
Hypertension: Open Access(HOA)
ISSN: 3143-0740 | DOI: 10.33140/HOA

Research Article - (2025) Volume 1, Issue 1
Prevalence of Chronic Kidney Disease and Associated Factors Among Hypertensive Patients in Ethiopia: A Systematic Review and Meta-Analysis
2Department of Health Promotion and Health Behavior, School of Public Health, College of, Medicine and Health Science, University of Gondar, 196, Gondar, Ethiopia
3Department of Nutrition, Antsokiya Gemza wereda Health Ofice, North, Shoa, North East Ethiopia, Mekoy, Ethiopia
4Department of emergency and critical care nursing, College of Medicine, and Health Science, Bahir Dar University, Bahir Dar, Ethiopia
5Health Promotion and Behavioral science department, school of public health, college of medicine and health science, Bahir Dar University, Bahir Dar, Ethiopia
Received Date: Jan 13, 2025 / Accepted Date: Feb 14, 2025 / Published Date: Mar 24, 2025
Copyright: ©Â©2025 Kedir Seid, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Seid, K., Lakew, G., Bogale, S. K., Getachew, E., Yirsaw, A. N., et al. (2025). Prevalence of Chronic Kidney Disease and Associated Factors Among Hypertensive Patients in Ethiopia: A Systematic Review and Meta-Analysis. Hypertens OA, 1(1), 01-11.
Abstract
Background: Hypertension is most common global cause of cardiovascular disease and death in the worldwide. Patients with target organ damage, particularly chronic kidney disease, are more common because of hypertension. Even though many primary studies have reported the prevalence of chronic renal disease. Thus, the purpose of this study was to determine the overall prevalence of chronic kidney disease and predictors among Ethiopian hypertensive patients.
Method: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist was used to select potential studies. PubMed, scopes, and web of science were searched to identify relevant studies. The estimated pooled prevalence and related variables of chronic renal disease were determined using STATA 17.0.
Result: Four research totaling 1,675 study participants were included in this meta-analysis. The pooled prevalence of CKD among hypertensive patients was found to be 21% (95% CI: 18–24). Age ≥ 60 years (OR = 1.73, 95%, CI: 1.02, 2.44), uncontrolled hypertension (OR = 4.64, 95%, CI: 1.83, 7.44), duration of hypertension >=10 years (OR = 6.05; 95% CI 3.40–8.70) and having co-morbid diseases (OR = 4.24; 95% CI: 1.46–7.03) were significantly associated with CKD.
Conclusion: This study showed that the prevalence of chronic kidney disease remains high among hypertensive patients in Ethiopia. This study found that Age ≥ 60 years, uncontrolled hypertension, duration of hypertension >=10 years and having diabetes diseases were associated with chronic kidney disease among hypertensive patients. Therefore, situation-based interventions and preventive strategies should be developed.
Keywords
Hypertension, Chronic Kidney Disease, Prevalence
Acronym and Abbreviation
CKD: Chronic Kidney Disease
ESKD: End Stage Chronic Kidney Disease
ESRD: End Stage Renal Disease
eGFR: estimated Glomerular Filtration Rate
NCD: Non-Communicable Disease
NOS: Newcastle–Ottawa scale
PRISMA: Preferred Reporting Items for Systematic reviews and Meta-analyses
SDG: Sustainable Development Goal
USRDS: United States Renal Data System
Introduction
Chronic kidney disease (CKD) A progressive loss of kidney function that affects the kidneys' capacity to handle waste and other vital functions, as well as renal impairment or low glomerular filtration rate, GFR < 60 mL/min per 1.73m2) greater than 3 months [1-3]. KDIGO definition: AKI, or GFR <60 ml/min per 1.73 m2, or markers of kidney damage for ≤3 mo, or decrease in GFR by ≥35% or increase in serum creatinine by >50% for ≤3 months [4].
The normal GFR is 125 mL/min/1.73 m2 , and there are five stages of CKD: Stage 1 if GFR ≥ 90 mL/min/1.73 m2 (harm with regular or heightened GFR), Stage 2 if GFR = 60 – 89 mL/min/1.73 m2 (mild decrease in GFR), Stage 3 if GFR = 30 – 59 mL/min/1.73 m2 (moderate decrease in GFR), Stage 4 if GFR = 15 – 29 mL/ min/1.73 m2 (severe decrease in GFR), and Stage 5 if GFR < 15 mL/min/1.73 m2 (end-stage renal disease) [3,5]. End stage renal diseases (ESRD) is irreversible and fatal, unless treated by dialysis or kidney transplant [6].
Over 800 million people, or more than 10% of the global population, suffer from chronic kidney disease, a degenerative illness. adults with diabetes mellitus, hypertension, women, older adults, and members of racial minorities are more likely to have chronic kidney disease. e, or more than 10% of the global population, suffer from chronic kidney disease, a degenerative illness. adults with diabetes mellitus, hypertension, women, older adults, and members of racial minorities are more likely to have chronic kidney disease [7].
Globally 850 million individuals live with the chronic kidney disease with all-age prevalence of 29.3% [8,9]. According to a prior worldwide comprehensive review and meta-analysis, 27% of patients with type 2 diabetes had chronic renal disease. The prevalence of chronic kidney disease differs across countries, with the maximum in the USA and the lowest in the United Arab Emirates [10].
African Americans are more likely than Hispanics or Caucasians to have chronic kidney disease (CKD), or kidney failure brought on by hypertension, according to data from the United States Renal Data System (USRDS) [11].
Research indicates that a variety of risk factors contribute to chronic kidney disease (CKD), even if the exact origin of the disease is still unknown such as obesity [12-15]. Old age, hypertension, diabetes mellitus [9,13-17]. male gender, family history of kidney disease, HIV infection, electrolyte and acid-base disturbances [13,15,18,19]. Low-income occupation, use of traditional medication, and low hemoglobin, Stroke [15,20]. Diseases of the peripheral vessels, gout, anxiety and depression as well as declines in patients' quality of life and a noticeable rise in medical expenses [21-25]. Patients with CKD may eventually progress to end-stage kidney disease (ESKD), which is associated with a high burden of disease and significant costs of treatment [26].
