
Archives of Infectious Diseases & Therapy(AIDT)
ISSN: 2577-8455 | DOI: 10.33140/AIDT
Impact Factor: 1.385


Research Article - (2025) Volume 9, Issue 3
Predictors of Anaemia Among Tertiary Level Students
Received Date: Nov 12, 2025 / Accepted Date: Dec 02, 2025 / Published Date: Dec 08, 2025
Copyright: ©2025 Williams Ampadu Oduro, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Oduro, W. A., Incoom, D. E. (2025). Predictors of Anaemia Among Tertiary Level Students. Archives of Infect Diseases & Therapy, 9(3), 01-11.
Abstract
Objectives: Anaemia is a widespread public health issue that affects young adults and can impair physical and cognitive performance. This study aimed to determine the prevalence and predictors of anaemia among students of Cape Coast Technical University, with particular focus on socio-demographic, lifestyle, dietary, environmental, and hygiene-related factors.
Study Design: Cross-sectional study.
Methods: A total of 400 first-year students were recruited using purposive and random sampling. Data were collected through structured questionnaires, and haemoglobin levels were measured to determine anaemia status. Descriptive statistics were used to estimate prevalence, while multivariate analysis was conducted to identify independent predictors of anaemia.
Results: The prevalence of anaemia was 50.7%. Significant predictors included low intake of protein-rich foods (p<0.05), low BMI (p<0.01), poor handwashing practices (p<0.05), and exposure to vehicular fumes (p<0.05). Socio-demographic factors, particularly age and sex, also showed significant associations with anaemia.
Conclusions: Anaemia is a major health concern among students in this setting. Both lifestyle and environmental factors contribute to its high prevalence. Targeted interventions focusing on nutrition, health education, and environmental risk reduction are needed to lower the burden of anaemia among university students.
Keywords
Anaemia, Haemoglobin Levels, Socioeconomic Factors, Nutritional Status and University Students
Introduction
Anaemia is one of the most pervasive public health concerns that affect populations across both developed and developing countries [1]. It is characterized by a reduction in the number of red blood cells, leading to low haemoglobin levels and impaired oxygen transport within the body. Anaemia is often multifactorial, resulting from nutritional deficiencies, infections, chronic diseases, and genetic disorders [2]. Among various demographic groups, individuals with lower socioeconomic status, underweight individuals, and women residing in rural areas have been reported to experience higher anaemia prevalence [3]. The condition is often exacerbated by infections such as schistosomiasis, hookworm infestations, and malaria, especially in sub-Saharan Africa [4].
Globally, approximately 24.8% of the population suffers from anaemia, with children under six years old exhibiting the highest prevalence at 47.4%. Among adults, women have a prevalence of 39.9%, while men have a significantly lower rate of 12.7% [1]. In Ghana, the burden of anaemia is considerable, affecting 30.2% of non-pregnant women and 41.8% of pregnant women [5]. The World Health Organization (WHO) estimates that iron deficiency accounts for nearly 50% of anaemia cases worldwide [6]. However, emerging evidence suggests that in areas with high burdens of infections, iron deficiency-related anaemia is relatively lower, possibly due to inflammation-driven alterations in iron metabolism [7].
Environmental and lifestyle factors also contribute significantly to anaemia prevalence. Exposure to biomass smoke has been linked to decreased haemoglobin levels and increased risks of anaemia [8,9]. Similarly, poor sanitation, lack of clean drinking water, and open defecation have been associated with higher anaemia risks [10]. Studies indicate that households reliant on groundwater for drinking face a greater risk of anaemia, likely due to contamination and poor water quality [5]. Additionally, inadequate sanitation facilities have been found to correlate with a higher likelihood of anaemia [11]. These environmental risk factors, coupled with dietary inadequacies and lifestyle habits, contribute to the widespread occurrence of anaemia.
The consequences of anaemia extend beyond immediate health concerns. A deficiency in haemoglobin limits the blood’s ability to transport oxygen efficiently, leading to reduced physical and mental performance. In children, anaemia has been linked to cognitive impairment and developmental delays, while in adults, it results in diminished work productivity [12]. A study conducted across ten developing countries found that anaemia-related productivity losses equated to approximately 0.57% of the gross domestic product (GDP) [12]. Among students, anaemia has been associated with poor academic performance, reduced concentration, and increased fatigue, ultimately hindering educational attainment [13]. Given these significant health and socioeconomic implications, addressing anaemia is critical to improving public health outcomes and fostering national development.
