




Case Report - (2024) Volume 3, Issue 3
Primary Umbilical Endometriosis Fine Needle Aspiration Cytology Diagnosis: Case Report and Literature Review
2Aksum university college of health science, Department of Surgery, Aksum, Ethiopia
3Aksum university college of health science, Department of obstetrics and Gynecology, Aksum, Ethiopia
4University of Gondar College of Medicine and Health sciences, Ethiopia
Received Date: Oct 31, 2024 / Accepted Date: Dec 13, 2024 / Published Date: Dec 18, 2024
Copyright: ©Â©2024 Birhanu Kassie Reta, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Reta, B. K., Gebremedhin, K. G., Gebreyesus, T. A., Gebreslase, M. N., Hailemariam, B. G. (2024). Primary Umbilical Endometriosis Fine Needle Aspiration Cytology Diagnosis: Case Report and Literature Review. J Surg Care 3(3), 01-05.
Abstract
Introduction Umbilical endometriosis is a rare form of endometriosis accounting for 0.5-1% of total cases of endometriosis. It may occur in the setting of prior abdominopelvic surgical procedures or spontaneously, where the latter is more common. The classic clinical presentation is red or black painful nodule with cyclical nature of pain. Initial diagnosis is usually made clinically but histopathologic confirmation is required. Fine needle aspiration cytology is also diagnostic for endometriosis. This case report is aimed to highlight the role of Fine needle aspiration cytology in diagnosing endometriosis, and discus the clinical presentation, pathogenesis and diagnosis of primary umbilical endometriosis with review of previously published case reports.
Presentation of Case A 24 years old nulliparous woman presented with slowly growing umbilical swelling and pain of 02 years duration. The pain worsens with menses. She had no history of previous surgical procedure. On physical examination there was well defined, non-tender, firm mobile subcutaneous mass with overlying skin hyperpigmentation measuring, 23mm*19mm. Fine needle aspiration cytology was done from the nodule and the findings were consistent with endometriosis. Subsequent histopathologic examination also confirmed the diagnosis of endometriosis.
Conclusion Even though it is rare, primary umbilical endometriosis should be considered in a women of reproductive age group presenting with painful umbilical mass. With favorable clinical setting, fine needle aspiration cytology is cost effective, fast and accurate diagnostic modality in diagnosing umbilical endometriosis.
Keywords
Umbilical, Endometriosis, Abdominal Wall, Primary
Abbreviations
FNAC-Fine Needle Aspiration Cytology; Hand E-Hematoxylin and EosinIntroduction
Endometriosis is defined as the presence of endometrial glands and stroma outside the uterine cavity [1]. The ovaries, fallopian tubes, and structures in vicinity to the ovary and uterus are commonly involved by endometriosis [2]. The ovary is the commonest site affected by endometriosis [1]. Endometriosis can also occur outside the pelvic cavity, where the abdominal wall and thoracic cavity making the commonest extrapelvic sites of endometriosis. Umbilical endometriosis is a rare form of endometriosis accounting for 0.5-1% of total cases of endometriosis, and 0.4-4% of extragenital endometriosis. Umbilical endometriosis clinically presents with red or purple or black umbilical mass. Associated with the mass lesion they also manifest with umbilical pain which worsens with menses, and bleeding in the periumbilical area [3, 4].
Umbilical endometriosis is classified as primary and secondary depending on whether the patient has previous surgery or not. The surgical procedure can be open or laparoscopic. Umbilical endometriosis occurring spontaneously is called primary and, those cases associated with previous abdominopelvic procedure are called as secondary. Primary umbilical endometriosis accounts for 70% of total cases of umbilical endometriosis. One of the theoretical explanations for primary umbilical endometriosis is shedding of endometrial cells which are transported by lymphovascular system to the umbilicus [4]. Diagnosis of umbilical endometriosis is initially clinical, but histopathologic confirmation is required [4]. Fine needle aspiration cytology (FNAC) is also fast and accurate diagnostic tool for diagnosing endometriosis. Cytologic examination of endometriosis demonstrates mainly epithelial cells and stromal component with occasional hemosiderin laden macrophages. Surgical management is currently the main stay of treatment of umbilical endometriosis. Here by we present a case of 24-year-old woman diagnosed with primary umbilical endometriosis after she presented with painful umbilical nodule of 02 years duration.
Presentation of Case
History and Physical Examination
This is a 24-year-old nulliparous woman presented to Aksum university comprehensive specialized hospital surgical outpatient department, with complaint of slowly growing umbilical swelling and pain of 02 years duration. She claimed that the pain is dull aching in type and worsens with menses. Otherwise, no history of lower abdominal pain, dysmenorrhea or dyspareunia. She has no history of previous abdominal surgical procedure. On physical examination, her vital signs were within normal range. Abdominal examination demonstrated firm mobile non-tender subcutaneous umbilical mass with overlying skin hyperpigmentation measuring, 23mm*19mm (Figure 1). Pelvic examination was non-revealing.

