
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2022) Volume 7, Issue 2
The Relationship between Pulmonary Artery Doppler and Non-Doppler Sonographic Parameters in the Fetal Lung Maturity According to Gestational Age
Received Date: Mar 25, 2022 / Accepted Date: Mar 29, 2022 / Published Date: Apr 04, 2022
Copyright: ©Sedigheh Salemkar, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Ensi Khalili Pouya, Elham Keshavarz, Sedigheh Salemkar, Moein Moradpour, Hamideh Zeidabadi, Elham Tavakkol. (2022). The Relationship between Pulmonary Artery Doppler and Non-Doppler Sonographic Parameters in the Fetal Lung Maturity According to Gestational Age. Int J Women's Health Care, 7(2), 67-72.
Abstract
Background: The evaluation of ultrasonic parameters of the lungs, especially the pulmonary arteries for gestational age, is still the first assessment of fetal lung maturity. We aimed to assess the relationship between pulmonary artery Doppler and non-Doppler sonographic parameters in the lung maturation of a fetus according to gestational age.
Methods: This cross-sectional study was performed on pregnant women at different gestational ages that were indicated for Doppler ultrasonography as an indication for assessing fetal lung maturity. The correlation between non-Doppler sonographic indices and fetal pulmonary artery Doppler indices was evaluated.
Results: Epiphyseal ossification centers, BPD, pulmonary echogenicity and free particles immersed in amniotic fluid were significantly higher in the group with a gestational age of 34 to 40 weeks than the group with a gestational age of 25 to 32 weeks. There was a significant difference in the mean of peak systolic velocity (PSV), ejection time (ET), acceleration time (AT) as well as acceleration time/ejection time (AT/ET) ratio between the two groups with a gestational age of 34 to 40 weeks and the group with a gestational age of 25 to 32 weeks. PSV, AT, ET, and AT/ET ration could predict fetal lung maturity with high sensitivity and specificity.
Conclusion: With increasing gestational age, an increase in PSV, increase in AT, decrease in ET, and increase in AT/ ET indices are expected. In this regard, PSA, AT, ET, and AT/ET values are able to predict neonatal lung maturity with acceptable sensitivity and specificity.
Keywords
Fetal Lung Maturity, Doppler Sonography, Fetus, Gestational Age
Introduction
Ultrasonic Doppler is at the forefront of all measures used to assess fetal lung maturity (FLM). In fact, Doppler effects make it possible to evaluate various parameters of fetal hemodynamic status [1]. In fact, based on the available evidence, the effects of ultrasonic Doppler have been a reliable way to predict FLM in the fetus [2]. The importance of Doppler is that it has always been considered a non-invasive method in assessing and estimating pulmonary artery pressure in infants as well as adults [3]. Doppler evaluation of the main pulmonary artery has been widely used in vascular system impedance analysis, and accordingly, pulmonary vascular Doppler evaluation seems to have a strong relationship with gestational age and FLM [4]. Fetal pulmonary artery Doppler volumetric may have major benefits in predicting FLM, which in fact is highly dependent on the sonographic echogenicity of fetal lung changes [5]. In fact, fetal pulmonary artery Doppler volumetric has also made it possible to assess the risk of fetal lung hypoplasia and the occurrence of RDS [6]. Recently, it has been shown that the pre¬dictability of fetal pulmonary artery indices has been much higher than biomechanical tests [7]. Accordingly, several formulas have been proposed to evaluate and estimate pulmonary artery pressure by determining the Doppler wave acceleration time (DWAT). In one of these formulas, a strong significant relationship was estab¬lished between DWAT and pulmonary artery pressure [8,9]. In this regard, both in infants and even adults, shortening of the acceler¬ation time/ejection time (AT/ET) ratio of pulmonary arteries has been suggested as a factor related to heart rate as well as increased pulmonary artery pressure [10-13].