Despite ongoing efforts to combat anaemia through iron fortification programs, a large segment of the reproductive- age population remains underserved. In Ghana, the majority of anaemia-related interventions target young children and pregnant women, leaving non-pregnant women and men of reproductive age largely neglected [14]. This research aims to bridge this knowledge gap by investigating the predictors of anaemia among students of Cape Coast Technical University. Understanding the specific risk factors contributing to anaemia within this population will provide valuable insights for targeted interventions. By identifying dietary, socioeconomic, environmental, and lifestyle determinants, this study will contribute to efforts aimed at reducing anaemia prevalence and improving the overall well-being of students in Ghana.
Methods
Study Setting and Design
An institution-based quantitative cross-sectional study was conducted among students at Cape Coast Technical University. Cape Coast Technical University (CCTU) is one of the leading technical universities in Ghana, located in Cape Coast in the Central Region. The university offers a range of academic programs in engineering, applied sciences, business, and technology, with the aim of equipping students with practical and technical skills. CCTU consists of multiple faculties and departments, providing a diverse learning environment. As of recent years, the university has enrolled thousands of students from different backgrounds, making it an ideal setting for studies related to public health, socio- economic factors, and environmental influences on student well- being.
Study Population
The study targeted first-year students at Cape Coast Technical University (CCTU), Ghana, who met the eligibility criteria. The focus was on individuals within the reproductive age range (15–49 years), as they are more susceptible to anaemia due to physiological and lifestyle factors.
Inclusion and Exclusion Criteria
Eligible participants were first-year students at CCTU, aged 15 to 49 years, who provided informed consent. Exclusion criteria included individuals outside this age range, those who declined participation, and individuals with sickle cell traits (HbAS and HbSS).
Sample Size Determination and Sampling Techniques
This study purposively selected first-year students as the target population. The sample size was determined using the Cochrane formula for cross-sectional studies [15]:
where P is the estimated prevalence of anaemia (40%), Zα/2 represents the critical value at a 95% confidence level (1.96), and d is the margin of error (5%). Based on this formula, the required sample size was 369. To account for potential missing data, the final sample size was increased to 400. Participants were selected using simple random sampling, ensuring that only individuals meeting the inclusion criteria were enrolled in the study.
Data collection
Questionnaire-Based Data Collection
Data on socio-demographic characteristics including age, sex, marital status, residence, house ownership, socio-economic characteristics, lifestyle and dietary habits, exposure to smoke, and sanitation and hygiene practices were collected using a structured questionnaire. The questionnaire was administered with the assistance of two research assistants, and participants completed it in person, over the phone, or via Google Forms. Clarifications were provided when necessary. Additionally, anthropometric measurements were taken by a trained technician, including weight (measured to the nearest 1 kg using a calibrated scale) and height (measured to the nearest 1 cm using a stadiometer). Body mass index (BMI) was subsequently calculated and recorded.
Blood Sample Collection and Hemoglobin Measurement
After obtaining informed consent, blood samples were collected using standard venipuncture procedures. The venipuncture site was cleaned with 70% ethanol and allowed to air-dry before a sterile needle was used to draw 2 mL of venous blood. The sample was then collected into an EDTA tube to prevent coagulation. To ensure accurate hemoglobin measurement, the sample was gently mixed by inverting the EDTA tube several times. Hemoglobin concentration was analyzed using a calibrated hematology analyzer, following standard laboratory protocols.
Data Processing and Analysis
For the quantitative study, the data collected was inspected, categorized and transported into Excel, and finally into STATA version 16 to be analyzed. Descriptive statistics such as tables, bar graphs, pie chart were used to give a detailed description of key characteristics of subjects and evaluate the widespread predictive factors of anaemia. Frequencies, percentages, mean and standard deviation (SD) were calculated and presented in the form of a frequency distribution table. Pearson-Chi Square analysis and logistic regression analysis was used to investigate the association between independent variables and the dependent variable, which is anaemia. With a p-value of <0.05 the statistical significance was determined, and the Multivariate logistic regression model was used to pinpoint the independent predictors of anaemia.
Quality Control and Pretesting of The Questionnaire
A pilot study with 20 second-year students assessed the clarity and reliability of the interview guides, leading to necessary revisions before data collection. Research assistants received training on study objectives, data collection, and ethics to ensure consistency, reduce bias, and enhance data quality. A qualified laboratory technician from the school’s health facility collected and analyzed blood samples using standard venipuncture procedures. Hemoglobin concentration was measured with a calibrated hematology analyzer for accuracy and reliability.
Ethical Considerations
Ethical approval for the study was obtained from the Ghana Health Service Ethics Review Committee with the approval number GHS-ERC:019/12/22. Permission was also sought from the head of the institution before the commencement of the study. All participants provided written informed consent after being fully briefed on the study’s objectives, confidentiality measures, and their right to withdraw at any stage without consequences. Students diagnosed with anaemia or testing positive for stool- related infections were referred to the university’s health facilities for further evaluation and treatment, with the associated costs covered by the investigators.
