
International Journal of Diabetes & Metabolic Disorders(IJDMD)
ISSN: 2475-5451 | DOI: 10.33140/IJDMD
Impact Factor: 1.23


Research Article - (2024) Volume 9, Issue 1
The Ability of Combination Sulfonylurea and Metformin in Reducing Morbidity and Mortality in Type 2 Diabetes
Received Date: Apr 12, 2024 / Accepted Date: May 13, 2024 / Published Date: May 16, 2024
Copyright: ©© 2024 Gary G. Adams, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Fletcher, K., Meal, A., Adams, G. G. (2024). The Ability of Combination Sulfonylurea and Metformin in Reducing Morbidity and Mortality in Type 2 Diabetes. Int J Diabetes Metab Disord, 9(1), 01-10.
Abstract
Background Literature: Type 2 diabetes is a health concern worldwide, and treatment with oral antidiabetic medicines presents a clinical challenge. This systematic review aims to assess the ability of combination sulfonylurea and metformin in reducing morbidity and mortality in type 2 diabetes.
Methods A search of the databases NU Search, PubMed, Ovid, Embase, CINAHL and Medline was conducted by the author, using key search terms. 11 studies were included, 6 RCT’s, and 5 cohort studies with a combined number of 168,138 participants.
Results Cardiovascular risk: Atherosclerotic Cardiovascular Disease (ASCVD) risk score DPP4i and metformin: -1.5 versus -1.1 for SU and metformin. Six studies found no difference for MI, CVD, stroke across groups for SU, DPP4i, or SGLT2i. DPP4i combination was superior, with better protective effects than SU combined for, Heart failure (HF) HR 0.86 DPP4i versus 1.0 SU, Cerebrovascular disease HR 0.72 versus 1.0 Myocardial Infarction (MI), DPP4i= 340, HR 1.0, versus SU =402, HR 0.84. HbA1c reductions across groups: SU -1.59, DPP4i -2.43 versus -2.91 with SGLT2i. More rapid reduction with SU and metformin versus SGLT2i and DPP4i from 0- week 18. Weight changes across groups: weight gain with SU 5.72kg, versus – 4.27kg for DPP4i and – 20.7kg for SGLT2i.
Conclusion Cardiovascular risk was inconclusive. SU’s were shown to be associated with a rapid reduction of HbA1c and weight gain. More robust research is needed to examine further combination oral antidiabetic treatments and cardiovascular risk, as a high level of heterogeneity (I2 ) and bias between the studies existed.
Introduction
The World Health Organisation (WHO) (2022) estimated that between 1980 to 2014, the prevalence of diabetes increased from 108 million to 422 million worldwide. Diabetes takes many different forms, such as type 1, type 2, gestational, type 3, Maturity Onset Diabetes of the Young (MODY), and Latent Autoimmune Diabetes in Adults (LADA) (Diabetes UK, 2019). Type 2 diabetes accounts for around 85% of the diabetic population, making it the most prevalent type [1]. During normal physiological conditions, blood glucose level is maintained and regulated by the islets of Langerhans located in the pancreas; insulin is secreted in response to elevated glycaemic levels and facilitates the transfer of glucose into muscle and fat cells for energy utilisation [1].
Under abnormal conditions in type 2 diabetes, however, the pancreas fails to produce sufficient insulin, or the insulin produced is deficient. This progressive autoimmune disease is linked to genetic causes, obesity and/or poor diet [2]. Metformin, a common treatment for type 2 diabetes, is part of the biguanide class of medicines and functions in reducing hepatic glucose output by suppressing gluconeogenesis. In contrast, sulfonylureas act by stimulating the pancreatic beta cells to increase the amount of insulin released and efficiency [3]. Here, the authors examined if combinatorial Sulfonylurea and Metformin therapy had the ability to reduce morbidity and mortality in Type 2 Diabetes.
Methodology
A comprehensive search of the databases NU Search, PubMed, Ovid, Embase, CINAHL and Medline was undertaken to identify studies for inclusion. The inclusion criteria were patients with type 2 diabetes, aged >18, taking metformin and/or sulfonylureas, assessing the safety and efficacy of combination therapy. The exclusion criteria were participants with other types of diabetes, patients aged <18, and patients taking insulin or other subcutaneous injection anti-diabetes medications. The following key search terms were entered into the selected online databases: type 2 diabetes + oral + metformin + sulfonylurea + adults + morbidity + mortality.
The search returned a total of 1057 studies. After reviewing each study manually, and assessing against inclusion and exclusion criteria, 1045 studies were excluded. A total of 11 studies met the inclusion criteria and were included in this review. A Critical Appraisal Skills Programme (CASP, 2020) was utilised for data extraction and assess the risk of bias. Each study was read, synthesized and the main outcomes described.
Results and Discussion
Theme one - Cardiovascular risk
Cardiovascular risk and diabetes have a well-documented association, and Diabetes UK (2019) states that the risk is increased by 2 and a half times for stroke or heart attack, which highlights the importance of reducing the risk. Ten of the eleven studies by Gillani et al. (2022), Wang, Wua, and Chiena, (2021), Douros et al. (2018), Chang et al. (2015), Leiter et al. (2015), Nauck et al. (2014), Del Prato et al. (2014), Hassan and Abd-Allah (2015), Pantalone et al. (2012), and Nauck et al. (2011) reported cardiovascular risk/mortality for 166,767 participants [4 -13]
Dpp4i Versus Sulfonylurea and Metformin
Of the ten studies, two of the studies by Gillani et al. (2022) and Wang et al. (2021) revealed that combination metformin and DPP4i versus SU and metformin, concurred that DPP4i combination had better cardioprotective effects [4,5]. Assessed Atherosclerotic Cardiovascular Disease (ASCVD) risk and identified a significant mean reduction -1.1 % from baseline for sulfonylureas plus metformin combined, and DPP4i and metformin – 1.56%. SU and DPP4i were both found to reduce ASCVD risk score, however DPP4i’s were superior. The study also found gliclazide exhibited an enhanced cardiovascular profile to glimepiride. The results of Wang et al. (2021) found that DPP4i combination was superior, with better protective effects than SU combined for, Heart failure (HF) HR 0.86 DPP4i versus 1.0 SU, Cerebrovascular disease HR 0.72 versus 1.0 Myocardial Infarction (MI), DPP4i= 340, HR 1.0, versus SU =402, HR 0.84 [5].
Metformin and Sulfonylurea Combinations
Of the ten studies, two by Hassan and Abd-Allah (2015) and Pantalone et al [11,12]. Assessed different combinations of SU and metformin. Assessed lipid profiles, and found Low density lipoprotein (LDL) improved from baseline, but suggested greater reduction of cardiovascular risk with glimepiride and metformin 142+7, versus gliclazide and metformin 146+7. Pantalone et al. (2012) found no significant difference in mortality across groups with metformin plus, glimepiride, versus metformin and glipizide HR 1.03, or metformin plus glimepiride HR 1.03 or glipizide and metformin versus metformin plus glibenclamide, HR 1.05. there were 636 deaths in the cohort [12].
