

Research Article - (2022) Volume 6, Issue 1
The Status of Sharp Injury and Risk Factors among Health Care Staffs in the Bule Hora Hospital, South Ethiopia, 2020
Received Date: Mar 23, 2022 / Accepted Date: Apr 01, 2022 / Published Date: Apr 05, 2022
Copyright: ©Copyright: Ã??Ã?©2022 Shiferaw Gelchu Adola. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Shiferaw Gelchu Adola,(2022). The Status of Sharp Injury and Risk Factors among Health Care Staffs in the Bule Hora Hospital, South Ethiopia, 2020.Stem Cell Res Int 6(1):13-20.
Abstract
Background: Sharp injury is a penetrating cut wound from a needle or other sharp object which may additionally bring in contacting with blood or other body fluids of patients who may be having an infectious disease. Every year, more than half million of health care workers encounter needle stick injury that leads exposure to dangerous blood borne pathogens. This study was conducted to assess the magnitude of needle stick injury and contributing factors among health care staffs in the Bule Hora Hospital, south Ethiopia.
Methods: Facility based cross-sectional study was carried out from June20- July 30, 2020 among health care workers in the Bule Hora Hospital. The sample size for this study was 383. Descriptive statistics, bivariate and multivariable logistic regression were done. Statistical significance adjusted at P< 0.05.
Results: Nearly half of 166(45.4%) of the study subjects had experienced Sharp injury. The activities mainly causinginjuries were; waste collection (37.5%), giving injection (29.2%), and uncooperativeness of the patients (9.7%). Study participants that had not got training on prevention of occupational risks were two times more likely exposed to sharp injuries, AOR=1.67(1.47- 3.53). Health care workers working > 40 hours per week were nearly four times more likely exposed, AOR=3.74(1.68-8.28) to sharp injury.
Conclusion: Even though the magnitude of sharp injury was similar to the other studies, the prevalence in the study area was high. Lack of training and prolonged working hours were risk factors identified in this study for sharp injury, Therefore, health care workers should get training on prevention of workplace hazards and working hours must be regulated
Keywords
Sharp Injury, Health Care Staffs, Work Place Hazard, South Ethiopia
Background
Sharp injury is cut from a needle or other sharp item which may result encountering to the blood or other body liquids of someone else who may be have an irreversible microbes [1].According to International Labour Organization (ILO) report, every year 2.78 million laborers pass away from occupational related hazards or diseases in the working environment, of which 2.4 million are due to disease and an additional 374 million workers experience the ill effects of non-deadly occupational accidents[2].
There are 35 million medical services laborers that equals to around to 12% of the working people around the world. The health-related problems of this critical workforce have been ignored by both au- thoritatively and government body’s for longer period. In medical services industry, there is a serious misinterpretation exists that considered as this industry of care is free from diseases. However, in reality there are many infections occurs at health care facility [3].
Annually, around one million health care personnel encountered serious needle stick transmitting blood-borne microbes through tainted needles, sharp instruments or body fluid splashes. There were over 20 other different types of disease causing microbes that can be spread through needle stick related hazards like HBV, HCV, HIV, syphilis, malaria, and herpes [4,5].
These serious presentations among health workers can lead to blood-borne infections prevalently HBV, HCV, and HIV. In an un- vaccinated individual, the danger of transmission is the most noted worthy HBV disease is between 6% to 30%. The assessed danger of transmission of HCV is between 3% to 10%.Transmission of HIV following NSI is 0.3% and 0.1%. Nonetheless, if the source has a high viral load, the transmission rate increases more than ten times. Despite the fact that the transmission of HIV is not as HBV, that is 100 times less and 10 times less than HCV. It is related with significant mental and emotional disturbance, even social disgrace and may drastically influence the job satisfaction of health care personnel and leads to poor performance of work [5,6].
Methods
Study area
This study occurred in the Health care facilities of Bule Hora Hos- pital, which was located in, Oromia regional state, Southern Ethi- opia. Study design: A facility-based cross-sectional study design with a quantitative approach was implemented from June 20, to July 30, 2020 among health workers.