Therefore, what many experts have agreed upon today is the value of Doppler of the main pulmonary artery of the fetus in predicting the onset and severity of RDS in late fetal and early infant lacta¬tion. In particular, the evaluation of this index in the two ranges of gestational age, late preterm (birth in weeks 34 to 36) and early term (birth in weeks between 37 to 38) has been very valuable [14,15]. Before the 34th week, the risk of fetal lung immaturity is very high and FLM evaluation is not very beneficial. Fetuses born after 39 weeks, on the other hand, have a very low risk of develop¬ing RDS [16,17]. It is possible to develop RDS between 34 and 38 weeks of pregnancy, but it is critical to assess FLM status before attempting to conceive a baby [18]. Today, various guidelines such as ACOG and SMFM are strongly recommended to use the FLM decision test for delivery [19,20]. Importantly, infants born at 36 to 38 weeks of gestation may be at high risk for RDS with hyperbili-rubinemia and hypoglycemia despite full neonatal lung maturation [21]. Therefore, in order to reduce the risk of developing RDS de¬spite fetal lung maturation, steroid therapy is still recommended (Guideline for Women and Pregnancy Canada) [22]. However, ac¬cording to European guidelines, the assessment and achievement of FLM is still a priority over steroid therapy [23]. Therefore, the evaluation of ultrasonic parameters of the lungs, especially the pulmonary arteries for gestational age, is still the first assessment of fetal FLM. In other words, pulmonary artery Doppler remains an important criterion in the evaluation of FLM. Some studies have shown that decreased impedance in the vascular bed of the fetal lungs in the third trimester will be an important predictor of neonatal RDS. In addition, infants with RDS will experience a de-crease in AT/ET ratio as well as an increase in pulsatility index (PI), vascular resistance index (RI), the systolic-diastolic pressure ratio of the pulmonary artery (S/D) ratio [24]. In assessing the risk of RDS, evaluation of the AT/ET ratio has also made it possible to assess the fetal pulmonary vascular resistance [24]. Therefore, it is not unreasonable to expect that pulmonary vascular Doppler char¬acteristics in the third trimester of pregnancy are closely related to non-vascular Doppler parameters such as RI and PI, and of course, this correlation will be directly related to gestational age. What we did in the present study was to investigate the relationship between pulmonary artery Doppler and non-Doppler sonographic factors in the lung maturation of a fetus according to gestational age.
Materials and Methods
This cross-sectional study was performed on pregnant women at different gestational ages that were indicated for Doppler ultraso-nography as an indication for assessing FLM. At the beginning of the study, background information including maternal age, parity, gestational age, maternal underlying diseases, and medi¬cations used were extracted. Mothers at risk for preterm delivery for various reasons were evaluated by ultrasonography before and after receiving the first dose of betamethasone. The most import¬ant non-Doppler parameters evaluated in these mothers were the presence of lower epiphyseal centers including the distal femoral epiphysis and proximal tibial epiphysis and the presence of free particles immersed in amniotic fluid, all of which indicate pulmo¬nary maturity in the fetus. In addition, the most important indica-tors of pulmonary artery Doppler in the fetus were PI, RI, S/D, AT, ET, and AT/ET ratio. Finally, both before and after betamethasone injection, the correlation between non-Doppler sonographic indi¬ces and fetal pulmonary artery Doppler indices was evaluated. In this regard, individuals were classified into two groups based on gestational age (25 to 32 weeks of gestation and between 34 to 40 weeks of gestation) and all correlations were evaluated in these two times.
For statistical analysis, results were presented as mean ± standard deviation (SD) for quantitative variables and were summarized by frequency (percentage) for categorical variables. Continuous vari¬ables were compared using a t-test or Mann-Whitney test when¬ever the data did not appear to have normal distribution or when the assumption of equal variances was violated across the study groups. P values of ≤ 0.05 were considered statistically significant. The correlation between the parameters was tested by Pearson or Spearman’s correlation test. The value of Doppler parameters in predicting FLM was assessed by the ROC curve analysis. For the statistical analysis, the statistical software SPSS version 23.0 for windows (IBM, Armonk, New York) was used.
