such as moderate, severe, among others, nutrition intervention and medical intervention are needed to treat malnutrition. In Rwanda, the child under moderate malnutrition is provided SOSOMA or a combination of porridge flour (3,5kg/week), Caw milk (7litres/week) or therapeutic milk (F-75: 1st Phase, F-100 2nd Phase) while for medical interven-tions, vaccination against measles, Mebendazole, vitamin A are provide to a child. For Severe malnutrition (Child in Red color on the vaccination card), the child is nutritionally given Plumpy Nut as therapeutic food ready to consume(RUTF F-100) while medi-cally, a child is given vaccination against measles, Mebendazole, vitamin A, Amoxicillin and Folic Acid (WHO, 2009). Finally, a child with severe or moderate chronic malnutrition (Child late in growth: stunted) is therapeutically given SOSOMA or a combi-nation of porridge flour (3,5kg/week) while medically is given vaccination against measles (WHO Multicentre Growth Refer-ence Study Group, 2009). Moreover, for the children of less than 2 years the interventions mentioned above are combined with the recommendation given to the mother breastfeeding their children many times as much as possible and every moment the child wants to be breastfed. In addition, breastfeeding mother is obliged to pre¬pare the balanced diet for his child in order to prevent any type of malnutrition disease. Similarly to the children of 2-5 years of age, the child is only given balanced diet (Ministry of Health Republic of Rwanda, 2009).
Cow’s dairy products play an important role in treating malnu-trition, and this has led to the introduction of these products that contain a large amount of milk (F-100) to improve weight by in-creasing it and reducing the mortality rate. Cow’s milk contains protein known as PDCAAS, many peptides and other bioactive substances. Milk is an important source of minerals that support growth (type II nutrients), such as potassium, magnesium, phos-phorous and zinc, and the high lactose content also appears to sup-port growth due to the effect of prebiotics and improving mineral absorption.
Scientific evidence indicates that there is a relationship between the consumption of dairy products and the growth of children. Many researchers advocate the inclusion of dairy products in the foods of malnourished children. The nutritional composition of milk is very complex, as it contains almost all the nutrients that the body needs. Where one cup of full-fat cow’s milk provides 3.25% of fat and contains:
Calories: 149%
Water: 88%
Protein: 7.7 grams
Carbs: 11.7 grams
Sugar: 12.3 grams
Fiber: 0 grams
Fat: 8 grams
In addition, milk contains minerals and vitamins that the child needs during the growth process, including vitamin B12, calcium, phosphorus, vitamin B2, in addition to vitamin D.
Subjects and Methods
The study adopted an objective and positive philosophy. The study used survey strategy and quantitative method. The non-probabil-ity sampling method and a purposive technique were used to se-lect the study making up the target populations which comprised of 57 malnourished children. The study was uncontrolled before and after study. The study was uncontrolled because all the par¬ticipants were given milk supplement and followed for the period of 11 months to see if they improve. Data was collected on 57 malnourished children admitted in nutrition follow up which was created under UNICEF & Access To Health Project fund for the study of their duration in management at Musanze health center in January 2016.
Data collection procedure
All parent/guardian of malnourished children admitted in the stud¬ies signed a consent form to participate in the study by respecting the recommendation regarding malnutrition management taken from the health center. All enrolled children adhered the follow up regularly and were warned to not miss any follow up. All parent/ guardian were asked if a child met a problem of illness in the home care week to avoid bias from lacking primary health care. During the follow up, a child were screened using anthropometric meth¬ods mainly Weight-for-Age and the Mid-Upper Arm Circumfer¬ence (MUAC). When the screening put a child in a good nutrition status or a child move from one nutrition status to another, the duration of the transition were noted. Home visit to see if the par¬ent/guardian implement the acquired advice were regularly done. Every child was visited at home at least one times per two weeks.
Statistical analysis
All data were recorded using Ms. Excel and analyzed using de-scriptive statistics with frequencies by means of statistical soft-ware (SPSS).
Results Discussion
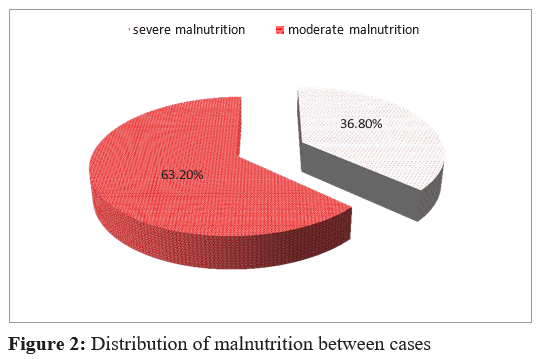
A total of 57 malnourished children were admitted in the study proposed by UNICEF & Access To Health Project at Musanze health center in January 2016. Of these, 21 (36.8%) in severe mal¬nutrition and 36 (63.2%) in moderate malnutrition, Figure.2.