The pathophysiological states of chronic kidney disease and hypertension are strongly related; persistent hypertension can worsen kidney function, and progressive renal decline can inversely worsen blood pressure (BP) regulation. There is a negative and cyclical relationship between CKD and HTN [27].
Growing public health concerns are related to the potential for non-communicable disease (NCD) such as chronic kidney disease (CKD), which are mostly caused by higher rates of obesity, smoking, and hypertension. For those residing in poor nations, it is becoming a serious problem [28,29]. Hypertension is considered as the major contributing determinants for CKD [25,30].
Rational and Objective of the Study
Ethiopia was signed to achieve sustainable development goal (SDG) from 2016 to 2030 and to reduce by one third premature death from non-communicable diseases [25]. Although chronic kidney disease is a prevalent, progressive, and treatable condition, most individuals worldwide lack access to or cannot afford the therapies. Determining the impact of hypertension in chronic kidney disease (CKD) in Ethiopia is crucial, given the severe limitations on treatment access and the exceedingly poor outcomes associated with chronic kidney failure and CKD, respectively. As a result, the goal of this study is to evaluate the pooled prevalence and related variables of chronic kidney disease (CKD) thoroughly and methodically from studies that identified hypertension as the primary cause of the disease.
Materials and Methods
Data Source and Search Strategy
The Preferred Reporting Items Standards for Systematic Reviews and Meta-analyses (PRISMA) declaration was followed in the conduct of this systematic review and meta-analysis [31]. We registered the protocol in PROSPERO (CRD 42023495007. We searched articles regardless of the year of publication, from PubMed, Scopus, and the web of Science to identify published reports of kidney disease among hypertensive patients in Ethiopia up to January 20, 2024.
Moreover, the reference lists of every article that was retrieved were examined to find more pertinent studies and reduce publication bias as much as feasible. Only free articles, full texts, human studies, and all language publications were included in the search parameters. The software Endnote X 6.1 reference manager was utilized to do a search, gather, arrange, and eliminate duplicate articles. During the search, we used Boolean operators such as “AND” and “OR” which were used to combine search terms: prevalence OR magnitude OR epidemiology OR incidence AND chronic kidney disease OR chronic kidney failure OR renal impairment OR end-stage kidney/renal disease OR renal insufficiency AND hypertensive patients OR essential hypertension OR uncontrolled hypertension and associated factors OR risk factors OR determinants OR predictors AND Ethiopia (Table 1).
Study Selection and Eligibility Criteria
Inclusion Criteria for this Study Were as Follows
Studies that did not meet the following criteria were eliminated: (1) they were not fully available; (2) they had a low-quality score according to the specified criteria; (3) case series, letters, comments, and editorials; and/or (4) they did not measure the intended outcome (chronic renal disease).
Study Selection: Following the search, all identified citations were uploaded into EndNote version 6.1, and duplicates were removed. Two reviewers (KSY and EKB) examined titles and abstracts to see whether they met the review's inclusion requirements. Two reviewers thoroughly evaluated the complete text of the chosen citations in relation to the inclusion criteria (GL and EG). The systematic review documented and reported the reasons behind the exclusion of full-text articles that did not fit the inclusion criteria. At every stage of the study selection process, conflicts among the reviewers were settled through discussion.
Data Extraction and Quality Assessment
Extraction of data and evaluation of quality when there was a disagreement, GL and GE came to a consensus. KSY and AY extracted the data independently and in duplicate. The first author's name, the study area and region, the study design, the total sample size, the sample size of study participants with hypertension, the study participants' starting age, the eGFR equation used for assessment, the number and prevalence of participants with CKD with its 95% confidence interval (CI), and associated factors were all taken from a subset of the studies. The third author (EKB) double-checked both tables to make sure there was consistency once the data was extracted.
Throughout the data extraction process, disagreements were resolved by consensus among the group. The Newcastle-Ottawa scale was used to assess the methodological quality of each included study (NOS) [32]. Representativeness, response rate, outcome assessment methodology, subject comparability, and suitability of the statistical test employed for data analysis are all evaluated on this tool. Studies that scored at least five out of 10 in three of the ten modified NOS components for observational studies were included in the analysis [33]. Furthermore, quality assurance checks were performed by two authors (YAA and WSS). All authors contributed their opinions to the collective resolution of any disputes pertaining to each article, with a consensus being reached at the end (supplementary file 1).
Assessment of Risk of Bias in Included Studies: All of the included studies underwent a risk of bias evaluation, which was created by Hoy et al. (38) to evaluate the internal and external validity of nonrandomized studies in meta-analyses. Studies were categorized as "high risk of bias" (total score ≤4), "moderate risk of bias" (total score between 5 and 7), or "low risk of bias" (total score between 8 and 10) based on the Hoy score, which is expressed as an out of ten (supplementary file 2). Two writers assessed the studies included in the analysis for potential bias.
Heterogeneity and Publication Bias: Cochran’s Q and the I2 statistics were employed to investigate heterogeneity between studies which estimates the percentage of total variation across studies due to true between-study differences rather than chance, with I2 values of 25, 50, and 75% denoting, respectively, moderate, medium, and great heterogeneity [34]. We explored sources of heterogeneity through subgroup analysis and Meta regression analysis. Sensitivity analysis was also carried out to determine how each study affected the prevalence overall. By objectively applying Egger's test and visually examining funnel plots, publication bias was evaluated [35].