Results
Socioeconomic Characteristics of The Students
The socio-demographic data in Table 1 below showed that most respondents were male (52.5%) and between the ages of 20 and 24 (62.7%). The majority were single (95.75%) and lived in urban areas (42%). Additionally, 62% owned their homes, while 36% rented their accommodations. Household characteristics indicated that 40.3% of respondents lived in houses with more than five rooms, and 77% had up to two children per household. Common household appliances included televisions (89%), refrigerators (85.3%), and computers (68.5%). In terms of lifestyle, 31.3% of respondents did not engage in physical activity, while only 6.8% participated in vigorous exercise. Fish and seafood were widely consumed, with 67.5% eating them daily. BMI analysis showed that 11.3% of respondents were underweight, 16% were overweight, and 8% were classified as obese. Regarding access to basic amenities, 64% of respondents had access to potable drinking water, while 86.5% used improved toilet facilities. Smoking was uncommon, with only 0.8% of respondents identifying as smokers.
|
Characteristics |
Frequency (%) |
|
Sex |
|
|
Male |
210 (52.5%) |
|
Female |
190 (47.5%) |
|
Age in years |
|
|
15-19 |
16 (4%) |
|
20-24 |
251 (62.7%) |
|
25-29 |
99 (24.8%) |
|
30-34 |
24 (6%) |
|
>35 |
10 (2.5%) |
|
Marital Status |
|
|
Single/Never married |
381 (95.75%) |
|
Married/living together |
14 (3.5%) |
|
Divorced/Separated |
3 (0.75%) |
|
Residence |
|
|
Urban |
168 (42%) |
|
Peri-urban |
132 (33%) |
|
Rural |
100 (25%) |
|
House ownership |
|
|
Own house |
248 (62%) |
|
Rented/leased house |
144 (36%) |
|
Borrowed house |
7 (1.8%) |
|
Others |
1 (0.3%) |
|
Number of children per |
|
|
house |
310 (77%) |
|
≤ 2 |
90 (23%) |
|
≥ 2 |
|
|
Number of rooms per |
|
|
house |
78 (19.5%) |
|
≤ 2 |
159 (39.8%) |
|
3-4 |
161 (40.3%) |
|
≥ 5 |
|
|
Household Appliances |
|
|
Refrigerator |
341 (85.3%) |
|
Television |
356 (89%) |
|
Bicycle |
143 (35.8%) |
|
Bus /truck/car |
146 (36.5%) |
|
Electric generator |
53 (13.3%) |
|
Washing machine |
83 (20.8%) |
|
Computer |
274 (68.5%) |
|
Physical activity |
|
|
No activity |
125 (31.3%) |
|
Light activity |
95 (23.8%) |
|
Moderate Activity |
54 (13.5%) |
|
Vigorous activity |
27 (6.8%) |
|
Protein-rich meals |
|
|
Organ meat intake |
|
|
Day |
17 (4.3%) |
|
Within the week |
17 (4.3%) |
|
Flesh meat intake |
|
|
Day |
157 (39.3%) |
|
Within the week |
159 (38.8%) |
|
Fish and seafood intake |
|
|
Day |
270 (67.5%) |
|
Within the week |
349 (87%) |
|
Body mass index (BMI) |
|
|
kg/m² |
44 (11.3%) |
|
Underweight (<18.5) |
251 (64.7%) |
|
Normal weight (18.5-24.9) |
62 (16%) |
|
Overweight (25-29.9) |
31 (8%) |
|
Obese (≥ 30) |
|
|
Drinking water |
|
|
Portable drinking water |
256 (64%) |
|
No access to portable |
106 (26.3%) |
|
drinking water |
|
|
Toilet facility Access to improved toilet facility No access to improved toilet facility |
346 (86.5%)
54 (13.5%) |
|
Cigarette smoking |
|
|
Smoker |
3 (0.8%) |
|
Non-smoker |
397 (99.2%) |
|
Vehicular Fumes exposure |
|
|
Yes |
108 (27%) |
|
No |
292 (73%) |
|
Cooking Fuel |
|
|
Little/ no smoke |
220 (55%) |
|
Moderate smoke |
136 (34%) |
|
High smoke |
56 (14%) |
|
Haemoglobin g/dl |
|
|
(Males) |
|
|
<13 |
77 (37%) |
|
≥13 |
131(62.4%) |
|
(Females) |
|
|
<12 |
123 (64.7%) |
|
≥12 |
66 (34.7%) |
Table 1: Socio-Demographic Information of Responders (n=400)
Descriptive Statistics of Respondents’ Demographic and Health Characteristics
Table 2 shows that respondents’ ages ranged from 18 to 48 years, with an average age of 24.06 years. The mean weight and height were 63.15 kg and 165.90 cm, respectively. Haemoglobin levels varied, with an average of 12.52 g/dL. Household sizes also differed, with respondents having an average of 4.2 rooms and 1.45 children per household.