Figure 1: Clinical Photograph of The Hyperpigmented Umbilical Nodule
Diagnostic Assessment
Routine laboratory investigation values were within normal range. Abdominal ultrasound scan revealed hypoechoic mass in the deep plane of skin with irregular border, measuring 18mm*13mm. The uterus, ovaries and other pelvic structures are normal in size and appearance, with no identifiable lesion in the pelvis and abdominal cavity. Abdominopelvic computed tomography (CT) scan was planned but it was not available at our center. FNAC from the nodule was done, and it showed cellular aspirate displaying monolayered sheets and loose clusters of monotonous round to oval epithelial cells having mild to moderate cytoplasm and finely chromatined nuclei, in a background of loose clusters and single cells of bland oval to spindle stromal cells with scant cytoplasm (Figure 2). Having the provided history of cyclical pain and the clear cut cytologic findings, the diagnosis of endometriosis was rendered on FNAC.
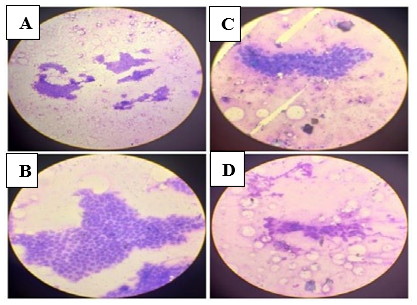
Figure 2: Cytology Microscopic Images
A. 10x magnification displaying monolayered sheets and loose clusters of bland round to oval epithelial cells. B. 20x magnification of image A, demonstrating the honey comb sheets of monotonous epithelial cells. C. 20x magnification displaying the epithelial cells forming gland like structures. D. 20x magnification showing the loose clusters of bland oval to spindle stromal cells, and background bare nuclei.
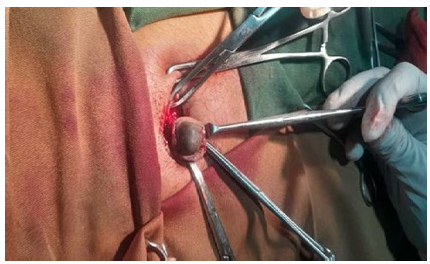
Figure 3: Photograph of The Surgical Removal of Umbilical Nodule
With impression of primary umbilical endometriosis, excisional biopsy was done and sent for further pathologic examination. The histopathologic examination macroscopically revealed, dermal based grey white lesion with irregular border having microcystic spaces measuring 18mm*12mm*10mm (Figure 4). Microscopically the H and E (Hematoxylin and eosin) examination revealed dermal based lesion displaying variable sized glands lined by cuboidal to columnar epithelium containing round to oval pseudostratified nuclei and moderate amphophilic cytoplasm, surrounded by endometrial stroma demonstrating areas of mononuclear inflammation, myxoidy change and hemorrhage (Figure 5). No atypia or mitosis is noted.
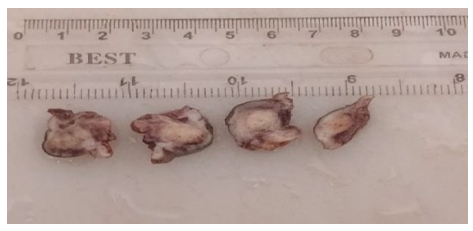
Figure 4: Histopathology Gross Pictures: Cut Surface of the Umbilical Nodule Specimen Displaying Grey White Dermal Based Mass with Microcystic Spaces
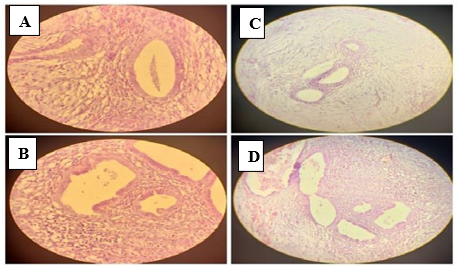
Figure 5: Histopathologic Microscopic Images
A. 20x magnification displaying endometrial glands surrounded by endometrial stroma. B. 20x magnification demonstrating endometrial glands and stroma with mononuclear inflammatory cells. C. 10x magnification showing the endometrial stoma with areas of myxoid change. D. 10x magnification displaying areas of stromal hemorrhage.
Therapeutic Intervention
With the working diagnosis of primary umbilical endometriosis, the patient was counseled on options of management and she opted for surgical management. Under local anesthesia and sedation wide skin incision and en block excision of the mass with skin, the muscles and fascia was done (Figure 3). The excised sample was sent for histopathologic examination.
