

Research Article - (2026) Volume 9, Issue 1
The Impact of Nurse Emotional Intelligence as a Measurable Outcome Variable in Results-Oriented Care
Received Date: Jan 05, 2026 / Accepted Date: Jan 26, 2026 / Published Date: Feb 12, 2026
Copyright: ©2026 Thizwilondi Ananias Magadze. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Magadze, T. A. (2026). The Impact of Nurse Emotional Intelligence as a Measurable Outcome Variable in Results-Oriented Care. Adv Neur Neur Sci 9(1), 01-08.
Abstract
Background: Modern healthcare systems increasingly adopt results-oriented care models that prioritise measurable performance indicators. However, traditional nursing performance metrics largely overlook emotional and relational competencies despite their significant influence on patient outcomes.
Aim: This study examined the impact of nurse emotional intelligence (EI) as a measurable outcome variable within results- oriented care and explored its influence on patient satisfaction, communication quality, and emotional support.
Methods: A mixed-methods descriptive cross-sectional design was employed in medical, surgical, and emergency units of a tertiary hospital. One hundred and twenty registered nurses completed the Wong and Law Emotional Intelligence Scale (WLEIS), and 150 adult inpatients completed a patient satisfaction and communication questionnaire. Semi-structured interviews were conducted with 20 patients. Quantitative data were analysed using SPSS (descriptive statistics, Pearson correlation, and linear regression); qualitative data underwent thematic analysis.
Results: Nurses demonstrated high overall EI (M = 4.03, SD = 0.64), with strongest performance in others’ emotion appraisal (empathy). Nurse EI showed strong positive correlations with communication clarity (r = 0.68, p < 0.001), emotional support (r = 0.71, p < 0.001), and overall patient satisfaction (r = 0.75, p < 0.001). Regression analysis revealed that EI explained 56% of the variance in patient satisfaction (R2 = 0.56, p < 0.001). Qualitative themes highlighted emotional presence, human-centred communication, and perceived competence as key patient-valued outcomes linked to high nurse EI.
Conclusion: Emotional intelligence is a measurable, powerful predictor of patient-centred outcomes and should be formally integrated into results-oriented nursing performance frameworks, staff development, and quality metrics.
Keywords
Emotional Intelligence, Nurse, Results-Oriented Care, Patient Satisfaction, Communication, Empathy, Performance Indicators, Mixed-Methods, Donabedian Model, Goleman
Introduction
Modern healthcare systems have undergone significant transformation as global demands for accountability, efficiency, and measurable outcomes have intensified. The shift toward results oriented care seeks to improve healthcare quality by focusing on measurable performance indicators such as patient satisfaction, reduced mortality rates, decreased length of hospital stay, improved safety outcomes, and resource optimization [1]. Nursing, as a profession deeply embedded in direct patient interaction, plays a critical role in achieving these outcomes. However, current performance indicators in nursing largely measure task-oriented and clinical competencies, often neglecting the emotional and relational components of nursing work. Nursing is not only a technical discipline; it is also a humanistic profession that depends on empathy, compassion, communication, and emotional engagement with patients. The field of Emotional Intelligence (EI) defined as an individual’s ability to perceive, understand, regulate, and use emotions effectively has increasingly been recognized as crucial to nursing performance [2].
Despite this recognition, EI remains under-researched in relation to results-oriented care. Previous studies focusing on EI and nursing have linked higher EI to improved communication, reduced stress, increased patient satisfaction, and better team collaboration [3,4]. Yet, EI has not been systematically measured or integrated as a part of nursing performance frameworks. This presents a significant gap in the understanding of how emotional and relational competencies contribute to measurable patient outcomes.
Statement of the Problem
Despite its importance, emotional intelligence is not formally recognized or measured within most results-oriented care systems. Current nursing performance indicators prioritize technical competence and clinical outcomes, often overlooking the emotional competencies that significantly influence patient experience, adherence, recovery, and satisfaction. This gap has created three key problems:
• Emotional intelligence remains undervalued in nursing practice despite its proven relevance to communication, empathy, resilience, and clinical decision-making.