Sulfonylurea and Metformin Versus SGLT2i
Leiter et al. (2015) assessed high density lipoprotein (HDL) and was found to be reduced in patients that received metformin and sulfonylurea combination 0.06 versus SGLT2i 0.38, however this was not statistically significant. Nauck et al. (2011), also reported results concomitant with Leiter et al. (2015) that HDL was increased in the SGLT2i group and reduced in the SU group. The 156-week extension study Nauck et al. (2014) did not report outcomes HDL. The extension study by Nauck et al. (2014) reported the additional cardiac outcomes, coronary artery occlusion (CAO) and aortic aneurysm (AA) but no differences were identified across groups [8,13]
Sulfonylurea and Metformin Vs Glinides and A- Glucosidase
Chang et al. (2015) identified that the metformin and glinides, N=9 or alpha glucosidase inhibitor N=13, Versus N=323 in SU and metformin group. significantly reduced the risk of MI, but showed no variance in risk of stroke or HF.
Sulfonylureas and Metformin Versus Sglt2i, Dpp4i And Su Combinations
Six of the ten studies by Douros (2018), Chang et al. (2015), Del Prato et al. (2014), Nauck et al. (2014), Pantalone et al. (2012) and Nauck et al. (2011) found no substantial difference between the study groups for cardiovascular risk of different events, including cardiovascular death, MI, CVD, stroke and heart failure, between combination SU with metformin, versus SGLT2i, DPP4i, and SU combinations. Though it would be important to note Nauck et al. (2011) suggested that persistent reduction in systolic blood pressure and weight with SGLT2i may exert a favourable effect on cardiovascular risk, but not a significant finding [6,7,9, 10,12,13].
After reviewing the results from all ten studies assessing cardiovascular risk and mortality, the studies confirm that combination metformin and sulfonylurea reduced cardiovascular risk to a degree, and some SU’s might be associated with a further reduced risk than others. However, the evidence is not strong enough to form a sound conclusion on the different types of SU. When comparing the performance of metformin and sulfonylureas to other anti-diabetic medicines, the results were inconclusive. Six out of ten, did not show a meaningful reduction of cardiovascular risk. More robust research is needed to further investigate this points out that SGLT2i combination with metformin may provide beneficial cardioprotective effects, which is supported by the current guidance by the National Institute for health and Care Excellence (2015) which advocates the use of SGLT2i for patients with cardiovascular risk or existing cardiac disease, rather than SU which is in keeping with the findings from the studies included in this review [4,5,11]. conducted their studies in settings that were vastly different, Malaysia, Egypt and Taiwan which limits the generalisations that can be made from this research. Two of the studies by Gillani et al. (2022) and Wang et.al. (2021) indicated enhanced cardioprotective effects of DPP4i in comparison to SU, however both had risk of bias. Gillani et al. (2022) may have introduced selection bias, as participants self-referred or were recommended by study sites [2,5]. Wang et al. (2021) had a large sample size which increases the validity. However, the retrospective cohort study design, reduces the strength of the results [5]. Additionally, the information was taken from an insurance database where there was potential for data to be missing. In the initial study by Nauck et al. (2011) HDL was reported as increased with the SGLT2i group and reduced in the SU groups [13]. The extension study Nauck et al. (2014), did not report outcomes for HDL, this could indicate reporting bias [14].
Theme Two - HbA1c Reduction
The second theme emerging from the results was HbA1C levels. Chen et al. (2015) explained that macrovascular complications in diabetes are associated with poor control of HbA1c and is linked to the pathophysiology of vascular damage.
Eight of the eleven studies by Gillani et al. (2022), Muskiet et al. (2020), Hollander et al. (2017) Hassan and Abd-Allah (2015), Leiter et al. (2015), Del Prato et al. (2014), Nauck et al. (2014) Nauck et al. (2011) assessed outcome for HbA1c levels in 8925 participants.
Sulfonylurea and Metformin Versus Dpp4i and Metformin
Two of the eight studies by Gillani et al. (2022) and Del Prato et al. (2014) found whilst HbA1c was improved with SU’s and metformin 7.93 +1.69, there was a greater improvement with DPP4i 7.86 + 1.92 at end point [2,10]. Gillani et al. (2022) and Del Prato et al. (2014) found that HBA1c was reduced with SU’s but noted a greater reduction with DPP4i and metformin over 24 and 104 weeks. 6.73 -2.65 metformin and SU, versus 6.22- 2.07 with metformin and DPP4i, a 0.72% mean change for DDP4i, versus 0.59%, for metformin and SU respectively.
One of the eight studies by Muskiet et al. (2020) found similar reductions for DPP4i linagliptin and SU glimepiride across both groups - 0.10% and -0.09% respectively from baseline to endpoint assessment after 8 weeks.
Sulfonylurea and Metformin Versus Sglt2i and Metformin
Four of the Eight studies Hollander et al. (2017), Leiter et al. (2015) Nauck et al and Nauck et al. (2011), assessed SGLT2i’s. Two of which, by Hollander et al. (2017) and Leiter et al. (2015) concurred that there was a sharp fall in HbA1c with SU at 6 -18 weeks. Both SGLT2i’s, ertugliflozin and canagliflozin, demonstrated an advantage in results over SU’s. Hollander et al. (2017) showed a reduction of -1.2 for ertugliflozin and metformin, versus -0.7 glimepiride and metformin. The results for Leiter et al. (2015) showed a reduction of -1.39 SGLT2i and metformin, versus metformin and SU -0.55. Both trials established non-inferiority between SGLT2i and SU [14,8].
Nauck et al. (2011) and Nauck et al. (2014) assessed SU versus SGLT2i, and found that glipizide had an earlier reduction in HbA1c in from baseline to week 18. At week 52, Nauck et al. (2011) found no difference between the groups. SU -0.52%, and SGLT2i -0.52%. However, at 104 weeks dapagliflozin showed a greater and sustained reduction in HbA1c, with a reduction of -0.32 for metformin and SGLT2i, and -0.14 for SU and metformin [13,9].
Different Combinations of Sulfonylurea with Metformin
Hassan and Abd-Allah (2015) compared different combinations of SU with metformin and found that glimepiride performed superior to gliclazide at 3months in reducing HbA1c. The results were Glimepiride and metformin 7±0.1, compared to 7.1±0 for Gliclazide and metformin [11].
The results here indicated a consensus towards sulfonylureas being effective in reducing HbA1c. All eight recorded a significant reduction from baseline.