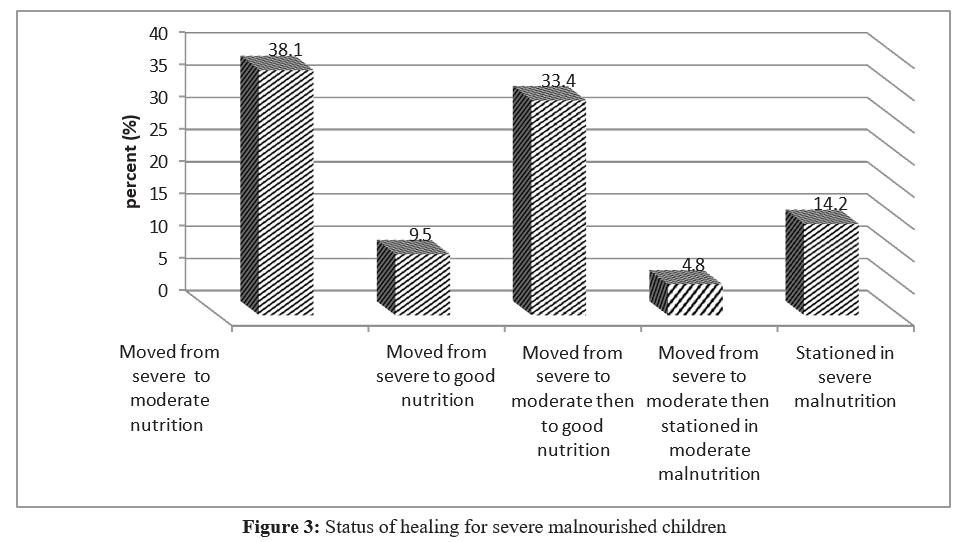
Severe cases followed up The results showed that 38.1% of followed children moved from severe to moderate nutrition. It is not ease to step from severe mal-nutrition directly to good nutrition (9.5%) when a child is regularly screened as indicated in the follow up table. Also it requires a long time to bring a child from severe malnutrition to good nutrition.
Among 21 severe cases followed up, only 17 healed whereas 3 remained in severe malnutrition during the intervention period of 11 months. Only 1 child stepped from severe malnutrition to mod¬erate malnutrition and stationed in moderate malnutrition. Most of them had chronic illness including mental disability, HIV and others lived in families with conflict of the husband and wife (Ta¬ble 1, Figure 3).
Table 1: Status of healing from severe malnourished children
|
Status of healing for severe malnourished children |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
|
|
Valid |
Moved from severe to moderate nutrition |
8 |
38.1 |
38.1 |
38.1 |
|
Moved from severe to good nutrition |
2 |
9.5 |
9.5 |
47.6 |
|
|
Moved from severe to moderate then to good nutrition |
7 |
33.4 |
33.4 |
81.0 |
|
|
Moved from severe to moderate then stationed in moderate malnutrition |
1 |
4.8 |
4.8 |
85.8 |
|
|
Stationed in severe malnutrition |
3 |
14.2 |
14.2 |
100.0 |
|
|
Total |
21 |
100.0 |
100.0 |
|
|
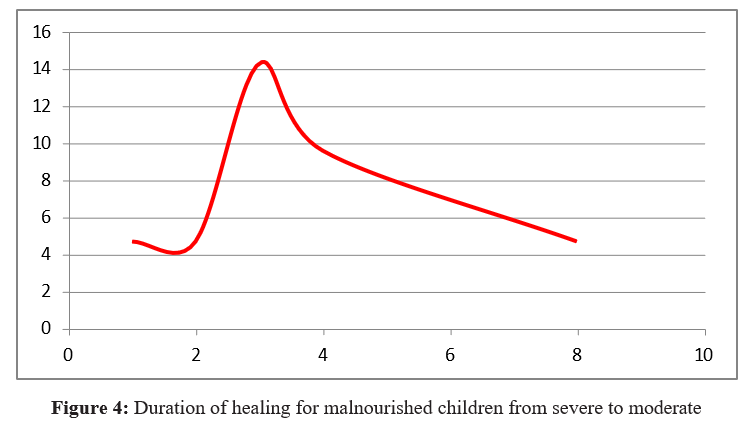
The study shows that generally a child could not exceed a period of 5 months in nutrition care center when he/she has not underlying serious causes. Most children followed up in moderate malnutri-tion healed within a period of 3 months. Only 30 children in 36 followed up healed and 6 remained malnourished. Of them 4 fallen from moderate malnutrition to severe malnutrition and returned in moderate malnutrition where they stationed. 2 children fallen from moderate malnutrition to severe malnutrition and stayed there. Most of those unhealed children had serious health problems (Ta-ble.2.A, Figure 4).