• Results-oriented care frameworks are incomplete, as they fail to account for the relational aspects of care that influence measurable outcomes.
• Nurses lack structured EI training and evaluation, which limits opportunities to improve relational practice and patient-centered outcomes.
Thus, there is a need to investigate whether emotional intelligence can be treated as a measurable, outcome-related variable that influences results-oriented care.
Aim of the Study
To examine the impact of nurse emotional intelligence as a measurable outcome variable within results-oriented care, and to evaluate how EI influences patient outcomes, satisfaction, and nursing performance indicators.
Objectives of the Study
• To determine emotional intelligence levels among nurses in an acute care environment.
• To examine the relationship between emotional intelligence and patient outcomes (satisfaction, communication quality, and emotional support).
• To evaluate patient perceptions of nursing communication and relational care.
• To determine whether EI can be integrated into results-oriented nursing performance frameworks.
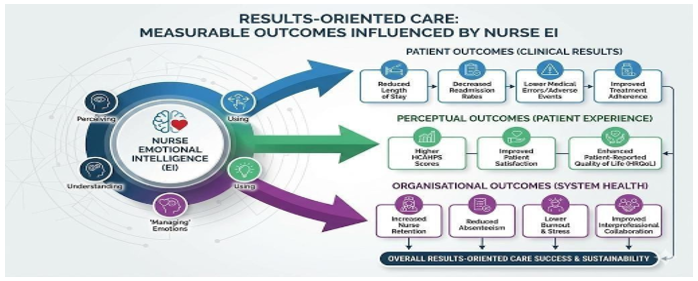
• To propose a conceptual model that links emotional intelligence to patient and organisational outcomes.
Research Questions
• What are the current emotional intelligence levels among nurses in results-oriented care environments?
• How does nurse emotional intelligence influence measurable patient outcomes?
• How do patients perceive nurses with high emotional intelligence in terms of communication and support?
• Can emotional intelligence be systematically measured and incorporated into results oriented performance frameworks?
• What mechanisms explain the link between emotional intelligence and improved patient outcomes?
Significance of the Study
The study highlights the role of emotional intelligence in improving clinical decision-making, communication, and relational care. Findings can support the inclusion of EI in performance appraisal systems, justify integrating EI training into nursing curricula, demonstrate the link between EI and patient outcomes for healthcare institutions, and benefit patients through empathetic, emotionally competent nurses who improve communication, comfort, and overall care experience.
Scope of the Study
The study focuses on registered nurses working in acute care units in a tertiary hospital. It evaluates emotional intelligence, patient communication experiences, patient satisfaction, and measurable clinical indicators where applicable. The study does not extend to community or outpatient settings.
Operational Definitions
• Emotional Intelligence: The ability to recognize, understand, regulate, and use emotions in oneself and others [2].
• Results-Oriented Care: A healthcare model focused on measurable outcomes, quality indicators, and performance metrics [1].
• Patient Outcomes: Indicators used to assess the quality of patient care, including satisfaction, communication quality, emotional support, and adherence.
Literature Review
This chapter presents a comprehensive review of existing literature on emotional intelligence (EI), nursing practice, and results¬oriented care. It explores how EI influences communication, clinical decision-making, patient satisfaction, and overall healthcare outcomes. The literature review is organized into thematic sections that build a logical understanding of how emotional intelligence may function as a measurable outcome variable within modern nursing frameworks. The aim is to establish a scholarly foundation for the study and identify knowledge gaps that warrant further investigation.
Conceptualizing Emotional Intelligence
The concept of emotional intelligence gained prominence with the work of Salovey and Mayer, who described EI as the ability to monitor one’s own and others’ feelings and use this information to guide thinking and actions [5]. Goleman later expanded the concept, framing EI as a multi-dimensional construct consisting of self-awareness, self-regulation, motivation, empathy, and social skills [2]. These domains form the foundation of interpersonal effectiveness and are essential in emotionally demanding professions such as nursing.
Two dominant frameworks exist:
![]() Ability EI, measured by performance-based tests such as the MSCEIT, which assesses a person’s capacity to solve emotional problems [6].