Statistical Analysis: We used the Der Simonian–Laird random-effects models to generate the pooled prevalence of CKD due to the anticipation of substantial variations in CKD prevalence estimates across the included studies. After important information was extracted on Microsoft excel from each original study, the data were exported to STATA for windows version 17 for analysis. The burden of CKD with 95% confidence interval and OR of the association between CKD among patients with hypertensive and its determinants were presented in the form of a forest plot. All the results are reported using PRISMA checklist (Table1).
Results
A total of 198 published articles were identified from PubMed, scopes and web of science. Of the total identified studies, 69 duplicates papers were removed, and 114 records were excluded by reviewing titles and abstracts. The full text of the remaining 15 studies was assessed and screened for eligibility. Accordingly, 9 studies were excluded based on pre-determined eligibility criteria. Finally, 4 articles fulfilled the eligibility criteria were included in the final analysis. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram was used to give the summary of the systematic review (Figure 1).
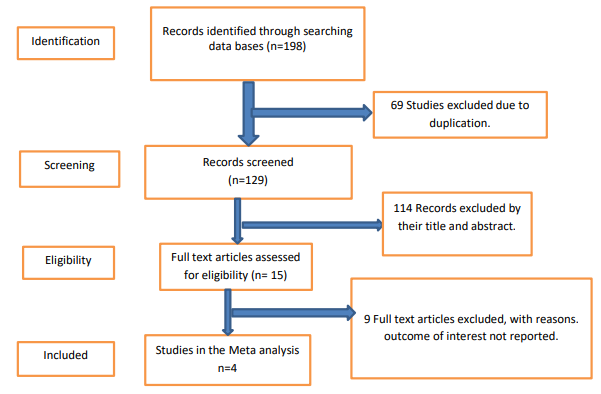
Figure 1: Flow Diagram of the Studies Included in the Meta-Analysis
Baseline Characteristics of the Studies and Study Participants: Of the 4 included studies, all were published articles. A total of 1,675 study participants with hypertension were included in the review. The subjects who participated in the studies were males and females aged ≥18 years. Regarding study design, all the studies were cross- sectional studies and institutional based assessment. The number of study participants per study ranged from 208 to 581 [36,37]. The prevalence of CKD in patients with hypertension was obtained from various regions in Ethiopia; one study from Amhara region, 2 studies from Oromia region and 1 study from Tigrai region [36-39]. With regard to the sampling technique, Two studies used systematic random sampling, one study used simple random sampling, one study Consecutive sampling technique [36-39]. The quality score of the included studies was assessed based on the Newcastle–Ottawa quality score. Among the included studies, the prevalence of chronic kidney disease among hypertensive patients ranges from 17.6% to 26% (Table 1) [36,37].
|
Author |
Publication Year |
Region |
Study area |
Study design |
Sampling technique |
Diagnostic criteria |
Sample size |
Response rate (%) |
Prevalence (%) of CKD (95% CI) |
Quality assessment based on NOS |
|
Bahrey D et al.[39] |
2019 |
Tigrai |
Tigray teaching hospitals |
Cross- sectional |
Consecutive sampling technique |
Cockcroft- gault Equation |
578 |
100 |
22.1(18.5-25) |
8 |
|
Ewnetu H. et al.[38] |
2022 |
Oromia |
Ambo Town Public Hospitals |
Cross- sectional |
Simple random sampling Technique |
CKD–EPI equation |
308 |
100 |
20.5(16-25) |
6 |
|
Hunegnaw A. et al. [37] |
2020 |
Amhara |
Northwest Amhara Referral Hospitals |
Cross- sectional |
Systematic random sampling technique |
Cockcroft– Gault |
581 |
100 |
17.6(14.7– 20.8) |
9 |
|
Kumela G. et al. [36] |
2019 |
Oromia |
Jimma University Medical Center |
Cross- sectional |
Systematic random sampling technique |
CKD–EPI equation |
208 |
100 |
26(20.3-31.8) |
7 |
Table 1: Baseline Characteristics of the Included Studies in Meta-Analysis
Pooled Prevalence of Chronic Kidney Disease Among Patients with Hypertension in Ethiopia
Overall, the pooled prevalence of CKD among patients with hypertension in Ethiopia was 21% (95% CI: 18–24, I2 = 59.45%, p < 0.001)) (Figure 2). Two studies reported the prevalence with the Cockcroft–Gault [37,39].. Two studies used the CKD-EPI equation [36,38]. Meta-regression was computed to see underlying sources of heterogeneity using sample size and year of publication, but none of them showed a statistically significant presence of heterogeneity (Table 2).
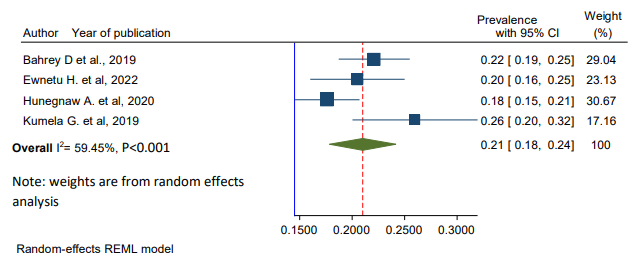
Figure 2: Forest Plot Showing the Pooled Prevalence of Chronic Kidney Disease Among Hypertensive Patients in Ethiopia, 2024
|
Variables |
Coefficients |
Std. error |
p-value |
(95% conf. interval) |
|
Publication year |
-0.0182647 |
0.0113272 |
0.107 |
-0.0404657 0.0039363 |
|
Sample size |
-0.0001656 |
0.0000854 |
0.053 |
-0.000333 1.86e-06 |
Table 2: Meta-Regression Analysis for the Included Studies to Identify the Source(S) of Heterogeneity
Publication Bias
As shown in Figure 3, the visual inspection of the funnel plot showed that there was no publication bias among the included studies, as illustrated by the symmetrical distribution of the funnel plot, when burden of CKD was evaluated. Likewise, the result of Egger’s test was not statistically significant for the presence of publication bias (P = 0.100) (Figure 3).