Study population
All health care workers who were found to have direct or indirect contact with patients and those who were practicing in this pro- fession for at least six months and above were incorporated in this study. Health care employees, those who were excluded from this study, were those on annual vacation, sick leave and pregnancy leave and have work experience less than six months.
Sample size determination and sampling procedure
The standard single population proportion formula was needed to decide the sample size in this study. Z (a/2)=1.96 (95% confidence level of the survey, 52.8 % prevalence from previous studies with similar study setting, and 5% margin of error was used in this study to bring sample size 383. HCWs were stratified based on their occupation and later by proportional allocation the required number of healthcare workers included in the sample from each stratum.
Data collection tools and techniques
The data was collected using structured and semi-structured self-administered questionnaires. The questionnaires were later divided into two parts: Part I: Socio-demographic Variables, Part II: Questionnaires related to the prevalence of needle stick injury.
The study subjects participated in the study voluntarily and they were able to stop participation whenever necessary. The tools were distributed and recollected from the participants after 24 hours. The pretested questionnaires and proper data collection procedure was done to ensure quality of the collected data. Pre-testing was done in Dilla referral Hospital among 10% (38) of the total study subjects.
Data management and analysis
First, the data was checked for completeness. Next, the cleaned data entered into Epi Data version 4.4.3.1. Finally, the data was exported to SPSS Statistics Version 25 for analysis. The results of this study were presented by tables, charts, and graphs. Percentage, frequency and mean were calculated using descriptive statistics. The associations between variables were checked using bivariate logistic regression. Variables that had as- sociation at P < 0.25 were taken to the multivariate logistic re- gression to control cofounding variables and check the strength of association. For multivariate logistic regression analysis, statically significance adjusted at p < 0.05 with 95% confidence interval.
Results
Socio-demographic Variables of Health Care Workers in the Bule Hora Hospital, 2020
The study was occurred among 383 health care workers with a response rate of 366 (95.56 %). Half of the 189(51.6%) study par- ticipants were males and 177(48.4%) were females. The median age of the study subjects was 26. About 209 (57.1%) were married in marital status and the highest number 152 (41.5%) were sanitary workers. In addition, 177 (48.4%) were diploma holders. Regard to the departments they were working 97 (26.6%), 69 (18.9%), and 69 (18.9%) of the health care workers were working in outpatient department, medical-surgical, and Ob-gyne wards respectively. The average service year of the respondent was 3.94+3.335 SD (See Table 1)
Table 1: Socio-Demographic Variables of the Study Participants (N=366)
|
Variables |
Variable Category |
Frequency(N) |
Percent (%) |
|
Sex |
Male |
189 |
51.6 |
|
Female |
177 |
48.4 |
|
|
Age |
≤25 |
159 |
43.44 |
|
25-34 |
193 |
52.73 |
|
|
>34 |
14 |
3.83 |
|
|
Marital status |
Single |
157 |
42.9 |
|
Married |
209 |
57.1 |
|
|
Profession |
Nursing |
120 |
32.8 |
|
Medical doctor |
34 |
9. |
|
|
Midwifery |
37 |
10.1 |
|
Lab. Technician |
23 |
6.3 |
|
|
Sanitary workers |
152 |
41.5 |
|
|
Education level |
Below Diploma |
55 |
15 |
|
Diploma |
177 |
48.4 |
|
|
Degree |
99 |
27 |
|
|
Master and above |
35 |
9.6 |
|
|
Work experience |
≤5 |
281 |
76.8 |
|
>5 |
85 |
23.2 |
|
|
Work in department |
Outpatient Department |
97 |
26.6 |
|
Emergency ward |
46 |
12.6 |
|
|
Operating theatre |
25 |
6.8 |
|
|
Medical-surgical ward |
69 |
18.9 |
|
|
Oby-Gyne ward |
69 |
18.9 |
|
|
Pediatrics ward |
18 |
5 |
|
|
Intensive care unit(ICU) |
32 |
8.7 |
|
|
Other |
9 |
2.5 |
Key: Other: pharmacy
Prevalence of sharp injury among health care workers in the Bule Hora Hospital, 2020
Majority of the study participants 313(85.5%) reported they gave attention to risk of the sharp injury while they were working and 308 (84.2%) rated the risk as high. Greater number of the HCWs 137(86.1%) agreed on the sharp injury was avoidable. The mag- nitude of the sharp injury in the Borana zone was 166(45.4%). The common activities which put HCWs at the risk of injuries were waste collection (37.5%), giving injection (29.2%), and uncooperativeness (9.7%) of the patients to the procedure per- formed to them (See Figure 1). Out of those exposed to sharp in- jury, 71(42.8%) of injuries happened in the past twelve months. All most all 334(91.3%) of the health care workers reported, there were an infection prevention committee in the zone. Regarding the use of PPE, 228(63.3%) of them always used PPE and 232(63.4%) reported insufficiency of PPE in the health care facility of the west guji zone. Concerning to the implementation of the standard pre- caution, 214(58.5%) of HCWs practice occasionally, and more than half 200(54.6%) not trained on infection prevention.