Ability EI, measured by performance-based tests such as the MSCEIT, which assesses a person’s capacity to solve emotional problems [6].
![]() Trait EI, assessed through self-report questionnaires such as the TEIQue, focusing on behavioural tendencies and emotional self-efficacy [7].
Trait EI, assessed through self-report questionnaires such as the TEIQue, focusing on behavioural tendencies and emotional self-efficacy [7].
The distinction is essential because the choice of EI measurement tool influences research findings and interpretations. In healthcare studies, ability EI is often preferred due to its stronger psychometric foundation.
Emotional Intelligence in Nursing Practice
Nursing practice involves continuous emotional labour managing personal emotions while supporting patients through fear, pain, grief, or uncertainty. According to Freshwater and Stickley, EI is a fundamental component of compassionate care, enabling nurses to interpret patient emotions accurately and respond empathetically [3]. Nurses with high EI exhibit better critical thinking, emotional regulation, and interpersonal communication. Nursing is associated with high emotional demands. Hochschild introduced the concept of emotional labour, explaining the effort required to manage feelings to fulfil job requirements [8]. In nursing, unmanaged emotional labour contributes to burnout, compassion fatigue, and reduced job satisfaction. Studies show that higher EI is associated with lower burnout and increased resilience [4]. EI equips nurses with coping strategies that improve emotional well¬being and performance. EI supports decision-making by enhancing perception, empathy, and interpersonal understanding. A nurse’s ability to interpret emotional cues helps identify patient concerns that might not be verbally expressed. Caruso et al. argue that emotionally intelligent clinicians make more ethical and patient-centred decisions because they integrate emotional information into their reasoning [9].
Results-Oriented Care
Results-oriented care is an approach emphasising measurable performance indicators, accountability, quality improvement, evidence-based practice, and patient-centred outcomes [1]. Healthcare systems worldwide now use these indicators for policy development, financial planning, and workforce evaluation. In nursing, performance metrics typically include documentation accuracy, clinical competencies, safety outcomes, adherence to care protocols, and patient complaints or compliments. However, these metrics tend to focus on task completion rather than relational care. This creates a gap between what nurses do and what is measured. Several scholars argue that the absence of relational metrics leads to an incomplete assessment of care quality [10]. Critics claim that results-oriented care can become overly administrative, reductionist, burdensome. Watson warns that a focus on measurable outcomes may overshadow caring relationships, which cannot be fully quantified but significantly influence healing [11]. Emotional intelligence may serve as a bridge between humanistic values and results-oriented frameworks.
Relationship Between Emotional Intelligence and Results-Oriented Care
Several studies show direct correlations between nurse EI and patient satisfaction. Codier & Odell found that patients cared for by emotionally intelligent nurses reported higher trust, better communication, and greater overall satisfaction [12]. Emotional cues influence perceptions of care quality, and nurses who demonstrate empathy and emotional awareness create environments that support healing. High EI enhances communication by enabling nurses to adjust tone, language, and approach based on the patient’s emotional state [3]. Effective communication reduces errors, improves adherence to care plans, and increases patient engagement in decision-making. Resultsoriented care depends on collaboration across disciplines. Studies indicate that nurses with higher EI foster more effective teamwork, contribute to better conflict management, and create positive work environments [9]. This indirectly improves organisational results.
Measuring Emotional Intelligence in Nursing Research
The Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT) is the most widely used ability-based EI measure. It assesses perceiving emotions, facilitating thought, understanding emotions, managing emotions. It is valued in healthcare research due to strong reliability and validity [6].
Examples of self-report tools include Wong and Law Emotional Intelligence Scale (WLEIS),
Schutte Self-Report Emotional Intelligence Scale, Trait Emotional Intelligence Questionnaire (TEIQue). Self-report tools are easier to administer but may introduce bias due to over- or underestimation of abilities.