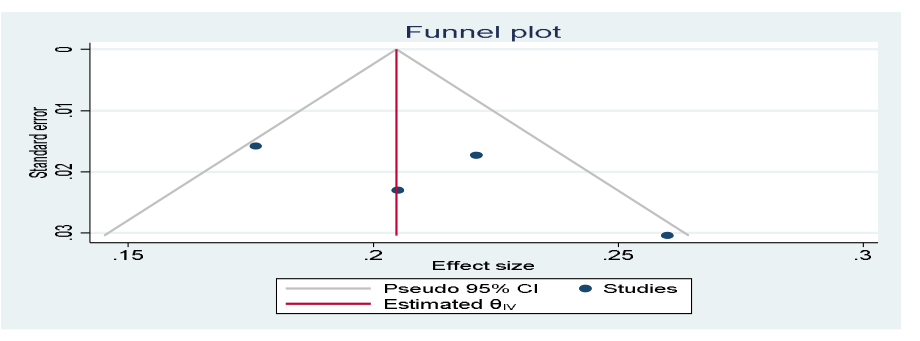
Figure 3: Forest Plot Showing Publication Bias Among Studies, 202
Determinants of Chronic Kidney Disease Among Patients with Hypertension in Ethiopia
Based on this meta-analysis, chronic kidney disease among hypertensive patients in the Ethiopian context was associated with uncontrolled hypertension, age ≥ 60 years, duration of hypertension >=10 years and having co-morbid diseases were factors significantly associated with the presence chronic kidney disease among hypertensive patients.
Age and Chronic Kidney Disease
To see the effect of age on CKD among hypertensive patients, two studies were included in meta-analysis [38,39]. In the present analysis, the pooled effect of two studies showed that age ≥ 60 years was statistically associated with CKD in patients with hypertension (OR = 1.73, 95%, CI: 1.02, 2.44). The heterogeneity test (I2=74.77%) showed significant evidence of variation across studies (Figure 4).
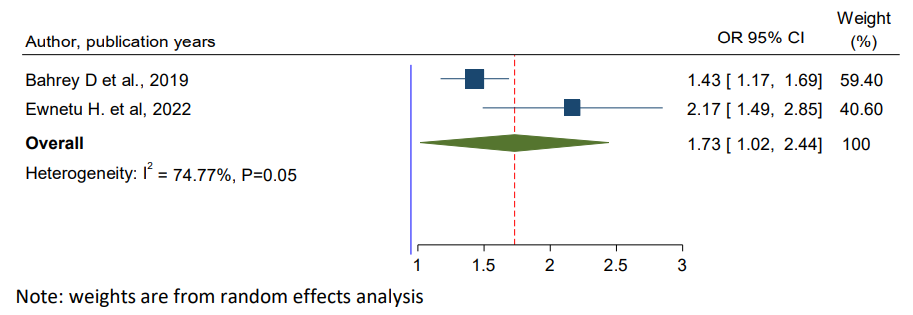
Figure 4: Forest Plot for Pooled Effect of Age >= 60 Years on Chronic Kidney Disease Among Hypertensive Patients in Ethiopia, 2024
Dyslipidemia and Chronic Kidney Disease
To see the effect of dyslipidemia on CKD among hypertensive patients, two studies were included in meta-analysis [37,39]. The pooled result showed that, there was not a statistically significant association between dyslipidemia and CKD among hypertensive patients in Ethiopia (OR (8.57, 95%, CI: -1.57, 18.72) (Figure 5).
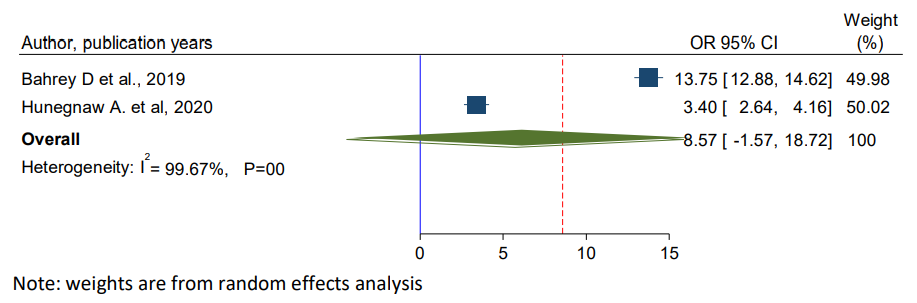
Figure 5: Forest Plot for Pooled Effect of Dyslipdmia on Chronic Kidney Disease Among Hypertensive Patients in Ethiopia, 2024
Uncontrolled Hypertension and Chronic Kidney Disease
To observe the pooled effect of uncontrolled hypertension on CKD, four studies were selected in the final meta-analysis [36-39]. All of 4 studies showed the presence of a statistically significant association between uncontrolled hypertension on CKD. In the present study, high heterogeneity was observed (I2= 97.94%, p-value < 0.001), a random-effects model was used to report the effect of uncontrolled hypertension on CKD. The pooled effect showed that the odds of developing CKD were 4.64 times more likely among patients with uncontrolled hypertension than their counter parts (OR = 4.64, 95%, CI: 1.83, 7.44) (Figure 6).