A combined loss of -1.59 for SU and metformin, versus DPP4i and metformin -2.43 versus -2.91 for SGLT2i and metformin. However, four of the eight studies and the extension study by Nauck et al. (2011) found that HbA1c had a more rapid reduction in the early stages of the studies with SU and metformin. However, SGLT2i’s had a longer sustained lowering than SU at endpoint. Chen and Li (2019) also supported this finding in their systematic review, as SGLT2i’s were shown to be more effective over longer periods of time than SU’s and have similar effects in the short term [8,9,13-15].
Similar to SGLT2i, DPP4i also demonstrated better efficacy long term in comparison to SU. A review conducted by Deacon and Lebovitz (2016), also supports this finding. Current guidance from National Institute for Health and Care Excellence (NICE) (2022) recommends the use of SU’s as rescue therapy, and advise to review the treatment, once glucose levels are under control. This correlates with its ability to rapidly reduce HbA1c in the studies above. The evidence confirms the efficacy of sulfonylurea in reducing HbA1c but suggest DPP4i and SGLT2i are an effective alternative treatment to SU [16]. Although eight of the 11 studies agreed that SU’s reduce HbA1c, there were some limitations in their design. Of the eight, seven studies Muskiet et al. (2020), Hollander et al. (2017) Hassan and Abd-Allah (2015, Leiter et al. (2015), Del Prato et al. (2014), Nauck et al. (2014) and Nauck et al. (2011) used a randomised control trial design (RCT). One study by Gillani et al. (2022) used a cohort study design. Using a Robust RCT design, enhances the validity of the results by providing a rigorous tool to test relationships between intervention, the design reduces the play of external factors influencing the outcome [4,9,11,10,13,14,18].
Muskiet et al. (2020) and Hassan and Abd-Allah (2015) used small sample sizes N=46 and N=180 respectively. Both studies also used short study periods, Muskiet et al. (2020) only eight weeks, and Abd-Allah (2015) assessed outcome at 3 months. Additionally, the sample only included males, meaning that the sample was not representative, which limits the generalisations that can be made from the results. Larger sample sizes and longer study periods could have been utilised to increase the validity and reliability [11,17]. The study by Gillani et al. (2022) may have introduced bias, as there was no mention of dosage of each medication used. Potentially, the interventions may have been different which could have introduced performance bias. Additionally, confounders may have had a role to play, as compliance with trial medication may have affected the results [4].
Theme Three - Changes in Body Weight
Of the eleven studies, seven by Gillani et al. (2022), Muskiet et al. (2020), Hollander et al [4,14,17]. Assessed body mass/weight in 8,745 participants. All established that SU and metformin combination was associated with weight gain [8,9,10,13].
Metformin and Su Combination
All seven studies established that SU and metformin combination was associated with weight gain. Gillani et al. (2022) found an increase of + 0.87kg, Muskiet et al. (2020) +0.8 increase with glimepiride, Hollander et al. (2017) + 0.9kg with glipizide, Leiter et al. (2015) + 0.8kg with glimepiride, Del Prato et al. (2014) + 0.95 kg for glipizide, Nauck et al. (2014) and Nauck et al. (2011) found a 1.4kg increase glipizide. A combined weight gain of 5.72kg for SU and metformin [4,8,13,17].
Metformin and DPP4i
Of the seven studies, three compared SU and metformin to DPP4i. All 3 studies concurred that DPP4i was linked to weight loss. Gillani et al. (2022) found a -2.2kg weight loss with DPP4i, Muskiet et al. (2020) a 0.5kg weight loss with Linagliptin and Del Prato et al. (2014) -0.68 and -0.89 loss with Alogliptin. A combined weight loss of -4.27kg for DPP4i [4,17].
Metformin and SGLT2i
Four of the seven studies measuring weight/body mass, assessed the performance of SU’s and metformin against SGLT2i. Hollander et al. (2017) found in the two ertugliflozin groups, a loss of - 3.4kg and -3.0kg. Leiter et al. (2015) found a loss of 3.6kg and 3.6kg in both canagliflozin groups. Nauck et al. (2014) and Nauck et al. (2011) demonstrated a -3.4kg and -3.7kg at the end of the studies [14,8,9,13].
A combined loss of -20.7kg. Here, all seven studies agreed that SU’s are associated with weight gain, with a combined weight gain of over 5.72kg. In contrast, SGLT2i’ and DPP4i’s showed significant weight reduction versus SU, -20.7kg and 4.27kg respectively. Overall SGLT2i’s provided a greater weight reduction than DPP4i’s. The findings are parallel to those of a systematic review and meta-analysis by Storgaard et al. (2016). They concluded that SGLT2i’s had a greater weight loss when compared to DPP4i and Sulfonylurea. In their study, sulfonylurea was also shown to cause increased weight gain. Storgaard et al. (2016) suggests SGLT2’s is a safe and effective alternative to SU’s, and that the reduction in body weight, lipid profiles and systolic blood pressure identified from the findings, may have a positive impact on the reduction of cardiovascular risk [18].
Gillani et al. (2022), included only newly diabetic patients, this means patients with more advanced disease were excluded [4]. This limits the generalisations that could be made from the results and indicates potential selection bias. Including patients with different stages of the disease would have increased the representativeness of the sample. Hollander et al. (2017) and Del Prato et al. (2014) performed a power calculation, which was met, thus adding validity to the study. In contrast, Leiter et al. (2015) did not. A power calculation would ensure enough participants were enrolled to see a true effect [14,10,8].
Seven of the studies by Gillani et al. (2022), Muskiet et al. (2020), Hollander et al. (2017), Leiter et al. (2015), Del Prato et al. (2014), Nauck et al. (2014) and Nauck et al. (2011) did not monitor the participants calorie intake or diet which could have impacted the outcomes [4,17,14,8,10,9,13]. Nauck et al. (2014) Nauck et al. (2011) conducted the studies internationally, including 16 UK centres, making the results more applicable and increases generalisability [9,19].
Conclusion
Whilst metformin and sulfonylureas remain an effective second line treatment option for type 2 diabetes by reducing HbA1c levels. The review emphasized that SU’s are associated with weight gain, and cardiovascular risk remains unclear. SGLT2i’s are concomitant with a reduction in body weight, with a more sustained lowering of HbA1c over time and blood pressure lowering. SGLT2i’s are a safe and effective alternative to SU as they may provide cardiovascular protection. An individualised holistic assessment of patients should be carried out to determine the cardiovascular risk, and regular reviews of antidiabetic medication should be carried out to ensure they are updated to suit the patient’s needs. More robust research is needed to further examine combination oral antidiabetic treatments and cardiovascular risk, as there was a high level of heterogeneity (I2) and bias between the studies [20-30].