Results
In the present study, individuals were classified into two groups based on gestational age, including pregnant women with a ges¬tational age of 25 to 32 weeks (20 cases) and pregnant women with a gestational age of 34 to 40 weeks (20 cases). Evaluations of non-Doppler ultrasonic indices in two groups are presented in Table 1. As can be seen, the mean of epiphyseal ossification cen¬ters in the group with a gestational age of 34 to 40 weeks was significantly higher than the group with a gestational age of 25 to 32 weeks (P = 0.009). Similarly, the mean BPD in the group with a gestational age of 34 to 40 weeks was significantly higher than the group with a gestational age of 25 to 32 weeks (P = 0.001). Also, the frequency of two parameters of pulmonary echogenicity and free particles immersed in amniotic fluid in the group with a ges¬tational age of 34 to 40 weeks was much higher than in the group with a gestational age of 25 to 32 weeks (P = 0.001).
Table 1: Non-Doppler sonographic parameters in the two groups
|
Parameter |
GA: 25 to 32 weeks |
GA: 34 to 40 weeks |
P value |
|
Mean of epiphyseal centers |
3.02±2.79 |
7.98±0.63 |
0.009 |
|
Mean BPD |
67.21±6.69 |
88.45±3.25 |
0.001 |
|
Mean lung echogenicity |
3 (15.0) |
18 (90.0) |
0.001 |
|
Free particles immersed in amniotic fluid |
3 (15.0) |
16 (80.0) |
0.001 |
Doppler sonographic indices of the pulmonary artery in two groups are presented in Table 2. As can be seen, there was a signif-icant difference in the mean of PSV, ET, AT as well as AT/ET ratio between the two groups with a gestational age of 34 to 40 weeks and the group with a gestational age of 25 to 32 weeks, but there was no significant difference in other indicators including RI and PI between the two groups.
Table 2: Doppler sonographic parameters in the two groups
|
Parameter |
GA: 25 to 32 weeks |
GA: 34 to 40 weeks |
P value |
|
Mean RI |
0.87±0.02 |
0.86±0.03 |
0.529 |
|
Mean PI |
2.17±0.43 |
2.16±0.23 |
0.820 |
|
Mean PSV |
57.11±15.11 |
71.21±14.65 |
0.006 |
|
Mean AT |
0.11±0.04 |
0.14±0.04 |
0.030 |
|
Mean ET |
0.22±0.06 |
0.17±0.03 |
0.005 |
|
Mean AT/ET ratio |
0.47±0.06 |
0.17±0.03 |
0.001 |
In the group with a gestational age of 25 to 32 weeks, in evaluat-ing the relationship between non-Doppler indices and ultrasonic parameters of the pulmonary artery, a significant direct correlation was observed between the RI index and pulmonary echogenicity. There was also a significant direct correlation between the PSV in-dex and BPD. However, AT, ET, or AT/ET ratios had no significant relationship with non-Doppler parameters (Table 3). However, in the group with a gestational age of 34 to 40 weeks, in evaluating the relationship between non-Doppler indices and pulmonary ar¬tery ultrasonic parameters, first, a direct correlation was obtained between RI index with two parameters of BPD and pulmonary echogenicity. There was a significant inverse correlation between AT and the number of bony epiphyseal centers. In addition, a sig¬nificant inverse correlation was obtained between AT/ET ratio and the number of bony epiphyseal centers as well as the number of particles immersed in amniotic fluid.