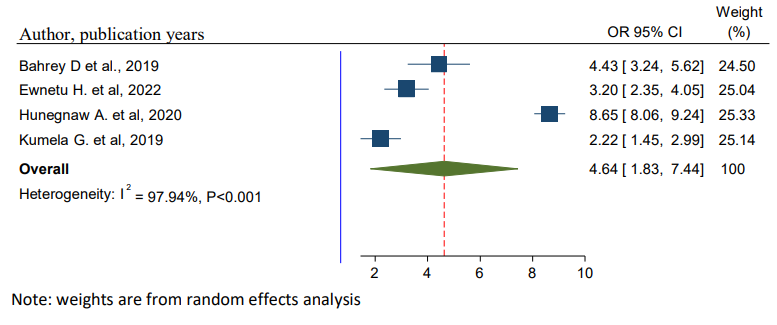
Figure 6: Forest Plot for Pooled Effects of Uncontrolled Hypertension on CKD Among Patients with Hypertension in Ethiopia, 2024
Duration of Hypertension and Chronic Kidney Disease
Three studies were identified to see the effect of duration of patients stayed with hypertension on the occurrence of CKD [36- 38]. The pooled finding indicates that, the duration of the patients stayed with hypertension were significantly associated with the development of CKD among hypertensive patients. Patients with duration of hypertension ≥10 years were 6.05 times more likely to develop CKD as compared to patients with duration of hypertension (AOR = 6.05; 95% CI 3.40–8.70) (Figure 7).
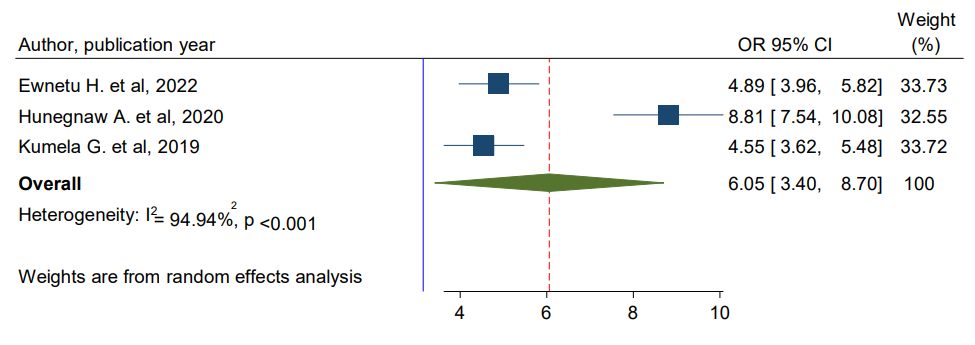
Figure 7: Forest Plot for Pooled Effects of Long Duration of Hypertension on CKD Among Patients Hypertensive in Ethiopia, 2024
Diabetes and Chronic Kidney Diseases
The pooled effects of three studies indicated that those patients who had diabetes diseases were 4.24 times more likely to develop CKD than patients who had no diabetes diseases (OR = 4.24; 95% CI: 1.46–7.03) (Figure 8) [36,37,39].
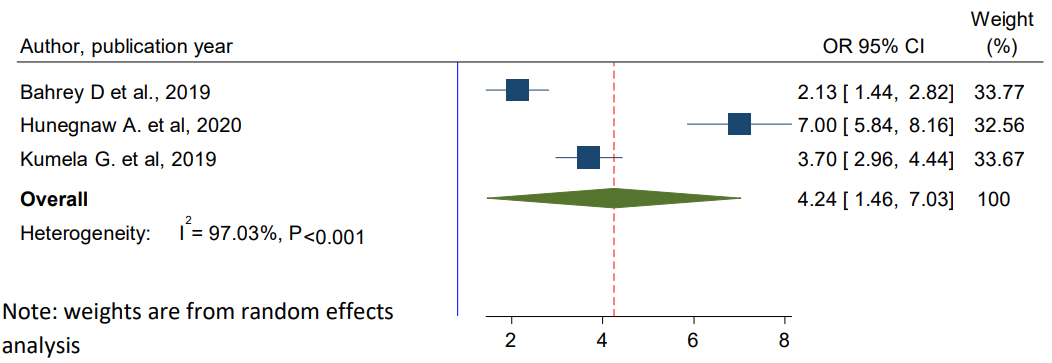
Figure 8: Forest Plot for Pooled Effects of Diabetes Diseases on CKD Among Hypertensive Patients in Ethiopia, 2024
Discussion
Hypertension is a major global cause of morbidity and mortality and is associated with target organ damage, including CKD due to low awareness, poor treatment, and low control of high BP, especially in African countries [40,41]. However, there is a dearth of relevant data illustrating the prevalence and contributing factors of chronic kidney disease (CKD) among hypertensive individuals in Ethiopia.
Chronic kidney disease is associated with several consequences, including anemia, bone and mineral disorders, electrolyte imbalance, acid-base abnormalities, sexual dysfunction, hypertension, cardiovascular diseases [9]. Renal anemia, issues with bone metabolism, and electrolyte imbalances are some of the systemic consequences of end-stage renal disease (ESRD), which is caused by diabetic kidney disease and lowers quality of life. People with diabetes with chronic kidney disease usually receive comprehensive therapy for hyperglycemia, hypertension, dyslipidemia, and healthy lifestyle choices [42,43].
The pooled prevalence of CKD among hypertension patients in Ethiopia was 21% (95% CI: 18–24) in this systematic review and meta-analysis, with notable variation among the studies. The result is relatively low when compared to the systematic review and meta- analysis on global burden of CKD among hypertensive patients (34.97%) [6]. This differences could be caused by variations in the sample size, demographics, diabetes, chronic kidney failure classification, and clinical features [44].
Another analysis of systematic review on the burden of CKD among hypertensive patients in Africa found that the pooled prevalence was 17.8%, which was in line with the result of the present systematic review and meta-analysis [40].
The present study revealed that age ≥ 60 years’ leads to a two times greater likelihood of developing CKD than age < 60 years among hypertensive patients. This finding is supported by previous study conducted in Nigeria [15]. This might be due to the nature as the age increase, the function of the kidney decreases. In order to address the growing problem of chronic kidney disease, our results advise physicians to improve hypertension treatment programs. Additionally, screening in this highly focused demographic may help identify the people who would most benefit from changing lifestyle changes associated with the development of diabetic chronic kidney disease (CKD), especially in its early stages.