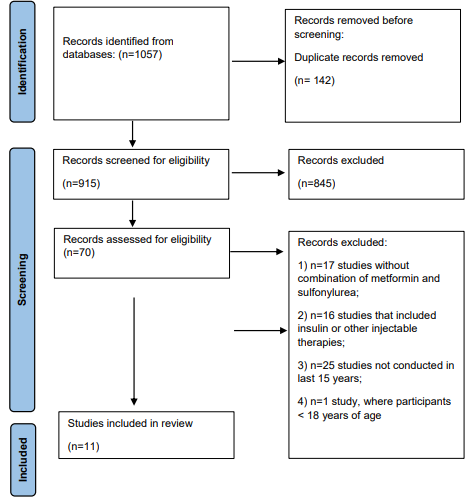
Figure 1: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. 2021.
The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71
Table 1: Characteristics of included studies
|
Study Number |
Author/ Year |
Study Design |
Participants/ Location/ sample age range |
Intervention |
Clinical Outcomes |
Results |
|
1 |
Gillani et.al, |
Prospective |
-N= 1657 |
Over 24 months (2 years) |
Increased body weight: metformin |
Increased body weight: |
|
|
2022 |
multicentre, |
-New diagnosis T2DM |
3monthly f/u centres |
+ gliclazide =0.87 increase, |
metformin + gliclazide |
|
|
|
observational cohort |
less than 5 years. |
monitored by research |
metformin + saxagliptin = 2.2 |
=0.87 increase, metformin |
|
|
|
study. |
-age > 18 years - |
team. Baseline Measures: |
decrease. |
+ saxagliptin = 2.2 |
|
|
|
|
No other serious |
lipid profile, renal |
ASCVD: differences from baseline |
decrease. |
|
|
|
|
comorbidities -5 |
function, risk ASCVD, |
to end of trial significant mean |
ASCVD: differences from |
|
|
|
|
different primary or |
glucose profile, BMI, BP |
reduction -1.1% 95% CI: -1.69 to |
baseline to end of trial |
|
|
|
|
tertiary healthcare |
then 3monthly N=513 G1 |
0.89, p = 0.041 ASCVD risk for |
significant mean reduction |
|
|
|
|
centres Penang, |
metformin, |
Su’s combined. Significant mean |
-1.1% 95% CI: -1.69 to |
|
|
|
|
Malaysia. - Above |
N=217, G2 metformin + |
reduction -1.56% 95% CI: -2.18 to |
0.89, p = 0.041 ASCVD |
|
|
|
|
6 mmol and Hb1Ac |
glimepiride N=231, G3 |
1.02 risk score for DPP4i combined. |
risk for Su’s combined. |
|
|
|
|
above |
metformin + gliclazide |
-Hospitalisation: significantly |
Significant mean reduction |
|
|
|
|
6% |
N=384, G4 metformin |
higher frequency of hospitalization |
-1.56% 95% CI: -2.18 to |
|
|
|
|
|
+sitagliptin N= 312, G5 |
from -Hba1c SU+ met =6.732.65, |
1.02 risk score for DPP4i |
|
|
|
|
|
metformin+ saxagliptin |
DPP4i+ met =6.222.07 |
combined. -Hospitalisation: |
|
|
|
|
|
DPP4i or SU |
-Hyperglycaemia metformin alone |
significantly higher |
|
|
|
|
|
|
78.16% and 30.8% SU 70.1% and |
frequency of hospitalization |
|
|
|
|
|
|
28.3%, and DPP-4 56.6% + 20.4% |
from -Hba1c SU+ met |
|
|
|
|
|
|
Hypoglycaemia SU + metformin |
=6.732.65, DPP4i+ met |
|
|
|
|
|
|
294 (65.6) Vs DPP4i + metformin |
=6.222.07 -Hyperglycaemia |
|
|
|
|
|
|
259 (37.2) |
metformin alone 78.16% |
|
|
|
|
|
|
HBA1c 6.73 – 2.65 SU+met |
and 30.8% SU 70.1% and |
|
|
|
|
|
|
6.22 -2.07DPP4i +met |
28.3%, and DPP-4 56.6% |
|
|
|
|
|
|
|
+ 20.4% |
|
|
|
|
|
|
|
Hypoglycaemia SU + |
|
|
|
|
|
|
|
metformin 294 (65.6) Vs |
|
|
|
|
|
|
|
DPP4i + metformin 259 |
|
|
|
|
|
|
|
(37.2) |
|
|
|
|
|
|
|
HBA1c 6.73 – 2.65 |
|
|
|
|
|
|
|
SU+met |
|
|
|
|
|
|
|
6.22 -2.07DPP4i +met |
|
2 |
Wanga, Wua and |
Cohort study |
N=68,591 aged >20 |
Compared DPP4i |
-Primary outcome: hospitalisation |
DPP4i more effective |
|
|
Chiena, (2021) |
|
years Taiwanese |
vs SU for Major Adverse |
for MACE’s -Secondary outcome: |
protective results than |
|
|
|
|
Insurance health data |
Cardiovascular Events |
hospitalisation for, MI, CVA, HF & |
Sulfonylurea for MACE, |
|
|
|
|
|
(MACEs) From health |
hospitalisation for hypoglycaemia. |
HF, acute MI, CVD, and |
|
|
|
|
|
claims on a national |
Comparison of SU &, DPP4i: |
hypoglycaemia. DPP4i |
|
|
|
|
|
insurance database - |
DPP4i Significantly reduced |
shows cardioprotective |
|
|
|
|
|
Patients who received |
hospitalisation risk for |
effects with +/-hx of CVD. |
|
|
|
|
|
metformin + DPP4i and |
MACE Hazard ratio (HR) adjusted |
Sitagliptin +vildagliptin |
|
|
|
|
|
metformin + SU. |
IRR 0.80 0.770.83 |
superior cardioprotective |
|
|
|
|
|
2yr 3month period |
(HF) HR 0.86 DPP4i, versus |
effect. saxagliptin may |
|
|
|
|
|
|
1.0 SU. Cerebrovascular disease |
increase risk of HF. |
|
|
|
|
|
|
HR 0.72 versus 1.0 Myocardial |
Compared SU, all 3 |
|
|
|
|
|
|
Infarction (MI), DPP4i= 340, HR |
DPP4i’s lowered the risk of |
|
|
|
|
|
|
1.0, versus SU =402, HR 0.84. |
hypoglycaemia in patients |
|
|
|
|
|
|
hypoglycaemia HR 0.46 0.41-0.52 |
T2DM |
|
|
|
|
|
|
Large reduction risk of |
|
|
|
|
|
|
|
hospitalisation for MACE |
|
|
|
|
|
|
|
Sitagliptin = 0.89 0.850.94 |
|
|
|
|
|
|
|
vildagliptin =0.77 0.60-0.99. |
|
|
|
|
|
|
|
saxagliptin borderline meaningful |
|
|
|
|
|
|
|
higher risk of |
|
|
|
|
|
|
|
HF |
|
|
3 |
Muskiet, et.al, |
Double-blind RCT |
DPP-4i Linagliptin vs |
Linagliptin 5mg vs |
GFR=Linagliptin- no effect from |
Renal function not affected |
|
|
2020 RENALIS |
|
sulfonylurea on renal |
glimepiride 1mg for 8 |
baseline ERPF= Linagliptin- no |
