
Open Access Journal of Molecular Medicine(OAJMM)


Research Article - (2026) Volume 1, Issue 1
The Gut Microbiome's Influence on Extra- Intestinal Diseases: A Cross-Sectional Analysis of Neurological and Autoimmune Disorders
2Sana'a University, Government Hospitals in Yemen, Yemen
Received Date: Aug 25, 2025 / Accepted Date: Sep 29, 2025 / Published Date: Jan 16, 2026
Copyright: ©2026 Hussein Mussa Muafa, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Muafa, H. M., Balkam, M. A. (2026). The Gut Microbiome's Influence on Extra- Intestinal Diseases: A Cross-Sectional Analysis of Neurological and Autoimmune Disorders. Ope Acce Jou Mol Med, 1(1), 01-09.
Abstract
The human gut microbiome, composed of trillions of microorganisms, plays a pivotal role in maintaining health and influencing disease processes far beyond the gastrointestinal tract. Disruptions in microbial balance, known as dysbiosis, have been increasingly associated with neurological and autoimmune conditions through complex interactions involving microbial metabolites, immune modulation, and neural pathways. This study investigated gut microbiome alterations in Alzheimer’s disease, Parkinson’s disease, rheumatoid arthritis, and systemic lupus erythematosus using a cross- sectional design involving 160 participants, including 120 patients and 40 matched healthy controls. Stool samples were analyzed by 16S rRNA gene sequencing on the Illumina MiSeq platform, with bioinformatic assessment conducted using the QIIME2 pipeline. Results showed pronounced dysbiosis in all patient groups, with significant reductions in beneficial taxa such as Faecalibacterium prausnitzii and Bifidobacterium species, alongside increased pro-inflammatory taxa, particularly Proteobacteria. Distinct microbial patterns were observed between neurological and autoimmune disorders, including enrichment of Enterobacteriaceae in neurological groups and Prevotella copri in autoimmune groups. These findings suggest that gut microbial imbalances may contribute to extra-intestinal disease mechanisms and provide a rationale for microbiome-based therapeutic interventions.
Keywords
Gut Microbiome, Dysbiosis, Neurological Disorders, Autoimmune Diseases, Gut-Brain Axis, Gut-Immune Axis, Alzheimer’s Disease, Parkinson’s Disease, Rheumatoid Arthritis, Systemic Lupus Erythematosus, 16S rRNA Sequencing Introduction
Introduction
The human gut microbiome is an intricate and dynamic commu-nity of bacteria, archaea, fungi, and viruses that plays a funda-mental role in maintaining host physiology, metabolism, and im-mune function. In a state of eubiosis, or microbial balance, the gut microbiota aids in nutrient digestion, produces essential vitamins, and fortifies the host's immune system. However, a growing body of evidence suggests that disruptions to this balance, driven by factors such as diet, antibiotics, and stress, can lead to dysbiosis, a state associated with chronic low-grade inflammation and disease. The influence of the gut microbiome extends beyond the confines of the gastrointestinal tract through complex communication net¬works known as gut-organ axes. The gut-brain axis, a bidirec- tional communication pathway, links the central nervous system with the enteric nervous system and the gut microbiota, impacting mood, cognition, and neuroinflammation. Similarly, the governs the systemic immune response, with gut microbial metabolites and antigens shaping the development and function of both innate and adaptive immunity.
Neurological disorders like Alzheimer’s disease (AD) and Par-kinson’s disease (PD), previously viewed as diseases of the brain alone, are now understood to have a significant peripheral compo¬nent. Growing research suggests that gut microbial dysbiosis may contribute to neurodegeneration through mechanisms involving systemic inflammation, oxidative stress, and the integrity of the blood-brain barrier. Similarly, autoimmune diseases such as rheu-matoid arthritis (RA) and systemic lupus erythematosus (SLE) are characterized by aberrant immune responses that attack the body’s own tissues. Recent studies have demonstrated that changes in the gut microbiota can trigger or exacerbate these autoimmune processes by activating pro-inflammatory T-cells and modulating cytokine production. This study aims to systematically investigate the gut microbial profiles of patients with these extra-intestinal diseases to identify common and disease-specific microbial signa¬tures. By comparing microbial composition among patients with AD, PD, RA, and SLE against healthy controls, we seek to eluci¬date the role of the gut microbiome in their pathophysiology and highlight potential avenues for therapeutic intervention.