The present study showed that uncontrolled hypertension was a strong predictor of CKD in patients with hypertension. That is patients who had not control their hypertension 4.65 times more likely to develop CKD than their counter parts. The result is consistent with previous systematic reviews and meta-analyses study on progression of chronic kidney disease: the role of blood pressure control, proteinuria, and angiotensin-converting enzyme inhibition: a patient-level meta-analysis that deals uncontrolled hypertension is associated with a higher risk for kidney disease progression [45]. Evidence also supports that early treatment of hypertension is important in preventing cardiovascular disease and the progression of hypertensive renal disease and the benefit of tight blood pressure control is very crucial issue to prevent CKD. In addition, another meta-analysis study reported that hypertensive patients may benefit more from intensive BP-lowering strategies to provide protection against kidney failure events in patients with hypertension [46].
This study found that among adult hypertensive patients, a longer duration of hypertension was linked to a higher risk of developing chronic kidney disease. Specifically, patients with hypertension duration of ≥ 10 years had a nearly six-fold higher risk of developing chronic kidney disease compared to those with a shorter duration. This might be due to Alternatively put, the kidney's nephrons are supplied with a dense network of blood vessels, and the high volume of blood flow through them can cause arteries surrounding the kidney to narrow, weaken, or harden over time. Patients with increased diastolic can also cause filtration to be damaged, and persistently high blood pressure predisposes hypertensive patients to renal vascular nephropathy, which gradually degrades glomerular filtration rate and gives enough time for the development of other renal diseases. The renal tissue cannot receive enough blood flow from these damaged arteries [47].
According to this study, patients with adult hypertension patients who also had diabetes or heart failure (CHF) were four times more likely to develop chronic kidney disease than those without these co-occurring conditions. This might be due to diabetes: the sugar stays in the bloodstream rather than entering the cells if the patient generates little or no insulin, or if the body is unable to use the insulin. Elevated blood sugar levels cause small blood vessels across the body, including the kidney's filter, to worsen over time. More kidney damage results in more fluid and waste being retained in the bloodstream rather than being eliminated, and cardiac output in patients with heart issues may be low in the glomerular filtration membrane [48].
This systematic review and meta-analysis is the first study in the country and nationwide because we incorporate determinants of CKD among hypertensive patients since other studies didn’t incorporate determinants of CKD.
Limitation of the Study
This study is not without limitations, despite the fact that the review will be crucial in helping to provide recent evidence in Ethiopia. First, there were not enough research conducted in the setting, which made it impossible to perform subgroup analysis by region because no data from every region of the nation could be located. Second, this study's data was highly varied in character.
Implication of the Study
Future scholars will use this study as a reference. The results of this study have consequences for clinical work. When possible and inexpensive, estimating the burden of chronic kidney disease (CKD) among hypertension patients should probably be the first step toward renal disease prevention. Preventive programs should include advice on how to raise patients' and healthcare providers' awareness of CKD and encourage healthy lifestyle choices. Additionally, it offers data regarding the prevalence and consequences of chronic kidney failure on public health in the county, which may be taken into consideration during standard clinical patient care. Additionally, knowing the risk factors may aid medical practitioners in managing hypertension patients with chronic kidney disease (CKD) during clinical treatment.
Conclusion
The current systematic review and meta-analysis revealed that the prevalence of CKD remains high among hypertensive patients in Ethiopia based on the 4 research-based papers included in this study. Although, this study assessed risk factor associated with CKD based on the pooled analysis of the adjusted odds ratio of studies. Risk factors like uncontrolled hypertension, age ≥ 60 years, duration of hypertension >=10 years and having diabets diseases were factors significantly associated with the presence of chronic kidney disease among hypertensive patients. The findings provide a scientific basis for a further understanding of the risk factors of CKD in patients with hypertension and serve as a baseline for preventive strategies. To address CKD concerns in hypertensive populations, this review recommends certain preventive measures, such as strict blood pressure management, routine CKD screening, and patient education initiatives. Therefore, situation- based interventions and context-specific preventive strategies like supportive public health policies that emphasize access to early detection services, cost-effective treatment options, and public awareness campaigns should be developed to reduce the prevalence and risk factors of CKD among hypertensive patients.
References
- Talbert, R., Yee, G., Matzke, G., Wells, B., & Posey, L. M. (2008). Pharmacotherapy: a pathophysiologic approach. McGraw-Hill Publishing.
- Naser, A. Y., Alwafi, H., Alotaibi, B., Salawati, E., Samannodi, M., Alsairafi, Z., ... & Dairi, M. S. (2021). Prevalence of Chronic Kidney Diseases in Patients with Diabetes Mellitus in the Middle East: A Systematic Review and Metaâ? Analysis. International Journal of Endocrinology, 2021(1), 4572743.
- Eknoyan, G., Lameire, N., Eckardt, K., Kasiske, B., Wheeler, D., Levin, A., ... & Coresh, J. J. K. I. (2013). KDIGO 2012clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney int, 3(1), 5-14.
- Levey, A. S., Eckardt, K. U., Dorman, N. M., Christiansen, S. L., Hoorn, E. J., Ingelfinger, J. R., ... & Winkelmayer, W. C. (2020). Nomenclature for kidney function and disease: report of a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney international, 97(6), 1117-1129.
- Isakova, T., Nickolas, T. L., Denburg, M., Yarlagadda, S., Weiner, D. E., Gutiérrez, O. M., ... & Kramer, H. (2017). KDOQI US commentary on the 2017 KDIGO clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease–mineral and bone disorder (CKD-MBD). American Journal of Kidney Diseases, 70(6), 737-751.
- Tekalign, T., Awoke, N., Asmare, H., Teshome, M., Mesele, M., & Meskele, M. Global Burden of Chronic Kidney Disease Among Hypertensive Patient Systematic-Review and Meta- Analysis. Lielt G/Selasie and Teshome, Mistre and Mesele, Molalegn and Meskele, Mengistu, Global Burden of Chronic Kidney Disease Among Hypertensive Patient Systematic- Review and Meta-Analysis.