by linagliptin. Linagliptin |
|
|
|
|
functioning |
weeks. (GFR) effective |
effect from baseline - HBA1c= |
increased vs glimepiride |
|
|
|
|
in T2DM patients |
renal plasma flow (ERPF) |
reductions similar: Glimepiride |
patients. |
|
|
|
|
already on metformin |
determined by Fractional |
–0.65 6 0.10%. |
-DPP-4 inhibition promotes |
|
|
|
|
-46 overweight T2DM |
excretions, urinary |
-Linagliptin mean 6 SEM – 0.45 |
Na excretion |
|
|
|
|
Caucasian, women |
damage markers, inulin, |
6 0.09% -BMI: glimepiride vs |
-SU associated with |
|
|
|
|
and men aged 35 to 75 |
-and paraMino hippuric |
linagliptin caused increased body |
increased weight gain and |
|
|
|
|
years, on metformin |
acid clearance, glucagon- |
weight |
more hypoglycaemic events |
|
|
|
|
alone HbA1c 6.5–9.0, |
like peptide 1SC derived |
+0.8 kg, -0.5kg for DPP4i. BP & |
|
|
|
|
|
BMI >25kg |
factor-1α and DPP4i |
HR - No changes noted for heart |
|
|
|
|
|
|
substrata |
rate and BP |
|
|
|
|
|
|
|
-Fractional excretion of sodium was |
|
|
|
|
|
|
|
increased with |
|
|
|
|
|
|
|
linagliptin |
|
|
|
|
|
|
|
Hypoglycaemia: Linagliptin 4% vs |
|
|
|
|
|
|
|
25% Glimepiride |
|
|
4 |
Douros et. al, |
Cohort study |
N=47,184 Patients |
Does adding or switching |
25,699 added or switched to SU |
SU alone linked with a |
|
|
2018 |
|
T2DM started on |
to SU increases risk |
Mean f/u 1.1 years. SU linked to |
higher risk of MI, severe |
|
|
|
|
metformin alone |
severe hypoglycaemia |
higher risk of MI =incidence 7.8 v |
hypoglycaemia, and |
|
|
|
|
between 1998 - 2013. |
ischaemic stroke, MI, |
6.2, HR 1.26, 95% CI 1.01 - 1.56 |
mortality, vs staying on |
|
|
|
|
UK CPRD database |
cardiovascular death, |
-Mortality= 27.3 v 21.5, 1.281.15 |
metformin alone. When |
|
|
|
|
|
mortality vs remaining |
- 1.44. -Hypoglycaemia= 0.7 v 5.5, |
introducing SU it is safer |
|
|
|
|
|
on metformin alone for |
7.60, 4.64 to 12.44 vs remaining on |
to add metformin than to |
|
|
|
|
|
second line treatment SU |
metformin only. |
switch |
|
|
|
|
|
N=23, 592 Metformin |
-Increased risk of cardiovascular |
|
|
|
|
|
|
N=23, 592 |
death 8.1 v 9.4, 1.18, 0.98 - 1.43. |
|
|
|
|
|
|
|
and stroke 6.7 v 5.5, 1.24 0.99 - |
|
|
|
|
|
|
|
1.56 Vs adding SU. switching to |
|
|
|
|
|
|
|
SU concomitant with higher risk |
|
|
|
|
|
|
|
of MI HR 1.51, 95% CI 1.03 - 2.24 |
|
|
|
|
|
|
|
and mortality 1.23, 1.00 - 1.50. |
|
|
|
|
|
|
|
No difference for, cardiovascular |
|
|
|
|
|
|
|
death ischaemic stroke, or severe |
|
|
|
|
|
|
|
hypoglycaemia adding SU= N39, |
|
|
|
|
|
|
|
CI 95% 3.4 2.5 - 4.7 |
|
|
5 |
Study Hollander |
RCT, double blind, |
N =1325,18+ years + |
-Measure effects and |
Participants were similar, a |
-More SAEs in ertugliflozin |
|
|
et. al, 2017 |
Non- inferiority |
T2DM |
safety of glimepiride |
minimum of 1 AE through the |
groups not considered |
|
|
VERTIS |
trial Phase 3 |
232 sites, 16 countries: |
compared with |
groups. Trial drug related AEs = |
related to medication |
|
|
|
|
Taiwan, |
ertugliflozin. Patients |
GMI. SAE’s in ertugliflozin 5mg |
- Safety for use of |
|
|
|
|
Canada, |
with T2DM - Poor |
group higher vs glimepiride and |
ertugliflozin acceptable |
|
|
|
|
Republic, Poland, |
control on metformin |
ertugliflozin 15mg. - Spread across |
- non-inferiority of |
|
|
|
|
South Korea, Hungary, |
-Over 104 weeks. First 52 |
classes, 2 Pneumonia: |
Ertugliflozin 15 mg + |
|
|
|
|
Argentina, Mexico, |
weeks (A phase) |
Ertugliflozin 5mg N=2 Glimepiride |
metformin to glimepiride |
|
|
|
|
Lithuania, Romania, |
Second 52 weeks (B |
N=1 |
confirmed inHbA1c |
|
|
|
|
Slovakia, South Africa, |
phase) to measure long- |
CVA: ertugliflozin 5mg N= 2 |
reduction. - Ertugliflozin |
|
|
|
|
Czech, Ukraine, USA, |
term effectiveness and of |
compared to glimepiride N=1 |
provides, better weight |
|
|
|
|
Philippines, Russia, |
ertugliflozin |
AE’s resulting in discontinuation |
loss, glucose control, and |
|
|
|
|
|
-HbA1c between 7 and 9 |
across groups. 7 deaths: glimepiride |
lowering BP relative to |
|
|
|
|
|
percent, taking metformin |
N=1 ertugliflozin 15mg N=1, |
Glimepiride. -Ertugliflozin |
|
|
|
|
|
1500 mg per day to, |
ertugliflozin 5mg N=5 and |
reduced the occurrence |
|
|
|
|
|
glimepiride titrated from |
Hypoglycaemia reduced with |
of hypo, but increased |
|
|
|
|
|
1 mg, or ertugliflozin |
ertugliflozin vs with glimepiride. |
incidence of Genital |
|
|
|
|
|
15mg/5mg once daily. |
Severe hypoglycaemia reported |
mycotic infections. |
|
|
|
|
|
|
in N=1 with ertugliflozin 15mg, |
Results: Ertugliflozin |
|
|
|
|
|
|
N=1 ertugliflozin 5mg, and N=10 |
safe alternative to SU for |
|
|
|
|
|
|