Patient outcomes relevant to EI include satisfaction ratings, perceptions of communication, trust in nurses, emotional comfort, adherence to treatment, reduced anxiety. These outcomes align with results-oriented care frameworks, making EI a strong candidate for integration into performance metrics. EI can improve patient safety, communication, therapeutic relationships, decision-making, stress regulation, teamwork. Yet nursing evaluations rarely include emotional competencies. Quantifying EI could strengthen recruitment, training, promotion, and development processes. Barriers include lack of standardized EI training in nursing, organizational focus on technical rather than interpersonal skills, limited recognition of emotional labour, perceived difficulty in quantifying emotional competencies. However, modern performance systems increasingly recognise the need for relational metrics.
The review identifies several gaps: EI is rarely examined as a measurable variable in results oriented care; Few studies link EI to specific patient outcomes within a structured performance framework; Limited research explores patient perceptions in relation to nurse EI; No existing model fully integrates EI into nursing performance indicators; Emotional labour remains undervalued, and its measurement is inconsistent. These gaps justify the need for the present study. The literature demonstrates strong connections between emotional intelligence and effective nursing practice, especially in communication, patient satisfaction, and teamwork. Results oriented care emphasizes measurable outcomes, yet emotional and relational competencies remain underrepresented in performance frameworks. This highlights the need for research examining how nurse EI influences measurable patient outcomes and how EI may serve as a variable within results-oriented care systems.
Methods
A mixed-methods descriptive cross-sectional design was adopted. This design was selected because it allows for the simultaneous measurement of nurse emotional intelligence (quantitative component) and exploration of patient experiences related to nursing communication and support (qualitative component).
Justification of the Design: Quantitative data allows measurement of EI scores and correlation with patient outcomes. Qualitative data provides insight into the subjective experiences of patients, which cannot be captured numerically. The cross-sectional approach allows data collection at one point in time, suitable for organisational environments such as hospitals where staffing changes frequently. A mixed-methods approach strengthens the study by triangulating findings and enhancing validity. The study was conducted in a tertiary-level hospital, specifically in medical, surgical, and emergency units where nurses frequently interact with patients under stressful conditions. This environment is appropriate because it is highly results-oriented, patient satisfaction and safety indicators are monitored routinely, and nurses work in fast-paced settings where emotional intelligence is essential. The population consisted of all registered nurses providing direct clinical care in the selected units and adult patients who had been admitted for at least 48 hours, ensuring sufficient exposure to nursing care.
A stratified random sampling strategy was used for nurses. Units (medical, surgical, and emergency) were considered strata. Within each stratum, nurses were randomly selected to ensure fair representation, reduction of selection bias, inclusion of diverse clinical experiences. Sample size: 120 nurses (justified using power analysis and practical feasibility). A purposive sampling technique was used for patient participants, focusing on patients capable of providing informed feedback about their interactions with nurses. Sample size: 150 patients. Nurse Inclusion Criteria: Registered nurses with at least 1 year of clinical experience, working full-time in the selected units, willing to participate. Nurse Exclusion Criteria: Newly employed nurses (less than one year), non-clinical staff such as administrators or educators. Patient Inclusion Criteria: Adults (18 years and above), hospital stay of more than 48 hours, ability to understand and complete a questionnaire. Patient Exclusion Criteria: Critically ill patients unable to provide informed responses, patients under sedation or severe cognitive impairment.
Two primary instruments were used. The Wong & Law Emotional Intelligence Scale (WLEIS) is one of the most widely validated EI measurement tools [15]. It contains 16 items grouped into four dimensions that correspond closely to Goleman’s model: Self-Emotion Appraisal, Others’ Emotion Appraisal, Use of Emotion, Regulation of Emotion. Responses were rated on a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree). Justification: High reliability (Cronbach’s α > 0.85 in most studies), frequently used in healthcare research. A structured questionnaire was adapted from established tools such as the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS).