- Kovesdy, C. P. (2022). Epidemiology of chronic kidney disease: an update 2022. Kidney international supplements, 12(1), 7-11.
- Jager, K. J., Kovesdy, C., Langham, R., Rosenberg, M., Jha, V., & Zoccali, C. (2019). A single number for advocacy and communication—worldwide more than 850 million individuals have kidney diseases. Nephrology Dialysis Transplantation, 34(11), 1803-1805.
- Bikbov, B., Purcell, C. A., Levey, A. S., Smith, M., Abdoli,, Abebe, M., ... & Owolabi, M. O. (2020). Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The lancet, 395(10225), 709-733.
- Fenta, E. T., Eshetu, H. B., Kebede, N., Bogale, E. K., Zewdie,, Kassie, T. D., ... & Gelaw, S. S. (2023). Prevalence and predictors of chronic kidney disease among type 2 diabetic patients worldwide, systematic review and meta- analysis. Diabetology & Metabolic Syndrome, 15(1), 245.
- Saran, R., Robinson, B., Abbott, K. C., Agodoa, L. Y., Bhave,N., Bragg-Gresham, J., ... & Shahinian, V. (2018). US renal data system 2017 annual data report: epidemiology of kidney disease in the United States. American Journal of Kidney Diseases, 71(3), A7.
- Garofalo, C., Borrelli, S., Minutolo, R., Chiodini, P., De Nicola, L., & Conte, G. (2017). A systematic review and meta- analysis suggests obesity predicts onset of chronic kidney disease in the general population. Kidney international, 91(5), 1224-1235.
- Okwuonu, C. G., Chukwuonye, I. I., Adejumo, O. A., Agaba,E. I., & Ojogwu, L. I. (2017). Prevalence of chronic kidney disease and its risk factors among adults in a semi-urban community of South-East Nigeria. Nigerian Postgraduate Medical Journal, 24(2), 81-87.
- Meremo, A. J., Masalu, M. B., Sabi, I., Ngilangwa, D. P.,Kapinga, J., Tagalile, R., ... & Mwashambwa, M. Y. (2018). Prevalence and risk factors associated with chronic kidney disease among patients presenting at a haemodialysis unit in dodoma, Tanzania. East African Health Research Journal, 2(1), 53-57.
- Chukwuonye, I. I., Ogah, O. S., Anyabolu, E. N., Ohagwu,K. A., Nwabuko, O. C., Onwuchekwa, U., ... & Oviasu, E. (2018). Prevalence of chronic kidney disease in Nigeria: systematic review of population-based studies. International journal of nephrology and renovascular disease, 165-172.
- Fiseha, T., Mengesha, T., Girma, R., Kebede, E., & Gebreweld,(2019). Estimation of renal function in adult outpatientswith normal serum creatinine. BMC Research Notes, 12, 1-6.
- Ephraim, R. K., Biekpe, S., Sakyi, S. A., Adoba, P., Agbodjakey, H., & Antoh, E. O. (2015). Prevalence of chronic kidney disease among the high risk population in South- Western Ghana; a cross sectional study. Canadian journal of kidney health and disease, 2, 76.
- Adugna, T., Merga, H., & Gudina, E. K. (2018). Impaired glomerular filtration rate, high grade albuminuria and associated factors among adult patients admitted to tertiary Hospital in Ethiopia. BMC nephrology, 19, 1-11.
- Moosa, M. R., Van der Walt, I., Naicker, S., & Meyers, A. M. (2015). Important causes of chronic kidney disease in South Africa. South African medical journal, 105(4), 320-327.
- Cherng, Y. G., Lin, C. S., Shih, C. C., Hsu, Y. H., Yeh, C. C.,Hu, C. J., ... & Liao, C. C. (2018). Stroke risk and outcomes in patients with chronic kidney disease or end-stage renal disease: two nationwide studies. PloS one, 13(1), e0191155.
- Garimella, P. S., & Hirsch, A. T. (2014). Peripheral artery disease and chronic kidney disease: clinical synergy to improve outcomes. Advances in chronic kidney disease, 21(6), 460-471.
- Mohammed, E., Browne, L. D., Kumar AU, A., Adeeb, F., Fraser, A. D., & Stack, A. G. (2019). Prevalence and treatment of gout among patients with chronic kidney disease in the Irish health system: A national study. PloS one, 14(1), e0210487.
- Adejumo, O. A., Iyawe, I. O., Akinbodewa, A. A., Abolarin,O. S., & Alli, E. O. (2019). Burden, psychological well-being and quality of life of caregivers of end stage renal disease patients. Ghana medical journal, 53(3), 190-196.
- Duko, B., Erdado, M., & Ebrahim, J. (2019). Prevalence and factors associated with depression among hospital admitted patients in South Ethiopia: cross sectional study. BMC research notes, 12, 1-4.
- Tegegne, B., Demeke, T., Amme, S., Edmealem, A., & Ademe,S. (2020). Knowledge towards prevention and early detection of chronic kidney disease and associated factors among hypertensive patients at a chronic illness clinic of Jimma Town Public Hospitals. BioMed research international, 2020(1), 5969326.
- Yeo, W. S., & Ng, Q. X. (2018). Disruptive technological advances in vascular access for dialysis: an overview. Pediatric Nephrology, 33(12), 2221-2226.
- H. M. Perry, Jr., J. P. Miller, J. R. Fornoff, J. D. Baty, M. P. Sambhi, G. Rutan, et al., "Early predictors of 15-year end- stage renal disease in hypertensive patients," Hypertension, vol. 25, pp. 587-94, Apr 1995.