Two-thirds of HCWs were working more than forty hours per week and the average working time was 49.88 + 10.190 SD. The highest 140(84.3%) number of accidents occurred at night shift. Of whom were exposed to sharp injury, 97(58.4%) of them screened the sources of exposures; 193(52.7%) reported as sufficient PEP in the hospital and More than 2/3 (74.9%) of HCWs told as health facility provided PEP services for 24 hours. Out of who were ex- posed to hazard, 78(47%) took PEP. However, 54(14.8%) of them took the PEP within the first one hour (See Table 2)
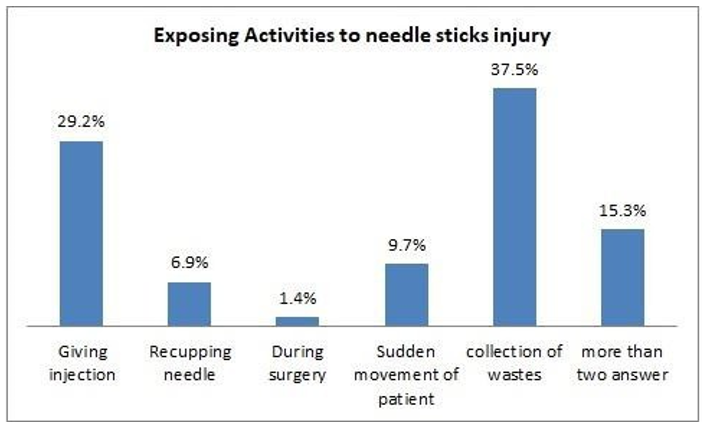
Table 2: Prevalence of Sharp injury among health care workers at Bule Hora Hospital, 2020 (N=366)
|
Variables |
Category |
Frequency |
Percent |
|
Do you concerned about risk of Needle Stick Injuries |
Yes |
313 |
85.5 |
|
No |
53 |
14.5 |
|
|
How do you rate the risk of Needle Stick Injuries |
Less risk |
58 |
15.8 |
|
High risk |
308 |
84.2 |
|
|
Is risk of Needle Stick injury avoidable |
Yes |
315 |
86.1 |
|
No |
51 |
13.9 |
|
|
Is there infection prevention committee in your health care institution |
Yes |
334 |
91.3 |
|
No |
32 |
8.7 |
|
|
Use of PPE |
Occasional |
138 |
37.7 |
|
Always |
228 |
63.3 |
|
|
Availability of Personal Protective Equipment’s in your institution |
Not Sufficient |
232 |
63.4 |
|
Sufficient |
134 |
36.6 |
|
|
Availability of safety guideline in your working ward. |
Yes |
311 |
85 |
|
No |
55 |
15 |
|
|
Ever exposed to NSI |
Yes |
166 |
45.4 |
|
No |
200 |
54.6 |
|
|
Exposed to Needle Stick Injuries in past 12 months |
Yes |
71 |
42.8 |
|
No |
95 |
57.2 |
|
|
Reporting Injuries to concerned body |
Yes |
53 |
31.9 |
|
No |
113 |
68.1 |
|
|
Exposure time to needle sticks injury |
Day |
26 |
15.7 |
|
Night |
140 |
84.3 |
|
|
Practice of standard precaution |
Sometimes |
214 |
58.5 |
|
Always |
152 |
41.5 |
|
|
Have you ever get training on Infection Prevention? |
Yes |
166 |
45.4 |
|
No |
200 |
54.6 |
|
|
Total working hour/week? ( in hours) |
≤40 |
106 |
29 |
|
>40 |
260 |
71 |
|
|
Post exposure screening of the source of exposure? |
Yes |
97 |
58.4 |
|
No |
69 |
41.6 |
|
|
Is there someone to administer PEP 24 hours a day in this facility |
Yes |
274 |
74.9 |
|
No |
92 |
25.1 |
|
|
Have you ever used Viral infection Post Exposure Prophylaxis? |
Yes |
78 |
47 |
|
No |
88 |
53 |
|
|
Time to start PEP after exposures |
Within 1hrs |
54 |
14.8 |
|
1-2hrs |
237 |
64.7 |
|
|
>2hrs |
75 |
20.5 |
Factors associated with sharp injury among health care workers in the Bule Hora Hospital, 2020
Factors associated with sharp injury were assessed using both bi- nary logistic and multivariable logistics regression model based on the developed conceptual framework. Variables which reach a P value of less than 0.25 were considered as having association with exposure of sharp injury at bivariate logistics regression.