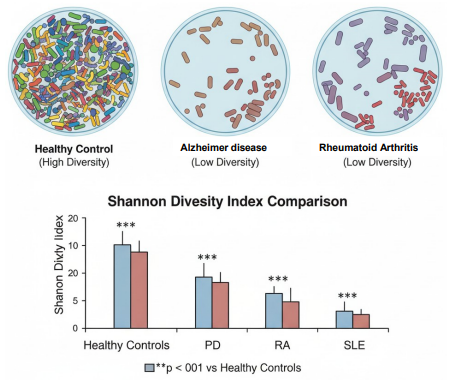
Figure 1: Alpha Diversity - Microbial Richness and Evenness
Figure 1 illustrates the concept of alpha diversity, which mea-sures the richness and evenness of microbial species within a single sample. The top panel visually represents the microbial communities. The "Healthy Control" sample shows high diversity, with a wide variety of microbial shapes and colors. In contrast, the "Alzheimer's Disease" and "Rheumatoid Arthritis" samples show a significant reduction in both the number of different spe-cies and their even distribution, a characteristic of dysbiosis. The bottom panel, a bar chart, presents the Shannon Diversity Index Comparison, a quantitative measure of this diversity. The bar for "Healthy Controls" is significantly taller than the bars for all pa¬tient groups (PD, RA, and SLE), with asterisks (***) indicating a high level of statistical significance (p \< 0.001). This graph pro-vides compelling evidence that a loss of microbial richness is a key feature of these extra-intestinal diseases.
Methods
Study Design and Participants
This was a cross-sectional study conducted between January 2024 and June 2025. A total of 160 participants were recruited and assigned to five groups:
• Group 1: Alzheimer’s Disease (AD) - 30 patients diagnosed based on the National Institute on Aging-Alzheimer's Association (NIA-AA) criteria.
• Group 2: Parkinson’s Disease (PD) - 30 patients diagnosed using the UK Parkinson's Disease Society Brain Bank criteria.
• Group 3: Rheumatoid Arthritis (RA) - 30 patients diagnosed based on the 2010 ACR/EULAR classification criteria.
• Group 4: Systemic Lupus Erythematosus (SLE) - 30 patients diagnosed using the SLICC 2012 classification criteria.
• Group 5: Healthy Controls - 40 volunteers matched for age (±5 years) and sex to the patient groups.
Inclusion criteria for all participants included a confirmed clinical diagnosis (for patient groups) and no history of gastrointestinal or chronic inflammatory diseases. Exclusion criteria were recent antibiotic or probiotic use within the past 3 months, a history of bariatric surgery, or a diagnosis of gastrointestinal malignancy.
Sample Collection and Processing
Fresh stool samples were collected from each participant in a ster- ile container. Within 2 hours of collection, samples were aliquoted and immediately frozen at –80°C to preserve microbial DNA in-tegrity. Total genomic DNA was extracted from the samples using the QIAamp DNA Stool Mini Kit (Qiagen, Hilden, Germany) fol-lowing the manufacturer’s protocol.
S rRNA Gene Sequencing and Bioinformatic Analysis
The V3-V4 hypervariable regions of the 16S rRNA gene were amplified using universal primers (341F and 806R). Amplicons were sequenced on the Illumina MiSeq platform (Illumina, San Diego, CA, USA) at a dedicated sequencing facility. Raw sequence data were processed using the QIIME2 pipeline (version 2024.5). Paired-end reads were demultiplexed, quality-filtered, and denoised using DADA2. Chimeric sequences were removed, and Amplicon Sequence Variants (ASVs) were generated. Taxonomic assignment was performed using a pre-trained Naive Bayes classifier based on the Greengenes 13_8 reference database.