Table 3: The association of Doppler sonographic and non-Doppler parameters
|
Parameter |
RI |
PI |
PSA |
AT |
ET |
AT/ET |
|
Age: 25 to 32 weeks |
||||||
|
Mean of epiphyseal centers |
0.380 |
0.138 |
-0.216 |
-0.098 |
-0.214 |
-0.085 |
|
Mean BPD |
0.089 |
-0.207 |
0.463* |
0.320 |
0.043 |
0.331 |
|
Mean lung echogenicity |
0.489* |
0.192 |
0.382 |
0.337 |
-0.240 |
0.412 |
|
Free particles immersed in amniotic fluid |
-0.137 |
-0.073 |
-0.392 |
-0.168 |
-0.239 |
-0.151 |
|
Age: 34 to 40 weeks |
||||||
|
Mean of epiphyseal centers |
0.160 |
-0.219 |
0.201 |
-0.578* |
0.035 |
-0.564* |
|
Mean BPD |
0.467* |
0.270 |
0.279 |
-0.363 |
0.055 |
-0.399 |
|
Mean lung echogenicity |
0.459* |
0.198 |
0.366 |
0.183 |
-0.345 |
0.182 |
|
Free particles immersed in amniotic fluid |
0.128 |
0.159 |
0.114 |
-0.435 |
0.189 |
-0.497* |
|
* p < 0.05 |
||||||
Based on the analysis of the area under the ROC curve, the best cut-off point for PSV in predicting FLM was 55, which was able to predict neonatal lung maturity with a sensitivity of 84.2% and a specificity of 55%. The best cut-off value for AT index in pre-dicting lung maturity was 0.04, which was able to predict neonatal lung maturity with 84.2% sensitivity and 55% specificity. The best cut-off point for ET index in predicting lung maturity was 0.17, which was able to predict neonatal lung maturity with a sensitivity of 0.85% and a specificity of 60%. In addition, the best cut-off point for AT/ET index in predicting lung maturity was 0.28, yield¬ing a sensitivity of 89.7% and a specificity of 76% (Figure 1).
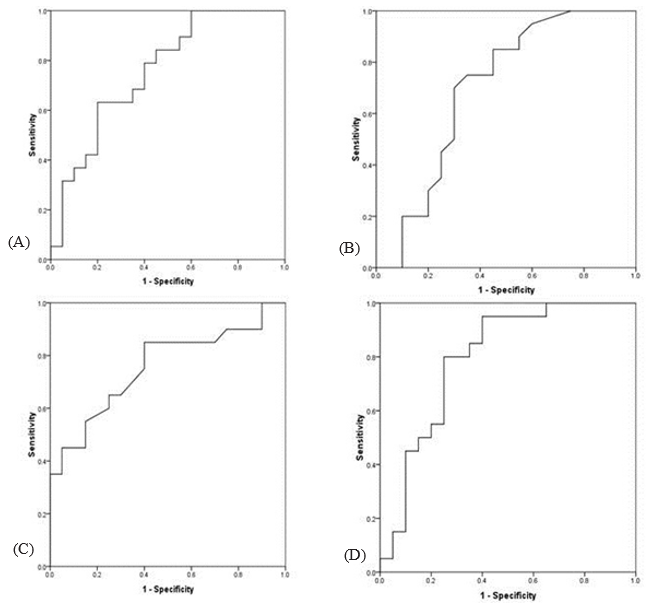
Figure 1: The ROC curve analysis to determine the value of Doppler parameters of PSV (A), AT (B), ET (C), and AT/ET (D) in predicting fetal lung maturity
Discussion
There are various criteria based on the structural characteristics of the fetus to predict the maturity of the fetal lung and in fact to predict the possible occurrence of respiratory distress in the in-fant. However, some of the tools used to assess such features were aggressive and some were not very sensitive or specific for as¬sessing fetal pulmonary maturity. Based on the available evidence, it seems that ultra-sonographic evaluation of fetal pulmonary ar¬teries (via Doppler ultrasound) can play a role in predicting fetal lung maturation with much higher accuracy and specificity. What was evaluated in the present study was the evaluation of the cor¬relation between non-Doppler ultrasonic parameters of the fetus and ultrasonic Doppler indices of the main pulmonary artery in the fetus. Given that gestational age is a confounding factor af¬fecting FLM, it is necessary to consider different gestational age groups in such an assessment. Therefore, in this study, two groups of fetuses with a gestational age of 25 to 32 weeks and 34 to 40 weeks were considered and statistical analyzes were considered in these two groups. First, in the present study, it was clearly shown that significant changes occurred in both categories of non-Dop-pler sonographic indices as well as fetal pulmonary artery Dop¬pler indices with increasing gestational age. Accordingly, with in¬creasing gestational age, the increase in mean epiphyseal centers, BPD, pulmonary echogenicity, and also immersed free particles as non-Doppler sonographic indices and, consequently, significant changes in arterial Doppler indices including AT, ET, and PSV was recorded with (although changes in RI and PI indices were not sta¬tistically significant). Therefore, in general, it can be said that the changes in terms of gestational age in non-Doppler and Doppler indices of the pulmonary artery occur parallel and simultaneously with each other.