|
|
Minimum |
Maximum |
Mean |
Std. Deviation |
|
Age of respondent |
18 |
48 |
24.06 |
4.014 |
|
Weight of respondent |
38.0 |
163.0 |
63.148 |
13.5862 |
|
Height of respondent |
13.3 |
190.0 |
165.902 |
11.6728 |
|
Haemoglobin (Hb) of respondent |
7.0 |
19.0 |
12.519 |
1.8689 |
|
The number of rooms in the respondent`s house |
1 |
15 |
4.20 |
2.056 |
|
The number of children in the respondent’s household |
0 |
10 |
1.45 |
1.554 |
Table 2: Mean Analysis of Demographics (n=400)
Prevalence of Anemia Among Students of Cape Coast Technical University
Fig 1 shows that 50.7% of respondents had anemia (203), while 49.3% (197) did not. Fig 2 indicates that most anemia cases were mild (27.5%), followed by moderate (21.7%) and severe (1.5%).

Figure 1: Prevalence of Anemia Among Students at Cape Coast Technical University
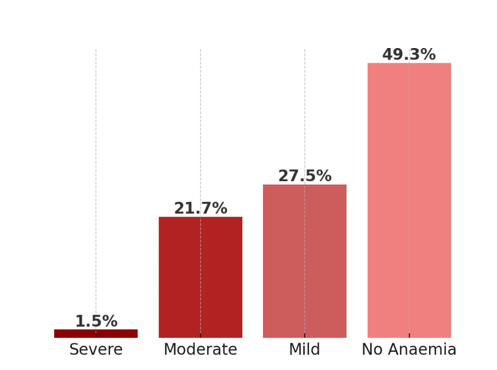
Figure 2: Distribution of Anemia Severity Among Students at Cape Coast Technical University
Predictive Factors Associated with Anaemia Among Students of Cape Coast Technical University
Table 3 below indicates that anaemia prevalence was notably high among respondents aged 20–29 years, with a significant association between age and anaemia (p<0.001, CI=95%). Female respondents had a higher prevalence (65.1%) compared to males (37%), and sex was significantly associated with anaemia (p<0.05, CI=95%). Housing conditions influenced anaemia rates, with respondents living in rented houses (53.9%) and those in smaller households (less than four rooms) showing higher prevalence. Households with more than two children also had increased anaemia cases. Lifestyle factors played a role, as respondents who engaged in no physical activity had significantly higher anaemia prevalence (66.7%, p<0.05). Among dietary factors, flesh meat consumption showed a significant association with anaemia (p=0.018, CI=95%), though no protein-rich diet exceeded a 50% anaemia prevalence. BMI was a significant factor, with underweight respondents (59.1%) and obese individuals (53.3%) having higher anaemia rates (p=0.007, CI=95%). Environmental exposures influenced anaemia prevalence. Smoking was significantly associated with anaemia, with 66.7% of smokers affected. Proximity to major roads also had a notable impact (p=0.03, CI=95%), with 59.3% of exposed individuals having anaemia. However, exposure to different levels of pollution from fuel showed no significant association with anaemia.