glimepiride. |
insufficient glycaemic |
|
|
|
|
|
|
Weight loss -6.4 with ertugliflozin |
control on metformin. |
|
|
|
|
|
|
HBA1c – ertugliflozin 1.1mmol |
|
|
|
|
|
|
|
difference. SU greater reduction – |
|
|
|
|
|
|
|
sharp fall 6-12 weeks |
|
|
6 |
Chang et. al, |
Retrospective |
N=36,118 Taiwanese, |
-Hospitalisations for any |
-ITT analysis results: No variance in |
-No alteration to overall |
|
|
(2015) |
cohort study |
National |
cardiovascular event: |
risk of cardiovascular events across |
cardiovascular risk linked |
|
|
|
|
Health Insurance |
MI, ischaemic stroke |
treatment groups. -Significantly |
with sulfonylureas vs other |
|
|
|
|
database |
congestive cardiac |
reduced |
second-line agents. |
|
|
|
|
1 year study |
failure (CCF) and - Over |
risk of acute MI found in glinides |
- Potentially lower risk |
|
|
|
|
|
1 year until outcome, |
and metformin group, crude HR |
of MI with glinides + |
|
|
|
|
|
death, or disenrollment. |
0.52 Adjusted HR 0.39; 95% CI |
metformin compared with |
|
|
|
|
|
5 categories: metformin, |
0.20 to 0.75 and -A- glucosidase- I |
sulfonylureas +metformin |
|
|
|
|
|
Aglucosidase inhibitors, |
+ metformin, HR (crude) |
|
|
|
|
|
|
sulfonylureas and |
0.63, |
|
|
|
|
|
|
metformin, metformin |
-Adjusted HR 0.54; 95% CI 0.31 |
|
|
|
|
|
|
and glinides, metformin |
to 0.95. |
|
|
|
|
|
|
and DPP4i and metformin |
Risk of stroke or CCF on change |
|
|
|
|
|
|
and pioglitazone |
observed |
|
|
7 |
Leiter, et.al, 2015 |
RCT Phase 3 Study |
N = 1,450) 52- weeks |
Canagliflozin 100 or |
104-week HBA1C reductions |
Canagliflozin provides |
|
|
|
|
followed by 52-week |
300 mg + Metformin Vs |
100mg -0.65%, -300mg 0.74%, and |
more reduced body weight, |
|
|
|
|
extension. 157 centres, |
N=968 |
Glimepiride -0.55% -7.1, 8.1, and |
durable |
|
|
|
|
19 countries |
Glimepiride -titrated |
-6.0 mmol. Reduced body weight |
glycaemic effect vs |
|
|
|
|
Study conducted 28 |
to 6 or 8mg daily + |
- 0.68kg, -0.89, Canagliflozin and |
Glimepiride |
|
|
|
|
August 2009 - January |
Metformin N=482 |
+0.95, Glimepiride. |
More hypoglycaemic |
|
|
|
|
2013. Age >18 and <80 |
|
SBP (-2.0 100mg -3.1 300mg and |
events and SAEs with |
|
|
|
|
years |
|
+1.7 Glimepiride. Adverse Events |
Glimepiride. |
|
|
|
|
|
|
73.3%, 100mg 77.9%, 300mg and |
AE’s similar across groups |
|
|
|
|
|
|
78.4% Glimepirides GMI, UTI, |
More UTIs and GMI’s in |
|
|
|
|
|
|
increased urination |
canagliflozin group |
|
|
|
|
|
|
related AEs increased for |
Reduce systolic BP and |
|
|
|
|
|
|
canagliflozin |
weight observed with |
|
|
|
|
|
|
vs glimepiride Hypoglycaemia |
canagliflozin versus |
|
|
|
|
|
|
significantly higher with |
glimepiride. |
|
|
|
|
|
|
Glimepiride 40.9% for canagliflozin |
Reduced eGFR observed in |
|
|
|
|
|
|
100mg 6.8 % and 300mg 8.2 % |
3 groups but was higher for |
|
|
|
|
|
|
glimepiride 6.8% reduction, in GFR |
Glimepiride |
|
|
|
|
|
|
with canagliflozin. This attenuated |
|
|
|
|
|
|
|
over the trial. SAEs =9.7%, |
|
|
|
|
|
|
|
100mg 9.7% 300mg and 14.3%, |
|
|
|
|
|
|
|
Glimepiride. |
|
|
|
|
|
|
|
Canagliflozin associated increased |
|
|
|
|
|
|
|
HDL-C 0.21 and 22, stable at 26 |
|
|
|
|
|
|
|
and remained |
|
|
8 |
Nauck et.al, |
Double blind |
52 weeks with a |
Initial 52-week study |
HbA1c mean decrease: at 52 weeks. |
Glycaemic durability |
|
|
(2014) |
multicentre RCT – |
156- week extension – |
once completed, entered |
Dapagliflozin vs glipizide changes |
significantly better over |
|
|
|
extension study |
N=814 |
longer extension |
at 104 wks −0.18% 2.0 mmol 95% |
24mnths with dapagliflozin |
|
|
|
|
DAP & Metformin = |
double-blind period. |
CI: −0.33 −3.6, −0.03−0.3. FPG |
vs glipizide, |
|
|
|
|
n 406 |
-52 additional treatment |
than decrease at 104 weeks −1.12 |
-UTIs and GMI most |
|
|
|
|
GLIP& Metformin = |
weeks One chance for |
mmol 95% CI: −1.32, −0.92, |
prevalent side effects linked |
|
|
|
|
n 408 |
up titration permitted. |
glipizide −0.68 mmol 95% CI: |
to dapagliflozin. incidence |
|
|
|
|
|
– If HbA1c was above |
−0.89, −0.47 0 deaths with |
reduced during assessment |
|
|
|
|
|
7, if not on max dose. |
dapagliflozin. 4 |
period. |
|
|
|
|
|
Down titration allowed if |
deaths with glipizide. |
-Persistent weight loss |
|
|
|
|
|
hypoglycaemia happens |
-7 cancers, across both groups |
+SBP, may provide a |
|
|
|
|
|
on more than one |
Weight: − 3.7 dapagliflozin + |
beneficial result for |
|
|
|
|
|
occasion. |
met vs + 1.4 glipizide + met |
cardiovascular risk – but no |
|
|
|
|
|
|
Hypoglycaemia less in dapagliflozin |
significant difference. |
|
|
|
|
|
|
4.2 % vs glipizide 45.8% |
|
|
|
|
|
|
|