In the second step, we evaluated the relationship between these two categories of non-Doppler and Doppler pulmonary artery in¬dices. This evaluation was performed separately in two subgroups including the group with gestational age under 34 weeks and over 34 weeks and was observed that first in the group between 25 to 32 weeks, the correlation between RI with echocardiography of lung tissue and also the correlation between PSA and BPD was ap-proved. . In other words, in this age group, despite the fact that we do not face complete immaturity of the fetal lungs, but there is also a significant relationship between arterial and non-arterial pulmo¬nary indices. Besides, at this age, fetal pulmonary artery Doppler indices did not show a significant correlation with non-pulmonary parameters such as the number of bone epiphyseal centers or the number of particles immersed in amniotic fluid. With increasing gestational age (in the group with a gestational age of 34 to 40 weeks) but the correlation between arterial Doppler indices and the above two non-pulmonary parameters also became statistical¬ly significant. First, the number of ossification epiphysis centers was predictable by both Doppler parameters AT and AT/ET. The RI index was also a predictor of echocardiography and BPD, and the number of free particles immersed in the high-amniotic fluid was predictable by the AT/ET ratio index. In conclusion, especial¬ly in the age group of 34 to 40 years, there is a strong correlation between non-Doppler parameters predicting pulmonary maturity or respiratory distress with pulmonary artery Doppler parameters.
The results of our study are consistent with some previous studies, but in general, the evaluation of fetal pulmonary artery Doppler indices in predicting fetal pulmonary immaturity or predicting the occurrence of RDS has been used. However, in some indices, there was no significant relationship between the occurrence of RDS and arterial Doppler indices. In the study of Moiety et al, PSV, RI, PI, and AT/ET ratio indices had a significant positive relationship with gestational age, which in our study was unique to PSV and AT/ET ratio. In addition, there was a significant difference between PI and RI, AT/ET ratio, and PSV indices between infants with and with¬out RDS [25]. In the study of Mohamed et al, the occurrence of RDS was closely and significantly related to each of the RI, PI, and AT/ET ratios [26]. In the study of Nasr Mohamed et al, there was a significant relationship between the occurrence of RDS and AT/ET ratio, but there was no relationship between the occurrence of RDS with two parameters PI and RI [27]. In the study of Mehrjardi et al. and quite similar to our study, RI and PI did not show a significant difference between the two groups of neonates with and without respiratory distress admitted to the NICU. However, the AT/ET ratio in infants with RDS was different from other infants [28].
Finally, although in the present study we did not evaluate the AT/ ET cut-off point for predicting RDS in neonates, this index with a cut-off point of 0.3 (in all studies) was able to predict the occur-rence of RDS with high sensitivity and specificity. Finally, it can be acknowledged that the Doppler characteristics of the pulmo-nary artery will be reliable indices for predicting fetal pulmonary maturity. Of course, it is recommended that the cut-off point of this index and other Doppler indices in predicting RDS in our society be considered and evaluated.
