
Journal of ENT Surgery Research(JESR)

Case Report - (2023) Volume 1, Issue 1
Rhinoscleroma- the Recalcitrant and Indolent Entity: A Case Report
2Professor & Head, Department of ENT and Head-Neck Surgery, Sri Guru Ram Rai, Institute of Medical and Health Sciences, Patel Nagar, Dehradun, 248001, Uttarakhand, India
3Assistant Professor, Department of Pathology, Sri Guru Ram Rai, Institute of Medical and Health Sciences, Patel Nagar, Dehradun, 248001, Uttarakhand, India
4Professor, Department of Pathology, Sri Guru Ram Rai Institute of Medical, and Health Sciences, Patel Nagar, Dehradun, 248001, Uttarakhand, India
Received Date: May 10, 2023 / Accepted Date: May 18, 2023 / Published Date: May 25, 2023
Copyright: ©©2023 Dr. Apoorva Kumar Pandey et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Mogla S, Pandey AK, Ahmed S and Bhardwaj A (2023). Rhinoscleroma- the Recalcitrant and Indolent Entity: A Case Report. J of ENT Surgery Research, 1(1), 01-03.
Abstract
Rhinoscleroma is a chronic granulomatous disease caused by the bacterium Klebsiella Rhinoscleromatis. It primarily affects the nasal mucosa and can also involve other parts of the respiratory tract. We present a case report of 50-year-old female with rhinoscleroma, who presented with a 4 month history of nasal obstruction, recurrent sneezing and frequent frontal headaches. The diagnosis was confirmed by histopathological examination of nasal biopsy. The patient was treated with a prolonged course of antibiotics, resulting in significant clinical improvement.
Introduction
Rhinoscleroma is a rare chronic granulomatous infectious disease that predominantly affects the nasal mucosa and can also involve other parts of the respiratory tract. It is caused by the bacterium Klebsiella rhinoscleromatis, a gram-negative rod- shaped bacterium that is non-motile, non-spore-forming and non-capsulated. The disease is more common in developing countries, particularly in Africa, Asia, and Latin America, and is rare in developed countries. The incidence of rhinoscleroma in India is not well documented, but it is considered to be relatively rare. The incidence of rhinoscleroma has decreased in recent years due to improved sanitation and living conditions. As the name suggests, the disease commences in the nose but it may also involve oral, pharyngeal and laryngo-tracheobronchial routes [1-5].
Case Report
A 50-year-old female presented to our OPD with a 4 months history of progressively increasing bilateral nasal obstruction, recurrent sneezing, and frequent frontal headaches. She reported that 1 year ago she had accidental trauma to her nose following which she had a few episodes of bleeding from her nose. She was medically managed at multiple places and got no relief from her complaints. There was no history of any drug abuse, smoking, alcohol use, change in voice, or family history of similar symptoms. On clinical examination, a slight widening of the lower part (cartilaginous portion) of nasal pyramid was seen.
On anterior rhinoscopy, a mass, near the vestibule, was seen in the septum bulging in both nasal cavities and it was round, soft, insensitive, and did not bleed to touch. (Figure no 1).
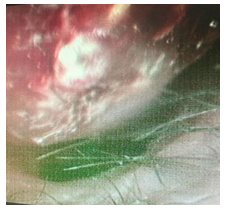
Figure 1: Anterior rhinoscopic picture of the mass in left side nasal cavity. Air passage is compromised on left side.
Computed tomography of the Nose-PNS showed a well-defined homogeneous mass lesion in the anterior nasal cavity along the anterior 1/3rd of nasal septum cartilaginous portion measuring approximately 2.5x2.4cm in size. There were no signs of bone destruction (Figure no 2a, 2b).
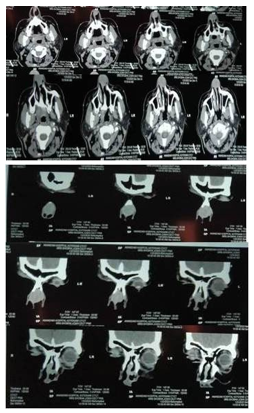
Figure 2a, 2b: Axial and coronal section of CT nose-PNS. Homogenous mass seen in anterior part of nasal cavity involving nasal septum.
The patient underwent biopsy of the mass/lesion under local anesthesia, and histopathology revealed acanthotic stratified squamous epithelium with underlying fibro collagenous stroma showing granulation tissue, few dilated blood vessels surrounded by aggregates of lymphocytes, plasma cells and histiocytes with intracytoplasmic bacilli (mikulicz cells) surrounded by granulation tissue (figure 3a,3b,3c). These findings confirmed the diagnosis of rhinoscleroma.