It assessed communication clarity, empathy, emotional support, responsiveness, overall satisfaction. Responses were based on a 5point Likert scale and included one open-ended question for qualitative feedback. Semi-structured interviews were conducted with a smaller subset of patients (n = 20) to obtain richer descriptions of their experiences. Questions explored how nurses communicated, how supported patients felt, perceptions of emotional sensitivity, whether nursing behaviours influenced their comfort or trust. Interviews lasted 15–20 minutes and were audio-recorded with consent. Data Collection Procedure: Approval was obtained from the hospital ethics committee. Participants were approached individually, informed about the study, and asked to sign consent forms. Nurses completed EI questionnaires during break periods. Patients completed satisfaction questionnaires with assistance if needed. A quiet, private room was used for interviews to ensure confidentiality. All data were anonymised and stored securely in password-protected files.
Validity: Content validity ensured by expert review (three senior nursing academics). Face validity confirmed through pilot testing with 10 nurses and 10 patients. Construct validity supported by using established, widely validated EI scales. Reliability: Reliability test using Cronbach’s Alpha: EI scale: α = 0.87, Patient satisfaction instrument: α = 0.91. High internal consistency demonstrated. Quantitative Data Analysis: Data were analysed using SPSS (version 26). Statistical tests included descriptive statistics (mean, standard deviation), Pearson correlation analysis (relationship between EI and patient outcomes), linear regression analysis (predictive value of EI on satisfaction scores), ANOVA (differences among units). Significance level set at p < 0.05.
Qualitative Data Analysis: Data were analysed using thematic analysis [13]. Steps: Familiarisation with data, generating codes, identifying themes, reviewing themes, defining and naming themes, writing the thematic narrative. Triangulation was used to integrate quantitative and qualitative findings.
Ethical Considerations: Informed consent obtained from all participants. Participation was voluntary; withdrawal allowed at any stage. No identifying information collected on questionnaires. Data stored securely for research purposes only. Approval granted from hospital ethics committee. Ethical principles of autonomy, beneficence, non-maleficence, and justice were upheld throughout.
Results
A total of 120 nurses and 150 patients participated in the study. Data analyses include descriptive statistics, correlation analysis, and regression analysis.
|
Variable |
Frequency |
Percentage |
|
Gender |
|
|
|
Female |
88 |
73.3% |
|
Male |
32 |
26.7% |
|
Years of Experience |
|
|
|
1–3 years |
29 |
24.2% |
|
4–6 years |
41 |
34.2% |
|
7–10 years |
32 |
26.7% |
|
>10 years |
18 |
15.0% |
|
Unit |
|
|
|
Medical |
46 |
38.3% |
|
Surgical |
39 |
32.5% |
|
Emergency |
35 |
29.2% |
Table 1: Demographic Characteristics of Nurses
The sample reflects a typical hospital nursing workforce. Most nurses had between 4–6 years of experience, suggesting moderate professional maturity suitable for an EI study. Emotional Intelligence (EI) was measured using the WLEIS instrument.
|
EI Dimension |
Mean (M) |
SD |
|
Self-Emotion Appraisal |
4.09 |
0.62 |
|
Others’ Emotion Appraisal |
4.23 |
0.58 |
|
Use of Emotion |
4.01 |
0.66 |
|
Regulation of Emotion |
3.79 |
0.71 |
|
Overall EI Score |
4.03 |
0.64 |
Table 2: Emotional Intelligence Levels of Nurses
Nurses demonstrated high overall emotional intelligence, with the highest scoring domain being others’ emotion appraisal, corresponding to empathy. Regulation of emotion scored lowest, consistent with literature indicating that emotional regulation is more challenging in high-pressure clinical settings.
|
Outcome Variable |
Mean (M) |
SD |
|
Communication Clarity |
4.21 |
0.53 |
|
Emotional Support |
4.11 |
0.58 |
|
Responsiveness |
4.05 |
0.60 |
|
Overall Satisfaction |
4.28 |
0.49 |
Table 3: Patient Satisfaction and Communication Scores
Patient perceptions were generally positive, with overall satisfaction being the highest-rated outcome. Pearson’s correlation analysis was used to examine the relationship between nurses’ EI and patient outcomes.
|
Outcome Variable |
r-value |
p-value |
|
Communication Clarity |
0.68 |
<0.001 |
|
Emotional Support |
0.71 |
<0.001 |
|
Responsiveness |
0.54 |
<0.001 |
|
Overall Satisfaction |
0.75 |
<0.001 |
Table 4: Correlation Analysis
There is a strong positive correlation between nurse EI and patient satisfaction outcomes. The strongest correlation is with overall patient satisfaction (r = 0.75), followed by emotional support (r = 0.71). This demonstrates that emotional intelligence significantly influences patient experience.