Outcome and Follow up
Currently, on the time of writing the case report, she is on her 18th postoperative day, she is doing good. Vital signs were within normal range and abdominopelvic ultrasound was done and it was unremarkable. No surgical complications are witnessed. The abdominal surgical wound is on optimal healing (Figure 6). Figure 6: Clinical Photograph of the Surgical Site on 18th Postoperative Day

Discussion
Endometriosis is a chronic proinflammatory condition characterized by presence of endometrium-like tissue outside the uterine cavity and, presence of the endometrial tissue at ectopic sites induces recruitment of proinflammatory cytokines resulting in sustained inflammation at involved sites. Endometriosis affects about 10% of women within reproductive age group [1,5,6]. Even though pelvic structures are mostly involved, endometriosis can also affect the intestine, abdominal wall, thoracic cavity, bladder and other organs. Among extrapelvic sites, abdominal wall endometriosis is the most common.
Umbilical endometriosis is one form of abdominal wall endometriosis constituting 0.5-1% of total cases of endometriosis and 30-40% of cases of abdominal wall endometriosis. About 25% of cases of umbilical endometriosis seen to have concurrent pelvic endometriosis. In our instance the ultrasound examination excluded presence of concurrent lesion at other sites. Umbilical endometriosis is classified as primary, which occur in the absence of previous surgical procedure, and secondary occurring in women who had previous surgery. The surgical procedures can be open or laparoscopic, and the former is more commonly associated with occurrence of endometriosis. There are postulated theories for development of endometriosis which includes; Sampson’s theory of retrograde menstruation, hematogenous or lymphatic spread theory, coelomic metaplasia theory, stem cell recruitment theory and embryogenetic theory. Of those theories retrograde menstruation theory is the most accepted theory [4-9]. Lymphatic or hematogenous spread theory is the likely theory to explain pathogenesis of primary umbilical endometriosis.
Clinically primary umbilical endometriosis presents with red or purple or black nodule [10]. Associated with the swelling they also have pain which usually worsens with menses, and bleeding from the swelling [8,10-12]. Similarly, our patient had hyperpigmented umbilical mass with associated cyclical pain, but she did not report bleeding from the mass. Diagnosis of primary umbilical endometriosis is initially clinical, but it should be confirmed by histopathology with Hand E examination [4]. The differential diagnosis for primary umbilical endometriosis includes; hamartoma, pyogenic granuloma, sarcoma, lymphoma [13-15]. Sister Marry Joseph’s nodule is also one cause of confusion with primary umbilical endometriosis clinically [8]. Sensitivity and specificity of ultrasonography, CT scan and magnetic resonance imaging (MRI) in diagnosing umbilical endometriosis is not clearly known and there are no pathogenomic features of umbilical endometriosis in imaging findings [16-18]. Definitive diagnosis of endometriosis is usually made by FNAC, histopathology and immunohistochemistry [15].
Fine needle aspiration cytology examination of umbilical endometriosis usually demonstrates epithelial cell clusters, stromal cells and admixed hemosiderin laden macrophages [19-21]. The cytomorphology typically displays a regularly arranged clusters pf epithelial cells comprising bland uniform cells, with loose clusters of stromal cells [20]. In our case FNAC and histopathology findings were consistent with endometriosis. Currently the mainstay of treatment of umbilical endometriosis is surgical exploration and removal of the nodule [4,10,15,17,18]. Recurrences are rare after surgical removal of the nodule [16]. There are reports which estimated recurrence rate of 5-9%, with higher rate for larger masses [2]. Medical management with combined oral contraceptives and progestins is also another option of treatment, which is intended to minimize the inflammatory effect and stimulation of endometrial implants [4]. This medical approach can be used to relief clinical symptoms but it is not curative [18].
Conclusion
In conclusion even though it is rare, primary umbilical endometriosis should be considered in a women of reproductive age group presenting with painful umbilical mass. With favorable clinical setting fine needle aspiration cytology is cost effective, fast and accurate diagnostic modality in diagnosing umbilical endometriosis.
Acknowledgement
None.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethics Approval
Ethical approval for publication of this case report is obtained from Aksum university ethics committee.
Funding
This study did not receive any grants or funding from either for- profit or non-profit organizations.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper
Data Availability
Data will be made available upon request
References
- Wang, P. H., Yang, S. T., Chang, W. H., Liu, C. H., Lee, F.K., & Lee, W. L. (2022). Endometriosis: part I. basic concept. Taiwanese Journal of Obstetrics and Gynecology, 61(6), 927-934.