Accordingly, the independent variable that had a statistically sig- nificant association with exposure to sharp injury was: Use of PPE, training, working time, report injury to responsible person and im- plement the standard precaution package.
The strength of association between the independent variables and exposure to sharp was done by using multivariable logistic regres- sion. The result showed HCWs who were not got training on infec- tion prevention were nearly two times more exposed AOR=1.67, with 95%CI (1.47-3.53) to sharp injury than trained health care workers. Working more than forty hours per week was significant- ly associated with sharp injury. Health care providers who work more than forty hours per week were nearly four times more ex- posed , AOR= 3.74, 95%CI (1.68-8.28) than those working less than forty hours per week. (See Table 3)
Table 3: Factors associated with Sharp injury among health care workers at Bule Hora Hospital, 2020
|
Predictors Variables |
Exposed to NSI |
COR(95%CI) |
P-Value |
AOR(95%CI |
P-Value |
|
|
No |
Yes |
|||||
|
Use of PPE |
|
|
|
|
|
|
|
Occasional |
64(32.2) |
74(44.4) |
1 |
0.05* |
1 |
0.95 |
|
Always |
136(67.8) |
92(55.6) |
0.59(0.31-.083) |
|
0.97(0.41-2.35) |
|
|
Training on IP |
|
|
|
|
|
|
|
Yes |
108(54) |
58(34.7) |
1 |
0.016* |
1 |
0.031** |
|
No |
92(46) |
108(65.3) |
2.18(1.16-4.20) |
|
1.67(1.47-3.53) |
|
|
Working Hours/week |
|
|
|
|
|
|
|
≤ 40 |
78(39.1) |
28(16.7) |
1 |
0.002* |
1 |
0.001** |
|
>40 |
122(60.9) |
138(83.3) |
3.15(1.50-6.82) |
|
3.74(1.68-8.28) |
|
|
Reporting injury |
|
|
|
|
|
|
|
No |
120(59.8) |
131(79.2) |
1 |
0.01* |
1 |
0.49 |
|
Yes |
81(40.2) |
34(20.8) |
0.38(0.19-0.79) |
|
0.69(0.24-1.96) |
|
|
Standard precaution Pr |
|
|
|
|
|
|
|
Occasional |
99(49.4) |
115(69.4) |
1 |
0.01* |
1 |
0.21 |
|
Always |
101(50.6) |
51(30.6) |
0.43(0.22-0.83) |
|
0.54(0.20-1.42) |
|
Key: COR- crude odds ratio, AOR- adjusted odds ratio, *Significant at P value < 0.25, **Significant at P value <0.05
Discussion
This study assessed the magnitude of sharp injury and risk factors among health care workersin the Bule Hora Hospital. The preva- lence of sharp injury was 166(45.4%). This finding is comparable with studies done in northern EthiopiaTigray region (38.5%), Ad- dis Ababa (39%) and Southeast Ethiopia Bale zone (37.1%) [7-9] and higher than studies conddacted in Malaysia (20.9%) and Saudi Arabia (13.84%)[10,11]. This result is lower than a systematic re- view and meta-analysis of 21 african countries (65.7%), Workers in Gondar Town 73.3%, and the study done in Serbia (56.5%) [12-14].The observed difference might be due to the difference in setting of the study, study population, study time gap, and aware- ness level of study participants regarding the implementation of the standard precaution packages.