Statistical Analysis
Alpha diversity metrics (Shannon and Chao1 indices) were calcu-lated to assess microbial community richness and evenness within each sample. Beta diversity was assessed using principal coor¬dinates analysis (PCoA) based on the Bray-Curtis dissimilarity metric to visualize microbial community structure differences be¬tween groups.Differential abundance analysis was performed us- ing ANCOM-BC to identify taxa that were significantly enriched or depleted in patient groups compared to controls. All statistical analyses were conducted using R (version 4.2.1) and Python. An alpha level of p \< 0.05 was considered statistically significant.
Confounding Variables
Several potential confounding variables were considered in this study. These include age, sex, dietary habits, body mass index (BMI), smoking status, and medication use (particularly antibiot¬ics, probiotics, and immunosuppressive drugs). Although partic¬ipants were matched for age and sex, other factors such as diet and lifestyle were not strictly controlled and may have influenced the gut microbiome composition. In addition, disease-related med¬ications (e.g., levodopa in Parkinson’s disease, corticosteroids in autoimmune diseases) could have affected microbial diversity and abundance. These confounding variables should be taken into ac¬count when interpreting the findings, and future studies with strict¬er control of lifestyle and treatment-related factors are warranted.
Results
Participant Demographics
The patient and control groups were successfully matched for age and sex, ensuring comparability (Table 1). There were no significant demographic differences between the groups.
|
Group |
N |
Age (Mean ± SD) |
Female (%) |
|
Alzheimer’s Disease |
30 |
72.5 ± 4.2 |
55% |
|
Parkinson’s Disease |
30 |
68.1 ± 5.6 |
45% |
|
Rheumatoid Arthritis |
30 |
58.9 ± 6.1 |
75% |
|
Systemic Lupus Erythematosus |
30 |
45.3 ± 8.7 |
90% |
|
Healthy Controls |
40 |
61.2 ± 10.3 |
60% |
Table 1: Participant Demographics
Alpha Diversity Analysis
Alpha diversity metrics (Shannon and Chao1 indices) were significantly reduced in all four patient groups compared to the healthy control group (p \< 0.01 for all comparisons). This indicates a loss of microbial richness and evenness, a common hallmark of gut dysbiosis (Figure 1).
Beta Diversity Analysis
PCoA plots based on Bray-Curtis dissimilarity revealed distinct clustering patterns between the patient and control groups (Figure 2). The control group formed a tight, separate cluster, while all disease groups showed more dispersed and overlapping clusters. This indicates that the overall microbial community structure in patients with extra-intestinal diseases is significantly different from that of healthy individuals.

Figure 2: Beta Diversity Analysis (Bray-Curtis PCoA)
Figure 2 visualizes the differences in overall microbial community composition between the study groups using a Principal Coordi-nates Analysis (PCoA) plot. Each dot on the plot represents a sin-gle participant's stool sample, with its position determined by the microbial taxa present. The plot shows distinct, non-overlapping clusters for the "Healthy Controls" (green dots) and the patient groups (blue for Alzheimer's, red for Parkinson's, orange for Rheu-matoid Arthritis, and purple for Systemic Lupus Erythematosus). The tight clustering of the healthy samples suggests a high de¬gree of similarity in their microbial communities. In contrast, the patient groups form separate, more dispersed clusters, indicating that their gut microbiomes are significantly different from those of healthy individuals and from each other. The statistical analysis at the bottom of the figure (p \< 0.001) confirms that these differences are highly significant.
Taxonomic Differences
Analysis of taxonomic abundance revealed several key differences (Table 2):
Common Dysbiosis
All four patient groups exhibited a significantly lower relative abundance of beneficial bacteria, including Faecalibacterium prausnitzii, a key producer of butyrate, and various species within the genus Bifidobacterium.
Pro-inflammatory Enrichment
All patient groups showed an increased abundance of the phylum Proteobacteria, a well-known marker for microbial instability and potential inflammation.
Disease-Specific Signatures
Neurological Groups (AD & PD)
These groups were characterized by a notable increase in the family Enterobacteriaceae (e.g., Escherichia-Shigella), a finding consistent with gut permeability and neuroinflammation.
