



Research Article - (2019) Volume 4, Issue 2
Spironolactone Versus Eplerenone as Adjunctive Treatment in Patients with Heart Failure
Received Date: May 13, 2019 / Accepted Date: May 25, 2019 / Published Date: May 28, 2019
Copyright: ©Mohammad A K Hasan. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: The goals of treatment in patients with heart failure (HF) are to improve their clinical status, functional capacity, and quality of life, prevent hospital admission and reduce mortality.
Aim of the work: This work aims to evaluate spironolactone versus eplerenone as an adjunctive therapy regarding tolerability in patients with HF (NYHA II to IV) already on anti-failure treatment with beta Blockers (BB) and/or ivabradine and their effect on major adverse cardiac events.
Study design: 100 patients were recruited and randomized into 2 groups (n=50/group); group 1 received spironolactone 25mg/d that was titrated to 100mg/d if tolerated, while group 2 received eplerenone 25mg/d that was titrated to 50mg/d if tolerated. Follow up of: symptoms, signs, potassium level, BNP, renal functions, systolic function and side effects was done over 3 months in 3 visits.
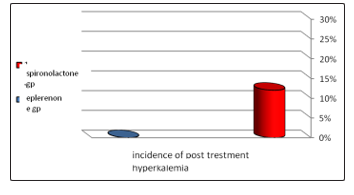
Results: After 3 months it was found that 39 patients (78%) in each group showed good or marked improvement, with non significant P-value. Regarding side effects, the spironolactone group showed incidence of hyperkalemia in 6 patients (12%) in the spironolactone group; with 0% incidence in the other group with significant P-value (P<0.001). On the other hand 5 patients (10%) had gynecomastia in the spironolactone group with 0% incidence in the eplerenone group with significant P-value (P<0.001).
Conclusion: spironolactone and eplerenone are both effective but the eplerenone is much more safer than spironolactone when added as an adjunctive therapy in patients with HF and are kept on full medical therapy including BBs.
Keywords
BNP level, Gynecomastia, NYHA, Potassium
Introduction
Heart Failure (HF) is a clinical syndrome characterized by typical symptoms (e.g. breathlessness, ankle swelling and fatigue) that may be accompanied by signs (e.g. elevated jugular venous pressure, pulmonary crackles and peripheral edema) caused by a structural and/or functional cardiac abnormality, resulting in a reduced cardiac output and/or elevated intracardiac pressures at rest or during stress [1,2].
HF comprises a wide range of patients, from those with normal LVEF [typically considered as ≥50%; HF with preserved EF (HFpEF)] to those with reduced LVEF [typically considered as <40%; HF with reduced EF (HFrEF)] [3].
Over the last 30 years, improvements in treatments and their implementation have improved survival and reduced the hospitalization rate in patients with HFrEF, although the outcome often remains unsatisfactory [4].
The plasma concentration of natriuretic peptides (NPs) can be used as an initial diagnostic test [5,6]. Echocardiography is the most useful, widely available test in patients with suspected HF to establish the diagnosis [7-16].
Treatment of Heart failure
The goals of treatment in patients with HF are to improve their clinical status, functional capacity and quality of life, prevent hospital admission and reduce mortality.
The treatment of HFrEF is though one of the following:
a) pharmacological treatment
b) non surgical device implantation
c) surgical device implantation
d) Heart transplantation
The pharmacological treatment is the main line of treatment which showed great innovations over the last decades, it includes:
1. Angiotensin converting enzyme inhibitors (ACEIs
2. Beta- Blockers (BBs)
3. Mineralocorticoid/aldosterone receptor antagonists (MRAs)
4. Diuretics
5. Angiotensin receptor neprilysin inhibitor (ARNI)
6. If channel inhibitors
7. Angiotensin II type I receptor blockers (ARBs)
8. Combination of hydralazine and isosorbide dinitrate
9. Digoxin
Our study is the first head to head trial between spironolactone and eplerenone. All previous studies compare the efficacy or safety of one of them against placebo.
Methods
In this study 100 patients attending Egypt Air hospital clinic were recruited and randomized into 2 groups in a single blinded manner as follows:
Group 1: contains 50 patients with their year of birth an odd number and they were subjected to spironolactone treatment.
Group 2: contains 50 patients with their year of birth an even number and they were subjected to eplerenone treatment.
The study duration was 3 months including 3 visits. All patients must have known to be a chronic heart failure patient with NYHA class II to IV with symptoms and/or signs of HF and are maintained on stable doses of medical treatment over the last 6 months with normal renal functions.
Group 1 received spironolactone 25 mg in visit 1 which was titrated if tolerated up to 100mg over the following visits while group 2 received eplerenone 25 mg in visit 1 which was titrated if tolerated up to 50 mg over the following visits.
Follow up of BNP, serum creatinine, serum potassium and echocardiography for EF% and myocardial mass was done for both groups.
Results
1. There was improvement in the EF% in both groups post treatment with no significant P value between them.
2. There was significant reduction in myocardial mass in both groups post treatment with non significant difference between the 2 groups.