In this study, one-year prevalence of sharp injury was 71(42.8%). This result is in agreement with a systematic review and meta-anal- ysis of 21 african countries (65.7%), Tanzania (48.6%) and the global systematic review and meta-analysis (44.5%)[12,15,16]. This higher than studyies done in northern EthiopiaTigray re- gion (38.5%), Addis Ababa (39%), Southeast Ethiopia Bale zone (37.1%) , and in Serbia[7-9,14].The difference might be explained by variation in study setting and study variables.
The common activities which put HCWs at the risk of injuries were waste collection (37.5%), giving injection (29.2%), and un- cooperativeness (9.7%) of the patients to the procedure performed to them. This result agreed with studies done in northern Ethio- piaTigray,un cooperativeness of patients (28.1%), waste collec- tion (18.1) and injection (14.6%), Southeast Ethiopia Bale zone, recping needle (46%), and waste collection (16.7%) and Kenya routen procedure 22% and waste collection (3.4%) [7,8,17]. This is might be due to the fact that the similarity of service provided in all health care setup.
According to this study, the higher number of injuries occurred during the night shift. This finding contradicts with studies done in northern EthiopiaTigray region and Kenya that the majority of an accident occurred at day time[1,17].In the present study, (31.9%) study participants not reported accidents to the concerned authority. This is comparable with the study conducted in Tanza- nia (32.1%) [15] and lower than sytematic review and meta-anal- ysis among healthcare workers in africa (48%) , and in Eastern Ethiopia Dire Dawa (65.3%) [16,18]. This is might be explained by difference regarding importance of reporting the injuries to the concerned authorities. In this study, 200(54.6%) of the study participants not get training on infection prevention. This result was supported by a study done in southern Ethiopia, Wilaita area, 58.9% [19]. This similarity may be explained by geographic loca- tion which was far from the training providing center. However,the result is lower than the study carried out in Southeast Ethiopia bale zone (65.3%) [9].
In this study, more than half of the health care workers (58.5%) not adhered to standard precoution during performing tasks.this find- ing agreed with the study conducted in in Addis Ababa (58.8%) and Northwest Ethiopia Awi zone (57.9%) [8,20].The similarity explained interms of non-adherance to standard precation is a com- mon problem across the country which needs awareness creation for all health care workers regarding the usefulness of consistent practice of standard precaution in preventing exposure of needle stick injury. The finding from this indicates 97(58.4%) of the study subjects screened sources of exposure. This is much lower than the study carried out in Tanzania (82.5%) and Kenya (91.5%) [15,17]. This considerable difference may be due to awareness regarding screening sources after exposure, fear of discrimination by col- leagues, and less concern to infection transmitted via needle stick injury.
Health care providers who were not got educational training on infection prevention were two times more likely exposed to sharp injury, AOR=1.67(1.47-3.53) than trained HCWs. This line with systematic review and meta-analysis of 21 african countries that HCWs without training were more exposed to sharp injury than trained one(AOR: 1.791, 95% CI: 1.234–2.071), Northern Ethi- opia Gondar town, no training AOR = 3.36, 95% (CI: 1.1, 11.2), study done in Tanzania AOR=3.10, 95% CI (2.58-626), Kenya protective training in infection prevention was[AOR= 0.52, 95% CI (0.03-0.90) [12,13,15,17]. This is due to the fact that lack of training increases the chances of exposure to sharp hazard.
This study shows HCWs works more than forty hours per week, nearly four times highly exposed, AOR= 3.74, 95%CI (1.68-8.28) sharp injury than those working less than forty hours per week. This finding supported with the study carried out in North Ethi- opia, Tigria region, AOR=16.09795%CI (6.252, 41.448) and a systematic review and meta-analysis of 21 african countries that health-care workers who worked less than forty hours per week were less likely exposed than those who worked more hours AOR: 2.221; 95% CI (1.001–4.926) [7,12]. This may be due to over work load from too much time working results fatigability which en- hances the risks of hazard.