Conclusion
In a conclusion, firstly, with increasing gestational age, we will see an increase in PSV increase in AT, a decrease in ET, and an increase in AT/ET indices. In this regard, PSA values above 55, AT above 0.04, ET below 0.17, and AT/ET values above 0.28 will be able to predict neonatal lung maturity with acceptable sensitivity and specificity. Therefore, evaluation of pulmonary artery indices along with non-Doppler indices can be used to predict fetal pul¬monary maturity and therefore predict the occurrence of RDS in the infant.
References
- Schenone MH, Samson JE, Jenkins L, Suhag A, Mari G. (2014). Predicting FL Musing the fetal pulmonary artery Doppler wave acceleration/ejection time ratio. Fetal Diagn Ther, 36: 208-214.
- Howard, L. S., Grapsa, J., Dawson, D., Bellamy, M., Chambers, J. B., Masani, N. D., & Gibbs, J. S. R. (2012). Echocardiographic assessment of pulmonary hypertension: standard operating procedure. European Respiratory Review, 21(125), 239-248.
- Fakhri, A. A., Hughes-Doichev, R. A., Biederman, R. W., & Murali, S. (2012). Imaging in the evaluation of pulmonary artery hemodynamics and right ventricular structure and function. Heart Failure Clinics, 8(3), 353-372.
- Guan, Y., Li, S., Luo, G., Wang, C., Norwitz, E. R., Fu, Q., & Zhu, J. (2015). The role of doppler waveforms in the fetal main pulmonary artery in the prediction of neonatal respiratory distress syndrome. Journal of Clinical Ultrasound, 43(6), 375-383.
- Moety, G. A. F. A., Gaafar, H. M., & El Rifai, N. M. (2015). Can fetal pulmonary artery Doppler indices predict neonatal respiratory distress syndrome?. Journal of Perinatology, 35(12), 1015-1019.
- Kim, S. M., Park, J. S., Norwitz, E. R., Hwang, E. J., Kang,H. S., Park, C. W., & Jun, J. K. (2013). Acceleration time-to-ejection time ratio in fetal pulmonary artery predicts the development of neonatal respiratory distress syndrome: a prospective cohort study. American journal of perinatology, 30(10), 805-812.
- Granstam, S. O., Björklund, E., Wikström, G., & Roos, M.W. (2013). Use of echocardiographic pulmonary acceleration time and estimated vascular resistance for the evaluation of possible pulmonary hypertension. Cardiovascular ultrasound, 11(1), 1-7.
- Dabestani, A., Mahan, G., Gardin, J. M., Takenaka, K., Burn, C., Allfie, A., & Henry, W. L. (1987). Evaluation of pulmonary artery pressure and resistance by pulsed Doppler echocardiography. The American journal of cardiology, 59(6), 662-668.
- Koestenberger, M., Apitz, C., Abdul-Khaliq, H., & Hansmann,G. (2016). Transthoracic echocardiography for the evaluation of children and adolescents with suspected or confirmed pulmonary hypertension. Expert consensus statement on the diagnosis and treatment of paediatric pulmonary hypertension. The European Paediatric Pulmonary Vascular Disease Net-work, endorsed by ISHLT and DGPK. Heart, 102(Suppl 2), ii14-ii22.
- Mitchell, J. M., Roberts, A. B., & Lee, A. (1998). Doppler waveforms from the pulmonary arterial system in normal fetuses and those with pulmonary hypoplasia. Ultrasound in Obstetrics and Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 11(3), 167-172.
- Chaoui, R., Taddei, F., Rizzo, G., Bast, C., Lenz, F., & Boll-mann, R. (1998). Doppler echocardiography of the main stems of the pulmonary arteries in the normal human fetus. Ultrasound in Obstetrics and Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 11(3), 173-179.
- Azpurua, H., Norwitz, E. R., Campbell, K. H., Funai, E. F.,Pettker, C. M., Kleine, M., ... & Thung, S. F. (2010). Acceleration/ejection time ratio in the fetal pulmonary artery predicts fetal lung maturity. American journal of obstetrics and gynecology, 203(1), 40-e1.