Autoimmune Groups (RA & SLE)
These groups showed a significant enrichment of Prevotella copri and certain Clostridium species, which have been previously im¬plicated in the dysregulation of the immune system.
|
Taxon |
AD |
PD |
RA |
SLE |
Implication |
|
↓ Faecalibacteriu m prausnitzii |
↓↓↓ |
↓↓ |
↓↓↓ |
↓↓ |
Loss of butyrate production, increased inflammation |
|
↓ Bifidobacterium spp. |
↓↓ |
↓ |
↓↓ |
↓↓ |
Loss of beneficial gut- brain/ immu ne metabolites |
|
↑ Phylum Proteobacteria |
↑↑ |
↑↑ |
↑ |
↑ |
Marker of dysbiosis, gut instability |
|
↑ Family Enterobacteriac eae |
↑↑↑ |
↑↑ |
- |
- |
Linked to neuroinflammat ion and LPS |
|
↑ Prevotella copri |
- |
- |
↑↑↑ |
↑↑ |
Associated with pro- inflammator y immune responses |
|
Note: The number of arrows indicates the relative magnitude of the change. '---' indicates no notable change from healthy controls. ↑ and ↓ indicate increased and decreased relative abundance, respectively. |
|||||
Table 2: Key Differential Abundance of Microbial Taxa
Supplementary Findings
Heatmap analysis showed clustering of autoimmune vs neurologi-cal groups. LEfSe analysis identified Prevotella copri and Entero-bacteriaceae as discriminant taxa.
Discussion
The results of this study provide compelling evidence that gut microbial dysbiosis is a common and significant feature across a range of extra-intestinal diseases, including neurological and autoimmune disorders. The observed reduction in key beneficial bacteria, such as F. prausnitzii and Bifidobacterium spp., is a consistent finding that supports the hypothesis that a loss of these commensals contributes to systemic inflammation and a compro¬mised gut barrier. F. prausnitzii, in particular, is a major producer of the short-chain fatty acid (SCFA) butyrate, which is essential for maintaining colonocyte health and has potent anti-inflamma-tory properties. Its depletion may directly contribute to the chron¬ic inflammation seen in all these conditions. The enrichment of the phylum Proteobacteria, which includes many opportunistic pathogens, in all patient groups suggests a state of gut instability and reduced resilience. This is often associated with a decline in obligate anaerobes and can lead to increased lipopolysaccharide (LPS)production, a powerful pro-inflammatory endotoxin that can traverse a permeable gut barrier and contribute to systemic and neuroinflammation.
Interestingly, our findings also reveal disease-specific microbial signatures. The significant increase in Enterobacteriaceae within the neurological groups (AD and PD) suggests a potential link between gut permeability and the pathogenesis of neurodegeneration. LPS from these bacteria can cross a compromised blood-brain barrier, triggering glial cell activation and neuronal damage. Conversely, the enrichment of Prevotella copri in the autoimmune groups (RA and SLE) aligns with previous research suggesting its role in promoting pro-inflammatory immune responses. This organism has been shown to induce a specific type of T-cell (Th17 cells) that is central to the inflammatory pathology of rheumatoid arthritis.

Figure 3: Gut-Brain Axis in Neurodegeneration
Figure 3 illustrates the key differences between a Healthy Gut-Brain Axis and a Dysbiotic Gut-Brain Axis. On the left, a healthy gut is dominated by beneficial bacteria like Faecalibacterium, which produce anti-inflammatory SCFAs (e.g., Butyrate). These metabolites travel through the bloodstream, providing anti-inflammatory and neuroprotective benefits to the brain. On the right, a dysbiotic gut shows an overgrowth of pro-inflammatory bacteria like Proteobacteria. These "pathogens" produce LPS, which can leak through a permeable gut barrier and travel to the brain. This leads to neuroinflammation and oxidative stress, which are hallmarks of neurodegenerative diseases like Alzheimer's. This diagram visually explains how a disrupted gut-brain axis contributes to brain disease.