The limitation of this study was from design it-self, cross-sectional study design was used in this survey that it was difficult to assume a causal relationship between variables. This study was conducted in a single zone, which is difficult to generalize the findings.
Conclusion
Nearly half of health care workers exposed to sharp injury. Even though the result is comparable with the similar studies, it is im- possible to say the low magnitude of hazard. More than half HCWs were not trained on infection prevention and not consistently prac- tice the standard precaution packages. Two-thirds of HCWs works more than forty hours per week and more than half of them report- ed as shortage of PPE in the institution.Use of PPE, reporting inju- ry to a responsible people, practice of standard precaution, training on infection prevention, and working hours per week were factors significantly associated with sharp injury. As a result, health care workers should get training on prevention of workplace hazards and working hours must be regulated.
What is already known on this topic?
• Sharp injury is a common problem among health care workers that face them at health care facilities.
• Even though different concerned bodies provide intervention to the problem; the magnitude of injuries still need greater concern.
What you add to this research ?
• This study identified the status sharp injury and contributing factors among health care staffs in the Bule Hora Hospital- which enables to give solution to the problem
• Lack of training and working for longer periods of times in the health care facilities were risk factors to sharp injury.
• Continuous training for health care workers regarding how to prevent the risk of sharp injury was a crucial intervention in the prevention of sharp injury in the health care facilities.
Lists of Abbreviations AIDS:
Acquired Immune Deficiency Syndrome; BBF: Blood and body fluid; CDC: Communicable disease control; HBV : Hepatitis B virus; HCV: Hepatitis C virus; HCW: Healthcare workers; HIV: Human immune deficiency virus; ILO: Internation- al Labour Organization; NSI: Needle stick injury; PPE: Personal protective equipment; PEP: Post exposure prophylaxis
Declaration
Ethics approval and consent to participate
Ethical clearance was obtained from Bule Hora University, Col- lege of Health and Medical Science, Institutional Review Board (IRB). Permission letter was given to managers of health care in- stitutions and informed consent was obtained from all respondents after explaining the objective of the study. The confidentiality of the collected data was assured and voluntary participation of study subjects was also maintained in this study.
Consent for publication
Not applicable
Availability of Data and materials
Author of this study declare that all data needed in this study can be available upon request by the side of corresponding author.
Competing Interests
Author of this study affirm that there was no compete of interests
Funding
Bule Hora University was funded for this study. The University has no role in designing and organizing, data collection, analysis, and report writing.
Authors' contributions
Shiferaw Gelchu Adola -Conceived and designed the study, ana- lyzed the data, and wrote the manuscript.
Acknowledgments
I acknowledge Bule Hora University for funding this study. I ex- tend our heartfelt thanks to all study participants, data collectors, and supervisors for their contribution to the success of our work.
References
- Rele, M., Mathur, M., & Turbadkar, D. (2002). Risk of needle stick injuries in health care workers-A report. Indian journal of medical microbiology, 20(4), 206-207.
- Tenkate, T., Adam, B., Al-Rifai, R. H., Chou, B. R., Gobba, F., Ivanov, I. D., ... & Modenese, A. (2019). WHO/ILO work-re- lated burden of disease and injury: Protocol for systematic re- views of occupational exposure to solar ultraviolet radiation and of the effect of occupational exposure to solar ultraviolet radiation on cataract. Environment international, 125, 542- 553.
- Wilburn, S. Q., & Eijkemans, G. (2004). Preventing needle- stick injuries among healthcare workers: a WHO-ICN collab- oration. International journal of occupational and environ- mental health, 10(4), 451-456.
- Wilburn, S. Q. (2004). Needlestick and sharps injury preven-tion. Online journal of issues in nursing, 9(3), 5.
- Hambridge, K. (2011). Needlestick and sharps injuries in the nursing student population. Nursing Standard, 25(27).
- Bhaskar, S. B. (2016). Manual of ICU procedures. Indian Journal of Anaesthesia, 60(11), 877.