- Yang, E., Chen, G. D., & Liao, Y. H. (2023). Spontaneous abdominal wall endometriosis: a case report and review of the literature. Taiwanese Journal of Obstetrics and Gynecology, 62(1), 155-157.
- Ferjaoui, M. A., Arfaoui, R., Khedhri, S., Abdessamia, K., amine Hannechi, M., Hajjami, K., ... & Neji, K. (2021). Abdominal wall endometriosis: A challenging iatrogenic disease. International Journal of Surgery Case Reports, 88, 106507.
- Ogamba, I., Napolitano, S., Chuang, L., August, D., & LaVorgna, K. (2022). Primary umbilical endometriosis presenting with umbilical bleeding: a case report. Case Reports in Women's Health, 36, e00441.
- Allaire, C., Bedaiwy, M. A., & Yong, P. J. (2023). Diagnosis and management of endometriosis. Cmaj, 195(10), E363-E371.
- Cano-Herrera, G., Salmun Nehmad, S., Ruiz de Chávez Gascón, J., Méndez Vionet, A., van Tienhoven, X. A., Osorio Martínez,M. F., ... & Cabrera Carranco, R. (2024). Endometriosis: A Comprehensive Analysis of the Pathophysiology, Treatment, and Nutritional Aspects, and Its Repercussions on the Quality of Life of Patients. Biomedicines, 12(7), 1476.
- Chauhan, S., More, A., Chauhan, V., & Kathane, A. (2022). Endometriosis: a review of clinical diagnosis, treatment, and pathogenesis. Cureus, 14(9).
- Guindo, B., Tall, K., Kitha, P., Keita, A., & Dissa, L. (2024). Umbilical Endometriosis: About a Case at the Dermatology Hospital of Bamako. J Dermatolog Clin Res, 12(3):1166.
- Signorile, P. G., Viceconte, R., & Baldi, A. (2022). New insights in pathogenesis of endometriosis. Frontiers in medicine, 9, 879015.
- Dridi, D., Buggio, L., Donati, A., Giola, F., Lazzari, C., Brambilla, M., ... & Barbara, G. (2022). Clinical features and management of umbilical endometriosis: a 30 years’ monocentric retrospective study. International Journal of Environmental Research and Public Health, 19(24), 16754.
- Cousins, F. L., McKinnon, B. D., Mortlock, S., Fitzgerald, H. C., Zhang, C., Montgomery, G. W., & Gargett, C. E. (2023). New concepts on the etiology of endometriosis. Journal ofObstetrics and Gynaecology Research, 49(4), 1090-1105.
- Dridi, D., Chiaffarino, F., Parazzini, F., Donati, A., Buggio, L., Brambilla, M., ... & Vercellini, P. (2022). Umbilical endometriosis: a systematic literature review and pathogenic theory proposal. Journal of clinical medicine, 11(4), 995.
- Becker, C. M., Missmer, S. A., & Zondervan, K. T. (2020). Endometriosis: the authors reply. New England Journal of Medicine, 383(2).
- Paramythiotis, D., Karlafti, E., Tsomidis, I., Iraklis, G., Malliou, P., Karakatsanis, A., & Antonios, M. (2022). Abdominal wall endometriosis: a case report. Pan African Medical Journal, 41(1).
- Beyene, S. A., Bogale, N. T., Berhe, B. M., & Teshome, D. D. (2024). Primary Umbilical Endometriosis: A Case Report and Literature Review. Open Access Surgery, 157-160.
- Theunissen, C. I., & IJpma, F. F. (2015). Primary umbilical endometriosis: a cause of a painful umbilical nodule. Journal of Surgical Case Reports, 2015(3), rjv025.
- Hirata, T., Koga, K., & Osuga, Y. (2020). Extra-pelvic endometriosis: a review. Reproductive medicine and biology, 19(4), 323-333.
- Makena, D., Obura, T., Mutiso, S., & Oindi, F. (2020). Umbilical endometriosis: a case series. Journal of Medical Case Reports, 14, 1-4.
- Singh, G., Brar, K., Parmar, P., Prakash, K. S., Yadav, N., & Sen, R. (2017). Scholars Journal of Medical Case Reports ISSN 2347-9507 (Print) Primary umbilical endometriosis: cytological diagnosis of a rare presentation. Sch J Med Case Rep, 5(3):197–8.
- Song, S. J., McGrath, C. M., & Yu, G. H. (2017). Fine-needle aspiration cytology of endometriosis. Diagnostic Cytopathology, 45(4), 359-363.
- Fernandes, H., Marla, N. J., Pailoor, K., & Kini, R. (2011). Primary umbilical endometriosis-Diagnosis by fine needle aspiration. Journal of cytology, 28(4), 214-216.