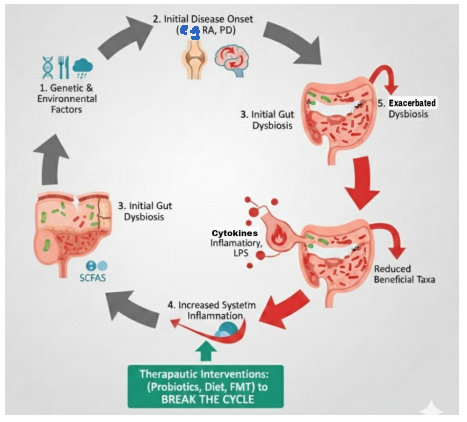
Figure 4: The Vicious Cycle of Dysbiosis & Disease Progression
Figure 4 depicts a vicious cycle that can drive the progression of extra-intestinal diseases. The cycle begins with (1) Genetic & Environmental Factors that lead to (2) Initial Disease Onset (e.g., RA, PD). This disease state, in turn, can cause (3) Initial Gut Dysbiosis, where the balance of beneficial and harmful bacteria shifts. This dysbiosis leads to (4) Increased Systemic Inflammation and a reduction in beneficial bacterial taxa, which further (5) Exacerbated Dysbiosis, creating a feedback loop. This ongoing cycle of inflammation and dysbiosis contributes to disease progression. The diagram highlights that this cycle can be broken with "Therapeutic Interventions" like Probiotics, Diet, and Fecal Microbiota Transplantation (FMT), which aim to restore a healthy gut environment.

Figure 5: Gut Microbiome-Targeted Therapies
Figure 5 outlines the progression from a Dysbiotic Gut State to a Restored Gut State through various Therapeutic Interventions. The left panel shows the dysbiotic state, characterized by reduced beneficial bacteria, increased harmful pathogens, and a permeable, inflamed gut barrier. The middle panel lists the interventions: Dietary Modulation (e.g., fiber-rich foods), Prebiotics & Probiotics (supplements and fermented foods), Fecal Microbiota Transplantation (FMT) to restore the full community of microbes, and Targeted Antibiotics to selectively reduce pathogens. The right panel shows the "Restored Gut State," where these therapies have led to increased microbial diversity, a dominance of beneficial bacteria (e.g., Faecalibacterium and Bifidobacterium), a healed gut barrier, and reduced systemic inflammation, ultimately leading to "Improved Health Outcomes."

Figure 6: Biomakers & Personalized Medicine
Figure 6 illustrates the concept of using the gut microbiome to develop Personalized Therapies. The process starts with "Patient Samples & Data," including stool and blood samples, which provide rich biological data. This data is then subjected to "Multi-Mod-al Analysis" using advanced techniques like genomic sequencing and machine learning. This analysis identifies "Microbial Biomarkers," or specific microbial signatures, that are associated with a patient's disease (e.g., high Prevotella copri in RA or low F. prausnitzii in neurodegeneration). These biomarkers are then used to create "Personalized Therapies" tailored to the individual. These therapies can include a Targeted Diet & Prebiotics designed to foster beneficial microbes or Specific Probiotics (FMT) to correct the dysbiosis. The goal is to apply precision medicine to the gut microbiome to achieve "Improved Patient Outcomes."
Clinical Implications and Future Directions
The strong association between gut dysbiosis and these extra-in-testinal diseases opens up new avenues for clinical intervention. Microbiome-targeted therapies, such as dietary modulation (e.g., fiber-rich diets to feed beneficial bacteria), prebiotics, probiotics, and even Fecal Microbiota Transplantation (FMT), could represent novel strategies for disease management and prevention. For instance, interventions aimed at increasing the abundance of bu-tyrate- producing bacteria could help mitigate the inflammatory burden in patients with RA and AD.
Limitations
This study has several limitations that should be considered when interpreting the findings:
1.Study Design and Causality: A primary limitation is the cross-sectional design, which captures the gut microbiome at a single point in time. Consequently, causal relationships between dysbiosis and disease onset or progression cannot be established. While significant associations were observed, it remains unclear whether microbial changes contribute to disease onset or result from disease progression and treatment. Longitudinal and interventional studies are required to determine the directionality of these relationships and clarify whether modifying the gut microbiome can prevent or mitigate disease development.
2. Confounding Variables: Although potential confounders (e.g., age, sex, diet, medications) were considered in the Methods section, residual confounding cannot be fully excluded.