No significant difference for |
|
|
|
|
|
|
|
cardiovascular |
|
|
|
|
|
|
|
risk between groups |
|
|
|
|
|
|
|
AA: SGLTi2+met=0 SU+met=1 |
|
|
|
|
|
|
|
MI: SGLTi2+met=1 SU+met=1 |
|
|
|
|
|
|
|
CAO: SGLTi2+met=0 SU+met=1 |
|
|
9 |
Del Prato et.al, |
RCT- Multi centre, |
N=2639 Participants |
Treatment for 104 weeks. |
Primary results: Mean HbA1c and |
Significantly increased |
|
|
(2014) |
double blind, |
aged |
N=880 metformin |
Fasting plasma glucose FPG at the |
risk of hypoglycaemia in |
|
|
|
|
18–80. |
+alogliptin 12.5mg OD |
end of 104 weeks from start 104: |
Glipizide group. Risk for |
|
|
|
|
With T2DM Research |
N=885 alogliptin25 mg |
−0.68% alogliptin 12.5 −0.59% |
MACE Cardiovascular |
|
|
|
|
sites: 310 |
OD |
glipizide and −0.72% alogliptin 25 |
death, stroke or MI and risk |
|
|
|
|
Australia, America |
N=874 Glipizide 5 mg |
mg FPG: reduced by 0.05 + 0.18 |
of pancreatitis comparable |
|
|
|
|
North + South, Europe, |
OD. Max titration of |
mmol for alogliptin 12.5/25mg, |
across the 3 groups |
|
|
|
|
South, New Zealand, |
20 mg |
glipizide increased 0.30 mmol - |
|
|
|
|
|
and South Africa |
|
Safety for MACE (cardiovascular |
|
|
|
|
|
|
|
death, Ml or stroke) alogliptin |
|
|
|
|
|
|
|
12.5mg = 6, alogliptin 25mg = 8, |
|
|
|
|
|
|
|
glipizide =11. Safety results for |
|
|
|
|
|
|
|
hypoglycaemia: |
|
|
|
|
|
|
|
Glipizide 23.2, alogliptin 25 mg |
|
|
|
|
|
|
|
1.4%, alogliptin12.5mg 2.5% Mean |
|
|
|
|
|
|
|
weight difference: −0.68, alogliptin |
|
|
|
|
|
|
|
12.5, −0.89 25mg and |
|
|
|
|
|
|
|
+0.95 glipizide. ss |
|
|
10 |
Hassan and Abd- |
RCT |
N=180 Recruited from |
Randomised 6 groups, |
HBA1c: met + gliclazide 7.1±0 Vs |
|
|
|
Allah, 2015 |
|
Alzahra Hospital, by |
N30 in each: Placebo |
glimepiride |
|
|
|
|
|
staff, Cairo, Egypt. |
Control group - calorie- |
7±0.1 from baseline change |
|
|
|
|
|
Male, age 30-75 |
restricted diet, active |
FPG reduction -26.1% gliclazide |
|
|
|
|
|
3month period T2DM |
lifestyle Gliclazide 80mg |
+ met ±3.7 vs. glimepiride + |
|
|
|
|
|
|
Metformin 500mg BD, |
met 28.9±3.1PPG gliclazide + |
|
|
|
|
|
|
Glimepiride 3 mg OD, |
Met-42.4%±3.3 vs Glimepiride |
|
|
|
|
|
|
Gliclazide + Metformin |
+ Met -46±2 HbA1C gliclazide |
|
|
|
|
|
|
or Glimepiride + |
+Met 21.1±1.5 vs. -21.3±1.6% |
|
|
|
|
|
|
Metformin |
Glimepiride +Met Gliclazide |
|
|
|
|
|
|
Outcome measures: FPG, |
or glimepiride + Met improved |
|
|
|
|
|
|
PPG, plasma glucose, |
induced disruption of Hcy. |
|
|
|
|
|
|
change in Hcy and |
glimepiride +met 10.3±0.3 |
|
|
|
|
|
|
HbA1c from 0-3mnths |
vs gliclazide + met 11±0.3 |
|
|
|
|
|
|
secondary outcomes: |
Hypoglycaemic events |
|
|
|
|
|
|
vitamin B12 level |
patients 6.6%, Gliclazide alone |
|
|
|
|
|
|
|
n=2, glimepiride alone n=2 |
|
|
|
|
|
|
|
Metformin=0, 3/30 met =gliclazide, |
|
|
|
|
|
|
|
5/30 (16.6%) met + glimepiride |
|
|
|
|
|
|
|
16.6% |
|
|
|
|
|
|
|
LDL: met + gliclazide 146±7 met + |
|
|
|
|
|
|
|
glimepiride 142±7 |
|
|
|
|
|
|
|
Cholesterol: met 235±8 212±12b |
|
|
11 |
Pantalone et. al, |
Retrospective |
N= (7320) Pts >18 yrs. |
3768 glibenclamide + |
Metformin plus glipizide or |
No identification of higher |
|
|
(2012) |
cohort study |
using academic health |
metformin |
glimepiride plus metformin: |
risk for mortality with |
|
|
|
|
centre electronic |
2277 glipizide + |
HR 1.03; 95% CI 0.89– 1.20, |
variation of metformin in |
|
|
|
|
health record system, |
metformin 1275 |
-Metformin plus glimepiride |
addition to sulfonylureas, |
|
|
|
|
Cleveland, OH, USA |
Glimepiride and |
plus versus Metformin plus |
indicating total mortality |
|
|
|
|
|
metformin, assessed for |
glibenclamide:1.08; 95% CI 0.90– |
is not significantly |
|
|
|
|
|
outcome of mortality by |
1.30, or metformin plus glipizide |
impacted by selection of |
|
|
|
|
|
Social Security Death |
vs. metformin plus glibenclamide: |
sulfonylurea. |
|
|
|
|
|
Index. |
HR 1.05; 95% CI 0.95–1.15. |
|
|
|
|
|
|
And electronic health |
636 deaths occurred in the cohort |
|
|
|
|
|
|
record |
|
|
|
|
|
|
|
From 1998 and 12 |
|
|
|
|
|
|
|
October 2006(8 years) |
|
|
|
|
|
|
|
follow up median (2.4 |
|
|
|
|
|
|
|
years) |
|
|
References
- Holt, R.I.G., Cockram, C.S., Flyvbjerg, A., Goldstein, B.J. (2017) Textbook of Diabetes. 5th ed. [online]. John Wiley & Sons, Ltd. Available at: ProQuest Ebook Central - Reader [Accessed: 28 December, 2022].
- Valaiyapathi, B., Gower, B., & Ashraf, A. P. (2020). Pathophysiology of type 2 diabetes in children and adolescents. Current diabetes reviews, 16(3), 220-229.
- Ghosh, S., & Collier, A. (2012). Churchill's Pocketbook of Diabetes E-Book. Elsevier Health Sciences.