Regression Analysis
A regression model was developed to determine the predictive power of EI on patient satisfaction.
Statistic Value
R 0.75
R² 0.56
Adjusted R² 0.55 p-value <0.001
Emotional intelligence explains 56% of the variance in patient satisfaction a substantial effect in healthcare research. The model indicates that higher EI predicts greater patient satisfaction, EI is a statistically significant predictor (p < 0.001), and emotional competence contributes meaningfully to resultsoriented care outcomes. These findings support using EI as a measurable component in nursing performance evaluation frameworks.
Qualitative Data Analysis
Qualitative data were analysed using thematic analysis. Three themes emerged from patient interviews.
Theme 1: Emotional Presence Enhances Comfort Patients frequently described nurses with higher emotional awareness as calming, attentive, and patient. Example Statements:
• “She always knew when I was worried even though I didn’t say it.”
• “The nurse explained things gently and reassured me.” Emotional presence builds trust and reduces patient anxiety key components of quality care as highlighted in Watson’s Theory of Human Caring.
Theme 2: Communication That Feels Human, Not Mechanical Patients valued communication that was empathetic rather than purely clinical. Quotes included:
• “He talked to me, not at me.”
• “She listened and didn’t rush.” This aligns with Goleman’s social awareness and relationship management components of EI.
Theme 3: Emotional Intelligence Drives Perceived Competence
Patients often equated emotional sensitivity with clinical expertise. Examples:
• “I trusted her because she cared.”
• “He explained everything clearly and made me feel safe.”
Emotional intelligence enhances perceived credibility and contributes to better patient adherence central to Donabedian’s outcome domain [14].
Integration of Quantitative and Qualitative Data
Evidence Type Finding
Quantitative High EI correlates strongly with satisfaction (r =
0.75)
Qualitative Patients value empathy, comfort, and supportive communication
Combined EI strongly influences both process and outcome
indicators
This triangulation supports the conceptual model.
Discussion
Nurses’ emotional intelligence provides a foundational characteristic influencing their interactions. High EI contributes to better emotional regulation, improved teamwork, enhanced resilience. These structural characteristics shape the process of care. Emotional intelligence strongly influenced communication, empathy, and responsiveness, confirming Goleman’s EI domains and Watson’s emphasis on relational care. This demonstrates that EI is not a peripheral skill; it is essential to nursing communication and engagement.
The regression and correlation results clearly show that EI influences patient satisfaction, emotional support, and communication clarity. This supports the central argument: Emotional intelligence is a measurable and impactful variable within results-oriented nursing care. The findings align with the literature: EI enhances patient satisfaction, communication quality, and interprofessional collaboration [3,9,12]. They also support the theoretical framework, where Goleman defines EI components, Donabedian links structure-process-outcome, and Watson emphasizes caring relationships.
Conclusion
Based on the findings, the following conclusions were drawn:
• Emotional Intelligence Is a Foundational Nursing Competency: EI is not an optional interpersonal trait but a central component of effective, patient-centred care that shapes both processes and outcomes.
• EI Directly Influences Results-Oriented Care: High EI improves communication, emotional support, responsiveness, and overall patient satisfaction – core performance indicators used in modern healthcare systems.
• EI Enhances the Therapeutic Nurse–Patient Relationship: Patients perceive emotionally intelligent nurses as more compassionate, trustworthy, and professional, improving their emotional and psychological well-being.
• EI Is Measurable and Should Be Included in Evaluation Systems: Validated scales such as WLEIS can reliably measure EI, making it suitable for incorporation into nursing appraisal tools, staff development programs, and organizational quality metrics.