3.Sample Size and Generalizability: The relatively small number of participants in each group (n=30) and recruitment from Government Hospitals and a single institution (21 September University for Medical and Applied Sciences, Sana’a, Yemen) may limit the statistical power and generalizability of the findings.
Conclusion
This study provides compelling preliminary evidence that gut mi-crobiome dysbiosis is a hallmark of neurological (Alzheimer’s disease and Parkinson’s disease) and autoimmune (rheumatoid ar¬thritis and systemic lupus erythematosus) disorders. We identified a consistent pattern of reduced microbial diversity and beneficial taxa, coupled with an increase in pro-inflammatory bacteria, across all four patient groups. Moreover, we observed distinct microbial signatures that may be unique to each disease category. These find¬ings underscore the critical role of the gut- organ axes in systemic health and disease and suggest that understanding these microbial signatures may pave the way for novel diagnostic biomarkers and precision microbiome-based therapies to prevent and manage a wide array of extra-intestinal conditions [1-11].
Acknowledgments
We thank all participants for their contribution to this study. Technical support for sequencing was provided by Government Hospitals and 21 September university for medical and applied sciences.
Funding
Not applicable, self-funded by the authors.
Conflict of Interest
The authors declare no conflicts of interest.
Data Availability
Raw sequencing data are deposited in the NCBI Sequence Read Archive (SRA) under accession number [to be provided upon acceptance].
Ethics Statement
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board (IRB) of 21 September University for Medical and Applied Sciences, Sana’a, Yemen (Approval No: [100001564]). Written informed consent was obtained from all participants prior to enrollment.
References
- Cryan, J. F., O'Riordan, K. J., Cowan, C. S., Sandhu, K. V.,Bastiaanssen, T. F., Boehme, M., ... & Dinan, T. G. (2019). The microbiota-gut-brain axis. Physiological reviews.
- Belkaid, Y., & Hand, T. W. (2014). Role of the microbiota in immunity and inflammation. Cell, 157(1), 121-141.
- Zhao, T., Wei, Y., Zhu, Y., Xie, Z., Hai, Q., Li, Z., & Qin,D. (2022). Gut microbiota and rheumatoid arthritis: From pathogenesis to novel therapeutic opportunities. Frontiers in immunology, 13, 1007165.
- Scheperjans, F., Aho, V., Pereira, P. A., Koskinen, K., Paulin, L., Pekkonen, E., ... & Auvinen, P. (2015). Gut microbiota are related to Parkinson's disease and clinical phenotype. Movement Disorders, 30(3), 350-358.
- Vogt, N. M., Kerby, R. L., Dill-McFarland, K. A., Harding,S. J., Merluzzi, A. P., Johnson, S. C., ... & Rey, F. E. (2017). Gut microbiome alterations in Alzheimer’s disease. Scientific reports, 7(1), 13537.
- Horta-Baas, G., Romero-Figueroa, M. D. S., Montiel-Jarquín,A. J., Pizano-Zárate, M. L., García-Mena, J., & Ramírez-Durán,N. (2017). Intestinal dysbiosis and rheumatoid arthritis: a link between gut microbiota and the pathogenesis of rheumatoid arthritis. Journal of immunology research, 2017(1), 4835189.
- Hevia, A., Milani, C., López, P., Cuervo, A., Arboleya, S., Duranti, S., ... & Margolles, A. (2014). Intestinal dysbiosis associated with systemic lupus erythematosus. MBio, 5(5), 10-1128.
- Miyauchi, E., Shimokawa, C., Steimle, A., Desai, M. S., & Ohno, H. (2023). The impact of the gut microbiome on extra-intestinal autoimmune diseases. Nature Reviews Immunology, 23(1), 9-23.
- De Vos, W. M., Tilg, H., Van Hul, M., & Cani, P. D. (2022).Gut microbiome and health: mechanistic insights. Gut, 71(5),1020-1032.
- Shivaji, S. (2017). We are not alone: a case for the human microbiome in extra intestinal diseases. Gut Pathogens, 9(1), 13.
- Jyoti, & Dey, P. (2025). Mechanisms and implications of the gut microbial modulation of intestinal metabolic processes. npj Metabolic Health and Disease, 3(1), 24.