- Weldesamuel, E., Gebreyesus, H., Beyene, B., Teweldemed- hin, M., Welegebriel, Z., & Tetemke, D. (2019). Assessment of needle stick and sharp injuries among health care workers in central zone of Tigray, northern Ethiopia. BMC research notes, 12(1), 1-6.
- Gebremariyam, B. S. (2019). Determinants of occupational exposure to blood and body fluids, healthcare workers’ risk perceptions and standard precautionary practices: A hospi- tal-based study in Addis Ababa, Ethiopia. Ethiopian Journal of Health Development, 33(1).
- Bekele, T., Gebremariam, A., Kaso, M., & Ahmed, K. (2015). Factors associated with occupational needle stick and sharps injuries among hospital healthcare workers in Bale Zone, Southeast Ethiopia. PloS one, 10(10), e0140382.
- Bhardwaj, A., Sivapathasundaram, N., Yusof, M. F., Minghat,A. H., Swe, K. M. M., & Sinha, N. K. (2014). The prevalence of accidental needle stick injury and their reporting among healthcare workers in orthopaedic wards in general hospital Melaka, Malaysia. Malaysian orthopaedic journal, 8(2), 6.
- Memish, Z. A., Assiri, A. M., Eldalatony, M. M., Hathout, H. M., Alzoman, H., & Undaya, M. (2013). Risk analysis of nee- dle stick and sharp object injuries among health care workers in a tertiary care hospital (Saudi Arabia). Journal of epidemi- ology and global health, 3(3), 123-129.
- Auta, A., Adewuyi, E. O., Tor-Anyiin, A., Aziz, D., Ogbole, E., Ogbonna, B. O., & Adeloye, D. (2017). Health-care work- ers’ occupational exposures to body fluids in 21 countries in Africa: systematic review and meta-analysis. Bulletin of the World Health Organization, 95(12), 831.
- Abere, G., Yenealem, D. G., & Wami, S. D. (2020). Occupa- tional Exposure to Blood and Body Fluids among Health Care Workers in Gondar Town, Northwest Ethiopia: A Result from Cross-Sectional Study. Journal of environmental and public health, 2020.
- Markovic-Denic, L., Maksimovic, N., Marusic, V., Vucicevic, J., Ostric, I., & Djuric, D. (2015). Occupational exposure to blood and body fluids among health-care workers in Serbia. Medical Principles and Practice, 24(1), 36-41.
- Chalya, P. L., Seni, J., Mushi, M. F., Mirambo, M. M., Jaka,H., Rambau, P. F., ... & Kalluvya, S. E. (2015). Needle-stick injuries and splash exposures among health-care workers at a tertiary care hospital in north-western Tanzania. Tanzania Journal of Health Research, 17(2).
- Bouya, S., Balouchi, A., Rafiemanesh, H., Amirshahi, M., Dastres, M., Moghadam, M. P., ... & Daley, K. A. (2020). Global prevalence and device related causes of needle stick injuries among health care workers: a systematic review and meta-analysis. Annals of global health, 86(1).
- Mbaisi, E. M., Wanzala, P., & Omolo, J. (2013). Prevalence and factors associated with percutaneous injuries and splash exposures among health-care workers in a provincial hospital, Kenya, 2010. Pan African Medical Journal, 14(1).
- Mekonnen, R., Yosef, H., Teklegiorgis, K., Tesfaye, F., & Dagne, I. (2018). Magnitude and impact of occupational re- lated needle stick and sharp injuries and associated factors among health care workers in Dire Dawa, Eastern Ethiopia. Med Saf Glob Health, 7(1), 2574-0407.
- Tadesse, M., Meskele, M., & Tadesse, A. B. (2016). Nee- dle-stick and sharps injuries among health care workers in Wolaita Zone, Southern Ethiopia. Med Saf Glob Health, 5, 2-7.
- Dilie, A., Amare, D., & Gualu, T. (2017). Occupational expo- sure to needle stick and sharp injuries and associated factors among health care workers in Awi Zone, Amhara Regional State, Northwest Ethiopia, 2016. Journal of environmental and public health, 2017.