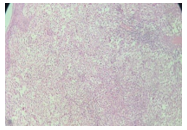
Figure 3a: The section shows acanthotic stratified squamous epithelium with underlying fibro collagenous stroma showing granulation tissue (H & E, 5X)
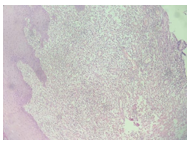
Figure 3b: The section shows fibro-collagenous stroma with dilated blood vessels, surrounded by aggregates of histiocytes, lymphocytes and plasma cells (H&E, 10X).
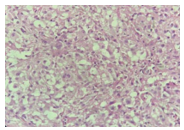
Figure 3c: The section shows clusters of histiocytes with in- tracytoplasmic bacilli surrounded by granulation tissue (H&E, 40X)
The patient was started on medical management with tablet ciprofloxacin 500mg every 12 hourly and tablet rifampicin 450mg every 24 hourly for a period of 6 weeks. The patient responded well to the treatment.
Discussions
For the first time, this rare disease was described in 1870 by Von Hebra. Women are more commonly affected as compared to men. The disease-causing organism has a very high affinity for nasal mucosa [6]. Contact with nasal exudate from an infected person is considered to be the mode of transmission of the disease and humans are the only known hosts. The most commonly affected area is the transition zone of nasal epithelium i.e. junction of stratified squamous epithelium lined vestibule and nasal ciliary epithelium [7].
Rhinoscleroma has 3 clinical stages that include: catarrhal, granulomatous and sclerotic or cicatricial stage. Symptoms of the patient depend on the stage of the disease. In the catarrhal stage, atrophic rhinitis-like symptoms i.e. crusting, foul- smelling purulent discharge, nasal obstruction and sometimes epistaxis occur. In the granulomatous stage, the patient usually develops nasal obstruction due to granulomatous nasal mass. In the sclerotic stage, thick dense scars start developing leading to complications like anosmia, nasal deformities and sometimes stridor [8]. The diagnosis is confirmed by histopathological examination of a biopsy specimen showing classical Mikulicz cells [9]. The treatment of Rhinoscleroma involves prolonged use of antibiotics. Initially, Doxycycline was considered to be a drug of choice but Streptomycin and tetracycline were found to be more effective. Fluoroquinolones like ciprofloxacin and Rifampicin are also used alone or in combination and found to be very effective against the gram-negative bacterium causing rhinoscleroma. Nowadays ciprofloxacin is considered over others as it has very few side effects along with excellent tissue penetration but it cannot be given below 12 years of age as it may cause arthropathy. Surgical intervention is usually required in later stages for the correction of nasal deformities or for symptomatic relief from nasal obstruction. Rhinoscleroma has a chronic course and can recur after treatment, so long-term follow-up is necessary. In this case, we used a combination of rifampicin (450 mg every 24 hourly) and ciprofloxacin (500 mg every 12 hourly) for our patient for a period of at least 6 weeks. A repeat biopsy was done after six weeks, which was negative and the medical treatment was discontinued then. The patient was symptomatically better and the swelling was significantly reduced in size relieving her of nasal obstruction considerably and satisfactorily although not completely.
Conclusion
Although rare, it should be considered in the differential diagnosis of chronic nasal symptoms, particularly in individuals from endemic areas as lack of awareness and a delay in the diagnosis of this disease can lead to complications.
References
- Bailhache A, Dehesdin D, François A, Marie JP, Choussy O.Rhinoscleroma of the sinuses. Rhinology. 2008; 46:338–41.
- Abalkhail A, Satti MB, Uthman MA, Al Hilli F, Darwish A, Satir A. Rhinoscleroma: A clinicopathological study from the Gulf region. Singapore Med J. 2007; 48:148–51.
- D'Souza N, Kulkarni S, Bhagwat S, Marolia R. Airway management of an unusual case of recurrent rhinoscleroma. J Anaesthesiol Clin Pharmacol. 2011; 27:389–92.
- Cone AL, Barton MS, Woodard RD. Treatment of scleroma with ceforanide. Arch Otolaryngol Head Neck Surg. 1987;113:3746.
- Hart AC, Rao SK. Rhinoscleroma. J Med Microbiol. 2000; 49:395–6.
- Inamadar AC, Palit A, Kulkarni NH, Guggarigoudar S P, Yelikar BR. Nodulo-ulcerative lesions over the nose. Indian J Dermatol Venereol Leprol. 2004; 70:197–8.
- Abdel Razek AA. Imaging of scleroma in the head and neck. Br J Radiol. 2012; 85:1551–55.
- Mukara BK, Munyarugamba P, Dazert S, Löhler J. Rhinoscleroma: A case series report and review of the literature. Eur Arch Otorhinolaryngol 2014; 271: 1851-6.
- Moraes MA, Magalhães AV, Marinho LC, Azevedo AE, Carneiro FP, Raymundo IT. Rhinoscleroma causing severe bilateral nasal obstruction. Braz J Infect Dis. 2010; 14:190-2.