- Declaration of Helsinki (1964). BMJ 1996. 313, 1448-1449.
- ACOG committee opinion no. 764 (2019): medically indicated late-preterm and earlyterm deliveries, Obstet. Gynecol. 133 (2) e151-e155.
- Hourani, M., Ziade, F., & Rajab, M. (2011). Timing of planned caesarean section and the morbidities of the newborn. North American Journal of medical sciences, 3(10), 465.
- Gawlik, S., Müller, M., Kuon, R. J., Szabo, A. Z., Keller, D., & Sohn, C. (2015). Timing of elective repeat caesarean does matter: importance of avoiding early-term delivery especially in diabetic patients. Journal of Obstetrics and Gynaecology, 35(5), 455-460.
- Tita, A. T., Jablonski, K. A., Bailit, J. L., Grobman, W. A.,Wapner, R. J., Reddy, U. M., ... & VanDorsten, J. P. (2018). Neonatal outcomes of elective early-term births after demonstrated fetal lung maturity. American journal of obstetrics and gynecology, 219(3), 296-e1.
- ACOG committee opinion no. 560 (2013): medically indicated late preterm and early-term deliveries, Obstet. Gynecol. 121(4), 908-910.
- Committee opinion no. 688 (2017): management of subopti-mally dated pregnancies, Obstet. Gynecol. 129(3), e29-e32.
- Bates, E., Rouse, D. J., Mann, M. L., Chapman, V., Carlo, W. A., & Tita, A. T. (2010). Neonatal outcomes after demonstrated fetal lung maturity prior to 39 weeks of gestation. Obstetrics and gynecology, 116(6), 1288.
- Boutin, A., Skoll, A., Bujold, E., Burrows, J., Crane, J., Geary, M., & Joseph, K. S. (2018). Antenatal corticosteroid therapy for improving neonatal outcomes: balancing benefits and risks. Journal of obstetrics and gynaecology Canada: JOG-C=Journal d’obstetrique et gynecologie du Canada: JOGC, 40(9), 1193-1197.
- D.G. Sweet, V. Carnielli, G. Greisen, M. Hallman, E. Ozek,A. Te Pas, R. Plavka, C.C. Roehr, O.D. Saugstad, U. Simeoni,C.P. Speer, M. Vento, G.H.A. Visser, H.L. Halliday, (2019). European consensus guidelines on the management of RCD -2019 update, Neonatology 115(4), 432–451.
- Suhag AH, Channar MI and Lakho AR (2016): Fetal biometry in the third trimester. www.meforum.pk/ index.database9-ar-ticles/ 79.
- Kitabatake, A., Inoue, M., Asao, M., Masuyama, T., Tanouchi, J., Morita, T., & Abe, H. (1983). Noninvasive evaluation of pulmonary hypertension by a pulsed Doppler technique. Circulation, 68(2), 302-309.
- Moety, G. A. F. A., Gaafar, H. M., & El Rifai, N. M. (2015). Can fetal pulmonary artery Doppler indices predict neonatal respiratory distress syndrome?. Journal of Perinatology, 35(12), 1015-1019.
- Mohamed A., Abo Elwan Y., El Shabrawy A., ELsayed H. (2020). Prenatal Prediction of Fetal Lung Maturity by Measuring Fetal Pulmonary Artery Doppler Indices. European Journal of Molecular & Clinical Medicine 7(11): 1334-1349.
- Nasr Mohamed M. Osman. Can ultrasound techniques predict neonatal respiratory distress 28? ECR 2020. Available in https://ecrtoday.myesr.org/
- Zare Mehrjardi, M. (2019, September). Fetal Pulmonary Artery Doppler Examination as a Non-Invasive Test for Assessing Prenatal Lung Maturity. In Iranian Congress of Radiology (Vol. 35, No. 4, pp. 89-89). Iranian Society of Radiology.