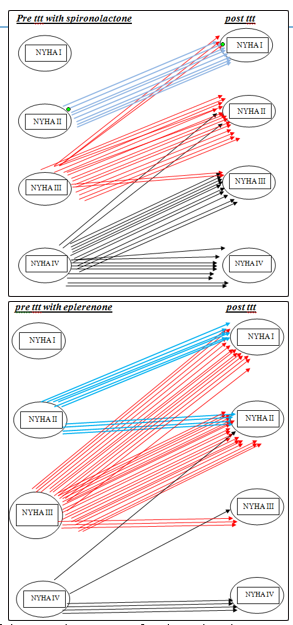
3. There was significant improvement in NYHA class in both groups with more improvement in the eplerenone group
4. Eplerenone shows more safety than spironolactone regarding side effects
(a) Incidence of post treatment hyperkalemia was more in the spironolactone group.
(b) Post treatment gynecomastia was only reported in the spironolactone group
|
Groups |
Incidence of post treatment gynecomastia |
|
|
Group I |
N |
5(10%) |
|
Group I I |
N |
(0%) |
|
P-value |
|
<0.001* |
Discussion
This study is the first head to head study for spironolactone versus eplerenone.
Many studies were done to evaluate adding spironolactone; RALES study, or eplerenone; EPHESUS and REMODEL studies showing their effect on hospitalization, remodeling and mortality.
In Rales study, it was found that blockade of aldosterone receptors by spironolactone, in addition to standard therapy, substantially reduces the risk of both morbidity and death among patients with severe heart failure.
EPHESUS study, studied the incidence of hyperkalemia in eplerenone treated patients versus placebo which showed non significant possibility of hyperkalemia in the eplerenone treated patients.
Our study told us that spironolactone and eplerenone are both effective with more efficacy towards the eplerenone also the eplerenone is much more safer than spironolactone when add as an adjunctive therapy in patients with HF and are kept on full medical therapy including BBs
Conclusion
We found that both spironolactone and eplerenone are effective as an adjunctive therapy with more effectiveness in the eplerenone group with much less side effects in that group.
This results in improved morbidity and clinical outcome as documented by improvements in NYHA class, BNP levels and myocardial mass with less incidence of gynecomastia and hyperkalemia in the eplerenone group.
References
- Wang TJ (2003) Natural history of asymptomatic left ventricular systolic dysfunction in the community. Circulation 108: 977- 982.
- The SOLVD Investigators (1992) Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. N Engl J Med 327: 685 - 691.
- Butler J, Fonarow GC, Zile MR, Lam CS, Roessig L, et al. (2014) Developing therapies for heart failure with preserved ejection fraction: current state and future directions. JACC Heart Fail 2: 97-112.
- Maggioni AP, Dahlström U, Filippatos G, Chioncel O, Crespo Leiro M, et al. (2013) EURObservational Research Programme: regional differences and 1-year follow-up results of the Heart Failure Pilot Survey (ESC-HF Pilot). Eur J Heart Fail 15: 808- 817.
- Roberts E, Ludman AJ, Dworzynski K, Al-Mohammad A, Cowie MR, et al. (2015) The diagnostic accuracy of the natriuretic peptides in heart failure: systematic review and diagnostic meta-analysis in the acute care setting. BMJ 350: h910.
- Maisel A, Mueller C, Adams K, Anker SD, Aspromonte N, et al. (2008) State of the art: using natriuretic peptide levels in clinical practice. Eur J Heart Fail 10: 824-839.
- Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, et al. (2007) How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J 28: 2539-2550.
- Marwick TH, Raman SV, Carrió I, Bax JJ (2010) Recent developments in heart failure imaging. JACC Cardiovasc Imaging 3: 429-439.
- Dokainish H, Nguyen JS, Bobek J, Rajiv Goswami Nasser M. Lakkis (2011) Assessment of the American Society of Echocardiography-European Association of Echocardiography guidelines for diastolic function in patients with depressed ejection fraction: an echocardiographic and invasive haemodynamic study. Eur J Echocardiogr 12: 857-864.
- Kirkpatrick JN, Vannan MA, Narula J, Lang RM (2007) Echocardiography in heart failure: applications, utility, and new horizons. J Am Coll Cardiol 50: 381-396.
- Nagueh SF, Bhatt R, Vivo RP, Krim SR, Sarvari SI et al. (2011) Echocardiographic evaluation of hemodynamics in patients with decompensated systolic heart failure. Circ Cardiovasc Imaging 4: 220-227.
- Caballero L, Kou S, Dulgheru R, Gonjilashvili N, Athanassopoulos GD, et al. (2015) Echocardiographic reference ranges for normal cardiac Doppler data: results from the NORRE Study. Eur Heart J Cardiovasc Imaging 16: 1031-1041.
- Garbi M, McDonagh T, Cosyns B, Bucciarelli-Ducci C, Edvardsen T, et al. (2015) Appropriateness criteria for cardiovascular imaging use in heart failure: report of literature review. Eur Heart J Cardiovasc Imaging 16: 147-153.
- Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, et al. (2015) Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 16: 233-270.
- Gimelli A, Lancellotti P, Badano LP, Lombardi M, Gerber B, et al. (2014) Non-invasive cardiac imaging evaluation of patients with chronic systolic heart failure: a report from the European Association of Cardiovascular Imaging (EACVI). Eur Heart J 35: 3417-3425.
- Voigt J-U, Pedrizzetti G, Lysyansky P, Marwick TH, Houle H, et al. (2015) Definitions for a common standard for 2D speckle tracking echocardiography: consensus document of the EACVI/ ASE/Industry Task Force to standardize deformation imaging. Eur Heart J Cardiovasc Imaging 16: 1- 11.