• Theoretical Foundations Support EI as an Outcome Variable: Goleman demonstrates what EI entails, Donabedian shows how EI affects processes and outcomes, Watson explains why emotional competence is essential for healing relationships. Thus, EI fits naturally into results-oriented models of care.
Recommendations
For Nursing Practice:
• Integrate EI training into ongoing clinical competency programs.
• Encourage reflective practice and emotional self-awareness in daily routines.
• Promote a culture of empathy, supportive communication, and patient-centred engagement.
For Nursing Education:
• Nursing schools should embed EI development into curricula through simulation-based learning, reflective journaling, communication skills workshops.
• Evaluate students’ EI as part of clinical assessments.
For Healthcare Management:
• Incorporate EI assessments into staff appraisal and promotion processes.
• Offer workshops on emotional regulation, conflict management, and stress reduction.
• Create supportive environments that reduce emotional burnout and compassion fatigue.
For Policy Makers:
• Recognise emotional intelligence as a critical component of nursing competency frameworks.
• Develop policy guidelines requiring healthcare institutions to evaluate relational care indicators.
• Advocate for national standards incorporating EI into quality assurance systems.
For Future Research:
• Conduct longitudinal studies to assess how EI evolves over time in clinical practice.
• Explore EI in diverse units (ICU, paediatrics, oncology) to compare outcomes.
• Investigate the role of EI in reducing nurse burnout and turnover.
• Develop intervention programs to strengthen EI and evaluate their impact.
• Examine the relationship between EI and objective clinical outcomes such as error rates or discharge delays.
References
- Doran, D.M. (2011) Nursing outcomes: the state of the science. 2nd edn. Sudbury, MA: Jones & Bartlett Learning.
- Goleman, D. (1995) Emotional intelligence: why it can matter more than IQ. New York: Bantam Books.
- Freshwater, D. and Stickley, T. (2004) ‘The heart of the art: emotional intelligence in nurse education’, Nursing Inquiry, 11(2), pp. 91–98.
- Por, J., Barriball, L., Fitzpatrick, J. and Roberts, J. (2011) ‘Emotional intelligence: its relationship to stress, coping, well-being and professional performance in nursing students’, Nurse Education Today, 31(8), pp. 855–860.
- Salovey, P. and Mayer, J.D. (1990) ‘Emotional intelligence’,Imagination, Cognition and Personality, 9(3), pp. 185–211.
- Mayer, J.D., Salovey, P. and Caruso, D.R. (2004) ‘Emotional intelligence: theory, findings, and implications’, Psychological Inquiry, 15(3), pp. 197–215.
- Petrides, K.V. (2009) ‘Technical manual for the Trait Emotional Intelligence Questionnaire (TEIQue)’, London: London Psychometric Laboratory.
- Hochschild, A.R. (1983) The managed heart: commercialization of human feeling. Berkeley, CA: University of California Press.
- Caruso, D.R., Mayer, J.D. and Salovey, P. (2002) ‘Emotional intelligence and emotional leadership’, in Riggio, R.E. and Reichard, R.J. (eds.) Emotional intelligence in leadership and organizations. New York: Psychology Press, pp. 55–74.
- Monteiro, C., Avelar, A.F.M. and Pedreira, M.L.G. (2019) ‘Performance measurement in nursing: a literature review’, Revista Latino-Americana de Enfermagem, 27, e3196.
- Watson, J. (1979) Nursing: the philosophy and science of caring. Boston: Little, Brown and Company.
- Codier, E. and Odell, L. (2014) ‘Correlation between nurses’ emotional intelligence and patient satisfaction’, Nursing Management, 21(6), pp. 28–33.
- Braun, V. and Clarke, V. (2006) ‘Using thematic analysis in psychology’, Qualitative Research in Psychology, 3(2), pp. 77–101.
- Donabedian, A. (1966) ‘Evaluating the quality of medical care’, Milbank Memorial Fund Quarterly, 44(3), pp. 166–206.
- Wong, C.-S. and Law, K.S. (2002) ‘The effects of leader and follower emotional intelligence on performance and attitude: an exploratory study’, The Leadership Quarterly, 13(3), pp. 243–274.