- Gillani, S.W., Sulaiman, S.A.S., Menon, V., Rahamathullah,I. N., Elshafie, R.M., Rathore H.A. (2022) Effect of different antidiabetic medications on atherosclerotic cardiovascular disease (ASCVD) risk score among patients with type-2 diabetes mellitus: A multicentre noninterventional observational study. Public Online Journal of Science, 17(6), 1-15
- Wanga, J., Wua, H.Y., Chiena, K.L. (2021) Cardioprotective effects of dipeptidyl peptidase-4 inhibitors versus sulfonylureas in addition to metformin: A nationwide cohort study of patients with type 2 diabetes. Diabetes & Metabolism, 48(3), 1-9
- Douros, A., Dell’ Aniello, S., Hoi Yun Yu, O., Filion, K., Azoulay. L., Suissa, S. (2018) Sulfonylureas as second line drugs in type 2 diabetes and the risk of cardiovascular and hypoglycaemic events: population-based cohort study. British Medical Journal 36(2), 1-9
- Chang, Y.C., Chuang, L.M., Lin, J.W., Chen. S.T., Lai, M.S., Chang, C.H. (2015) Cardiovascular risks associated with second-line oral antidiabetic agents added to metformin in patients with Type 2 diabetes: a nationwide cohort study, Diabetic Medicine, 32(11), 1397-1528
- Leiter, L., Yoon, K.H., Arias, P., Langslet, G., Xie, J., Balis, D.A., Millington, D., Vercruysse, F., Canovatchel, W., Meininger, G. (2015) Canagliflozin Provides Durable Glycaemic Improvements and Body Weight Reduction Over 104 Weeks Versus Glimepiride in Patients with Type 2 Diabetes on Metformin: A Randomized, DoubleBlind, Phase 3 Study Diabetes Care, 38(3), 355–364
- Nauck, M.A., Del Prato, S., Duran-Garcia, S., Rohwedder, K., Langkilde A.M., Sugg., Parikh, S.J. (2014) Durability of glycaemic efficacy over 2 years with dapagliflozin versus glipizide as add-on therapies in patients whose type 2 diabetes mellitus is inadequately controlled with metformin. Diabetes, Obesity and Metabolism, 16(11)
- Del Prato, S., Camisasca, R., Wilson, C., Fleck, P. (2014) Durability of the efficacy and safety of Alogliptin compared with glipizide in type 2 diabetes mellitus: a 2-year study. Diabetes, Obesity and Metabolism, 16(12), 1239–124
- Hassan, M.H., Abd-Allah, G.M. (2015) Effects of metformin plus gliclazide versus metformin plus glimepiride on cardiovascular risk factors in patients with type 2 diabetes mellitus. Pakistan Journal of Pharmaceutical Sciences, 49(1), 60-74
- Pantalone, K.M., Kattan. M.W., Yu, C., Wells, B. J., Arrigain, S., Nutter, B., Jain, Atreja, A.A., Zimmerman, R.S. (2012) Treatment The risk of overall mortality in patients with Type 2 diabetes receiving different combinations of sulfonylureas and metformin: a retrospective analysis. Journal of Diabetic Medicine, 29(8), 1029-1035
- Nauck, M.A., Del Prato, S., Meier, J.J., Duran- Garcia, S., Rohwedder, K., Elze, M., Parikh, S.J. (2011) Dapagliflozin Versus Glipizide as Add-on Therapy in Patients with Type 2 Diabetes Who Have Inadequate Glycaemic Control With Metformin A randomized, 52-week, double-blind, active-controlled noninferiority trial. Diabetes, Obesity and Metabolism, 34(9), 2015–2022
- Hollander, P., Liu, J., Hill, J., Johnson, J., Jiang. J.W., Golm.G., Huyck, S., Terra, S.G., Mancuso, J.P., Engel, S.S, Laurin,B. (2017) Ertugliflozin Compared with Glimepiride in Patients with Type 2 Diabetes Mellitus Inadequately Controlled on Metformin: The VERTIS SU Randomized Study. Diabetes Therapy, 9,193–207
- Chen, Z., & Li, G. (2019). Sodium-glucose co-transporter 2 inhibitors compared with sulfonylureas in patients with type 2 diabetes inadequately controlled on metformin: a meta-analysis of randomized controlled trials. Clinical drug investigation, 39, 521-531.
- Deacon, C.F., Lebovitz, H.E. (2016) Comparative review of dipeptidyl peptidase-4 inhibitors and sulfonylureas. Diabetes, Obesity and Metabolism, 18(4) 334-347
- Muskiet , M.H.A., Tonneijck, L., Smits, M.M., Kramer, M.H.H., Ouwens, D.M., Hartmann, B., Holst, J.J., Touw, D.J., Danser, H.J., Joles, J.A., Van Raalte, D.H. (2020) Effects of DPP-4 Inhibitor Linagliptin Versus Sulfonylurea Glimepiride as Add-on to Metformin on Renal Physiology in Overweight Patients With Type 2 Diabetes (RENALIS): A Randomized, Double-Blind Trial. Diabetes Care, 43(11), 2889–2893
- Storgaard, H., Gluud, L.L., Bennett, C., Grøndahl, M.F., Christensen, M.B., Knop, F.K., Vilsbøll, T. (2016) Benefits and Harms of Sodium-Glucose Co-Transporter 2 Inhibitors in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Public Library of Science ONE, 11(11), 1-23
- Chen, Y.Y., Lin, Y.L., Chong1, E. Chen, P.C., Chao, T.F., Chen, S.A., Chien, K.L. (2015) The Impact of Diabetes Mellitus and Corresponding HbA1c Levels on the Future Risks of Cardiovascular Disease and Mortality: A Representative Cohort Study in Taiwan. PLOS one, 10(4), 1-12
- A Meta-Analysis of Randomized Controlled Trials. Clinical Drug Investigation
- Critical Appraisal Skills Programme (2020) CASP (Randomised Controlled Trial and Cohort Study) Checklist.
- Diabetes UK (2019) Tackling the crisis: Transforming diabetes care for a better future England.
- Diabetes.co.uk (2022) Insulin
- Hariton, E., Locascio, J.J. (2018) Randomised controlled trials—the gold standard for effectiveness research. British journal of obstetrics and gynaecology, 125(13), 1-3
- National Institute for Health and Care Excellence (NICE).(2022) How to choose medicines for further treatment.
- National Institute for Health and Care Excellence (NICE). (2015) Putting NICE guidance into practice: Resource impact report: Type 2 diabetes in adults: management (update) NICE.
- National Health Service (NHS). (2020) Understanding Medicine: Type 2 diabetes.
- PRISMA. (2020) PRISMA 2020 Checklist.
- Training, Research and Education for Nurses in Diabetes (TREND). (2022) For Healthcare Professionals: An Integrated Career and Competency Framework for Adult Diabetes Nursing. TREND. 6th ed.
- World Health Organization (WHO). (2022) Diabetes: key