Table 2.A: Duration of healing for malnourished children
|
Duration of healing for malnourished children from severe to moderate malnutrition |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
|
|
Valid |
8 months |
1 |
4.7 |
12.5 |
12.5 |
|
|
4 months |
2 |
9.6 |
25 |
37.5 |
|
|
3 months |
3 |
14.3 |
37 |
75 |
|
|
2 months |
1 1 |
4.7 |
12.5 |
87.5 |
|
|
1 month |
8 |
4.7 |
12.5 |
100.5 |
|
|
Total |
999 |
38.0 |
100.0 |
|
|
|
Missing |
13 |
62.0 |
|
|
|
|
Total |
21 |
100.0 |
|
|
After 8 months malnourished children directly moved from severe malnutrition to good nutrition (Table.2.B).
Table.2.B: Duration of healing for malnourished children directly from severe malnutrition to good nutrition
|
Duration of healing for malnourished children directly from severe malnutrition to good nutrition |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
|
|
Valid |
8 months |
2 |
9.5 |
100.0 |
100.0 |
|
Missing |
999 |
19 |
90.5 |
|
|
|
Total |
|
21 |
100.0 |
|
|
Most children followed up in moderate malnutrition healed within a period of 8 months. 19% were seen in good nutrition after 8 months, while 9.6% took 5 months and after 4 months 4.8 % be-come well healthy (Table.3).
Table 3: Duration of healing for malnourished children from severe to moderate then to good nutrition
|
Duration of healing for malnourished children from severe to moderate malnutrition |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
|
|
Valid |
8 months |
4 |
19.0 |
57.1 |
57.1 |
|
|
5 months |
2 |
9.6 |
28.6 |
85.7 |
|
|
4 month |
1 |
4.8 |
14.3 |
100.0 |
|
|
Total |
7 |
33.4 |
100.0 |
87.5 |
|
Missing |
999 |
14 |
66.6 |
|
|
|
Total |
|
21 |
100.0 |
|
|
Moderate cases followed up
Among 36 moderate cases followed up, only 30 healed whereas 4 remained in moderate malnutrition during the intervention period of 11 months. Only 2 children stepped from moderate malnutrition to severe malnutrition (Table 4).
Table 4: Status of healing for moderate malnourished children to good nutrition
|
Status of healing for moderate malnourished children to good nutrition |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
|
|
Valid |
Recovered |
30 |
83.3 |
83.3 |
83.3 |
|
|
Complicated from moderate to severe and returned to stay in moderate malnutrition |
4 |
11.1 |
11.1 |
94.4 |
|
|
Complicated from moderate to severe and stayed in severe malnutrition |
2 |
5.6 |
5.6 |
100.0 |
|
|
Total |
36 |
100.0 |
100.0 |
|
Conclusion
Many children showed positive nutritional status evolutions but there was some who showed a negative evolution by staying in severe or moderate malnutrition. Family conflict and chronic ill-ness are among the main causes of negative evolution in nutrition¬al status.
The other underlying cause is the situation of hunger in families having malnourished children. It requires a period of 3 to 4 months to take a child from severe malnutrition to moderate malnutrition and a period of 2 to 3 months to take a child from moderate mal¬nutrition to good nutrition. By comparing the effort required, it requires much effort for a child in severe nutrition to move him/her to the other nutritional status. In general the management of a child using caw milk as supplementary food is not sufficient because it require an average of 7 months to take a child from severe malnu¬trition to good nutritional status which is beyond the predicted 4 months in WHO nutrition management protocol.
Basing on the study findings where it requires double time dura-tion for malnutrition healing in comparison with the time proposed by WHO, basing on the comparison of nutrition value labeled on the package of caw milk with nutrition values of RUTF, we rec-ommend the Ministry of Health to use caw milk together with RUTF for malnutrition management. As long the child remain in malnutrition the more the child is affected by the consequence of malnutrition.
There is consensus that children suffering from malnutrition should be provided with dairy products that contain large amounts of milk protein. In view of the high prices of these products, which are difficult to provide, especially in developing countries where the disease is spread, more studies are required to try to provide alternatives within the reach of everyone and have the ability to increase growth, in addition to weight gain.
Recommendations
Basing on the study findings, the researcher generated the follow-ing recommendations:
To the community:
• To adhere the community based nutrition program for malnu¬trition screening
• To prioritize feeding a balanced diet for under five years chil¬dren
• To adhere family planning services for spacing birth
• To adhere prenatal consultation when pregnant in order to avoid chronic illness that could be avoided
• To the nutrition care centers:
• To do home visit for all children in nutrition care in order to see the specific problem in each child family
• Multisectoral collaboration in order to succeed the problem of malnutrition
• To support families with different diet products than supple¬menting caw milk
• To reinforce nutrition education in community.