- AKeates, A. K., Mocumbi, A. O., Ntsekhe, M., Sliwa, K., & Stewart, S. (2017). Cardiovascular disease in Africa: epidemiological profile and challenges. Nature Reviews Cardiology, 14(5), 273-293.
- McGill Jr, H. C., McMahan, C. A., & Gidding, S. S. (2008). Preventing heart disease in the 21st century: implications of the Pathobiological Determinants of Atherosclerosis in Youth (PDAY) study. Circulation, 117(9), 1216-1227.
- Bahrey, D., Gebremedhn, G., Mariye, T., Girmay, A., Aberhe, W., Hika, A., ... & Demoz, G. T. (2019). Prevalence and associated factors of chronic kidney disease among adult hypertensive patients in Tigray teaching hospitals: a cross- sectional study. BMC research notes, 12, 1-5.
- Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche,P. C., Ioannidis, J. P., ... & Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. Bmj, 339.
- Luo, Z., Dong, X., Wang, C., Cao, W., Zheng, Y., Wu, Z.,... & Li, N. (2023). Association between socioeconomic status and adherence to fecal occult blood tests in colorectal cancer screening programs: systematic review and meta- analysis of observational studies. JMIR Public Health and Surveillance, 9(1), e48150.
- Modesti, P. A., Reboldi, G., Cappuccio, F. P., Agyemang, C., Remuzzi, G., Rapi, S., ... & ESH Working Group on CV Risk in Low Resource Settings. (2016). Panethnic differences in blood pressure in Europe: a systematic review and meta- analysis. PloS one, 11(1), e0147601.
- Huedo-Medina, T. B., Sánchez-Meca, J., Marín-Martínez, F., & Botella, J. (2006). Assessing heterogeneity in meta-analysis: Q statistic or I² index?. Psychological methods, 11(2), 193.
- Egger, M., Smith, G. D., & Altman, D. (Eds.). (2008). Systematic reviews in health care: meta-analysis in context. John Wiley & Sons.
- Kumela Goro, K., Desalegn Wolide, A., Kerga Dibaba, F., Gashe Fufa, F., Wakjira Garedow, A., Edilu Tufa, B., & Mulisa Bobasa, E. (2019). Patient awareness, prevalence, and risk factors of chronic kidney disease among diabetes mellitus and hypertensive patients at Jimma University Medical Center,Ethiopia. BioMed Research International, 2019(1), 2383508.
- Hunegnaw, A., Mekonnen, H. S., Techane, M. A., & Agegnehu, C. D. (2021). Prevalence and associated factors of chronic kidney disease among adult hypertensive patients at Northwest Amhara Referral Hospitals, Northwest Ethiopia, 2020. International Journal of Hypertension, 2021(1),5515832.
- Hailu, H. E., Dinku, B., Wondimu, J., & Girma, B. (2022). Prevalence and Associated Factors of Chronic Kidney Disease Among Diabetic and Hypertensive Patients at Ambo Town Public Hospitals of West Shewa Zone, Oromia Region, Ethiopia.
- Bahrey, D., Gebremedhn, G., Mariye, T., Girmay, A., Aberhe, W., Hika, A., ... & Demoz, G. T. (2019). Prevalence and associated factors of chronic kidney disease among adult hypertensive patients in Tigray teaching hospitals: a cross- sectional study. BMC research notes, 12, 1-5.
- Ajayi, S. O., Ekrikpo, U. E., Ekanem, A. M., Raji, Y. R., Ogah,O. S., Ojji, D. B., ... & Okpechi, I. G. (2021). Prevalence of Chronic Kidney Disease as a Marker of Hypertension Target Organ Damage in Africa: A Systematic Review and Metaâ? Analysis. International journal of hypertension, 2021(1), 7243523.
- Mills, K. T., Bundy, J. D., Kelly, T. N., Reed, J. E.,Kearney, P. M., Reynolds, K., ... & He, J. (2016). Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation, 134(6), 441-450.
- Levey, A. S., Gansevoort, R. T., Coresh, J., Inker, L. A.,Heerspink, H. L., Grams, M. E., ... & Willis, K. (2020). Change in albuminuria and GFR as end points for clinical trials in early stages of CKD: a scientific workshop sponsored by the National Kidney Foundation in collaboration with the US Food and Drug Administration and European Medicines Agency. American journal of kidney diseases, 75(1), 84-104.
- Cherney, D. Z., Bell, A., Girard, L., McFarlane, P., Moist, L., Nessim, S. J., ... & Weinstein, J. (2023). Management of type 2 diabetic kidney disease in 2022: a narrative review for specialists and primary care. Canadian Journal of Kidney Health and Disease, 10, 20543581221150556.
- Stanifer, J. W., Jing, B., Tolan, S., Helmke, N., Mukerjee, R., Naicker, S., & Patel, U. (2014). The epidemiology of chronic kidney disease in sub-Saharan Africa: a systematic review and meta-analysis. The Lancet Global Health, 2(3), e174-e181.
- Jafar, T. H., Stark, P. C., Schmid, C. H., Landa, M., Maschio,G., De Jong, P. E., ... & AIPRD Study Group*. (2003). Progression of chronic kidney disease: the role of blood pressure control, proteinuria, and angiotensin-converting enzyme inhibition: a patient-level meta-analysis. Annals of internal medicine, 139(4), 244-252.
- Coresh, J. (2017). Update on the burden of CKD. Journal of the American Society of Nephrology, 28(4), 1020-1022.
- Webster, A. C., Nagler, E. V., Morton, R. L., & Masson, P. (2017). Chronic kidney disease. The lancet, 389(10075), 1238-1252.
- Di Angelantonio, E., Chowdhury, R., Sarwar, N., Aspelund, T., Danesh, J., & Gudnason, V. (2010). Chronic kidney disease and risk of major cardiovascular disease and non-vascular mortality: prospective population based cohort study. Bmj, 341.