Acknowledgements
The present research work was undertaken by authors in collabo-ration with the authority of Musanze who facilitated the study; the authority provided an approval to conduct a study and guaranteed researchers any required assistance related to the study. This is gratefully acknowledged. The opinions and conclusions presented in this paper are those of the authors and do not necessarily reflect the views of the sponsoring organization
Funding Statement
The respondents were given a motivation payment in order to at-tract their mind on the focus of our study (i.e to avoid the lack of interest thinking that they are spending their time which could be used in money making). The motivational expenses for research participants and other study related expenses like transport of researchers and printing of questionnaires were contributed by UNICEF & Access To Health Project.
Ethical Statement
Before conducting this study, ethical clearance was requested to Musanze Health center and was approved (Signature & Stamp of the institution to the request letter) by the authority on 29th De¬cember 2015.
We, the researchers, have approved the final version to be pub-lished and we agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All persons who have made substantial contributions to the work reported in the manuscript, including those who provided editing and writing assistance but who are not authors, are named in the Acknowledgments section of the manuscript and have given their written permission to be named.
References
- Doherty, C. P., Sarkar, M. A., Shakur, M. S., Ling, S. C., Elton,R. A., & Cutting, W. A. (1998). Zinc and rehabilitation from severe protein-energy malnutrition: higher-dose regimens are associated with increased mortality. The American journal of clinical nutrition, 68(3), 742-748.
- FMOH, E. (2007). Protocol for the management of severeacute malnutrition. Federal Ministry of Health: Addis Ababa.
- Izing, G. (2004). Developing Zinc Intervention Programmes.
- Kurubi, J., Vince, J., Ripa, P., Tefuarani, N., Riddell, M., & Duke, T. (2009). Immune response to measles vaccine in 6 month old infants in Papua New Guinea. Tropical Medicine & International Health, 14(2), 167-173.
- Lazzerini, M., & Wanzira, H. (2016). Oral zinc for treating diarrhoea in children. Cochrane database of systematic reviews, (12).
- Mahomva, A. I., Moyo, I. M., & Mbengeranwa, L. O. (1997). Evaluation of a measles vaccine efficacy during a measles outbreak in Mbare, City of Harare Zimbabwe. The Central African journal of medicine, 43(9), 254-256.
- Ministry of Health Republic of Kenya. (2009). National Guideline for Integrated Management of Acute Malnutrition. Nairobi, Kenya.
- Ministry of Health Republic of Rwanda. (2009). National Guideline for Management of Acute and moderate malnutrition. Kigali, Rwanda: Available at http://www.moh.gov.rw.
- De Onis, M., Yip, R., & Mei, Z. (1997). The development of MUAC-for-age reference data recommended by a WHO Expert Committee. Bulletin of the World Health Organization, 75(1), 11.
- Savy, M., Edmond, K., Fine, P. E., Hall, A., Hennig, B. J., Moore, S. E., ... & Prentice, A. M. (2009). Landscape analysis of interactions between nutrition and vaccine responses in children. The Journal of nutrition, 139(11), 2154S-2218S.
- Sommer, A. (2015). Zinc deficiency and its consequences. A field guide to detection and control, 3rd ed. Geneva, Switzerland: World Health Organization.
- World Health Organization. (2005). Pocket book of hospital care for children: guidelines for the management of common illnesses with limited resources. World Health Organization.
- WHO. (2007). Vit A supplement: A guide to their use in the treatment and prevention of Vit A deficiency and xerophthal-mia, 2nd ed. Geneva, Switzerland: World Health Organization.
- World Health Organization. (2009). WHO child growth standards and the identification of severe acute malnutrition in infants and children: joint statement by the World Health Organization and the United Nations Children’s Fund.
- World Health Organization. (2009). WHO child growth standards and the identification of severe acute malnutrition in infants and children: joint statement by the World Health Organization and the United Nations Children’s Fund.
- WHO. (2009). Position on measles vaccines. Vaccine 27(52),7217-7219.
- Guideline, W. H. O. (2013). Updates on the management of severe acute malnutrition in infants and children. Geneva: World Health Organization, 2013, 6-54.
- WHO. (2015). Nutrition supplement and nutrient deficiency; assessment, prevention and control. Geneva 27, Switzerland: Unpublished document WHO/NUT/98.6: available on request from program of nutrition, World Health Organization,1211.
- World Health Organization. (2017). Guideline: assessing and managing children at primary health-care facilities to prevent overweight and obesity in the context of the double burden of malnutrition.
- World Health Organization, & World Health Organization. Nutrition for Health. (2009). WHO child growth standards: growth velocity based on weight, length and head circumference: methods and development. World Health Organization.
- World Health Organization. (2007). Community-based management of severe acute malnutrition: a joint statement by the World Health Organization, the World Food Programme, the United Nations System Standing Committee on Nutrition and the United Nations Children’s Fund.