|
Characteristics |
Socio -economic factors |
|
|
|
|
|
Non-anaemic |
Anaemic |
X² |
p-value |
|
Age in years** |
|
|
|
|
|
15-19 |
9 (56.3%) |
7 (43.8%) |
7.767 |
.021 |
|
20-24 |
119 (47.8%) |
130 (52.2%) |
|
|
|
25-29 |
45 (45.9%) |
53 (54.1%) |
|
|
|
30-34 |
18 (75%) |
6 (25%) |
|
|
|
≥35 |
6 (60%) |
4 (40%) |
|
|
|
Sex** |
|
|
|
|
|
Male |
131 (63.0%) |
77 (37%) |
31.189 |
0.000 |
|
Female |
66 (34.9%) |
123 (65.1%) |
|
|
|
Residence** |
|
|
|
|
|
Urban |
79 (48.2%) |
85 (51.8%) |
1.357 |
.716 |
|
Peri-urban |
67 (50%) |
67 (50%) |
|
|
|
Rural |
52 (52%) |
48 (48%) |
|
|
|
House ownership |
|
|
|
|
|
Own house |
126 (50.8%) |
122 (49.2%) |
3.186 |
.364 |
|
Rented house |
122 (64.1%) |
76 (53.9%) |
|
|
|
Borrowed house |
5 (71.4%) |
2 (28.6%) |
|
|
|
Number of rooms per |
|
|
|
|
|
house** |
|
|
|
|
|
|
37 (48.7%) |
39 (51.3%) |
1.993 |
.369 |
|
< 2 |
73 (45.9%) |
86 (54.1%) |
|
|
|
3-4 |
86 (53.8%) |
74 (46.3%) |
|
|
|
>5 |
|
|
|
|
|
Number of children per |
|
|
|
|
|
Household |
|
|
|
|
|
|
154 (50%) |
154 (50%) |
4.863 |
.182 |
|
<2 |
42(48.3%) |
45 (51.7%) |
|
|
|
≥ 2 |
|
|
|
|
|
Household Appliances |
|
|
|
|
|
Refrigerator |
170 (50.1%) |
169 (49.9%) |
1.419 |
.492 |
|
Television |
170 (48%) |
184 (52%) |
|
|
|
Bicycle |
75 (52.4%) |
68 (47.6%) |
|
|
|
Bus /truck/car |
68 (46.9%) |
77 (53.1%) |
|
|
|
Electric generator |
27 (50.9%) |
26 (49.1%) |
|
|
|
Washing machine |
40 (48.2%) |
43 (51.8%) |
|
|
|
Computer |
140 (51.3%) |
133 (48.7%) |
|
|
|
Characteristics |
Lifestyle and dietary factors |
|||
|
9 (56.3%) |
Non-anaemic |
Anaemic |
X² |
p-value |
|
Physical activity |
|
|
|
|
|
No activity |
41 (33.3%) |
82 (66.7%) |
19.1554 |
.000 |
|
Light activity |
61 (64.2%) |
34 (35.8%) |
|
|
|
Moderate Activity |
28 (51.9%) |
26 (48.1%) |
|
|
|
Vigorous activity |
19 (70.4%) |
8 (29.6%) |
|
|
|
Protein-Rich Diet |
|
|
|
|
|
(Organ meat intake) |
|
|
|
|
|
Day |
13 (76.5%) |
4 (23.5%) |
5.357 |
.069 |
|
Within the week |
10 (58.8%) |
7 (41.2%) |
.602 |
.438 |
|
(Flesh meat intake) |
|
|
|
|
|
Day |
91 (58.3%) |
65 (41.7%) |
8.421 |
.015 |
|
Within the week |
94 (59.5%) |
64 (40.5%) |
12.089 |
0.002 |
|
(Fish and seafood intake) |
|
|
|
|
|
Day |
143 (53.4%) |
125 (46.6%) |
4.728 |
.193 |
|
Within the week |
175 (50.6%) |
171 (49.4%) |
3.133 |
.679 |
|
Body mass index(BMI) kg/ |
|
|
|
|
|
m² ** |
|
|
|
|
|
Underweight (<18.5) |
18 (40.9%) |
26 (59.1%) |
|
|
|
Normal weight (18.5-24.9) |
125 (50%) |
125 (50%) |
2.610 |
.456 |
|
Overweight (25-29.9) |
35 (56.5%) |
27 (43.5%) |
|
|
|
Obese(≥ 30) |
14 (46.7%) |
16 (53.3%) |
|
|
|
Characteristics |
Hygienic and sanitary factors |
|
|
|
|
7 (43.8%) |
Non-anaemic |
Anaemic |
X² |
p-value |
|
Hand washing |
|
|
|
|
|
Never |
4 (50%) |
4 (50%) |
18.248 |
0.032 |
|
Sometimes |
66 (56.9%) |
50 (43.1%) |
|
|
|
Often |
75 (51.7%) |
70 (48.3%) |
|
|
|
Always |
52 (40.6%) |
76 (59.4%) |
|
|
|
Drinking water |
|
|
|
|
|
Portable drinking water |
67 (47.2%) |
75 (52.8%) |
.526 |
.468 |
|
No access to portable water |
130 (51%) |
125 (49%) |
|
|
|
Toilet facility |
|
|
|
|
|
Access to improved toilet |
165 (48%) |
179 (52%) |
0.574 |
.902 |
|
facility |
32 (60.4%) |
21 (39.6%) |
|
|
|
No access to improved |
|
|
|
|
|
toilet facility |
|
|
|
|
|
Use of insecticide mosquito |
|
|
|
|
|
net |
42 (55.3%) |
34 (44.7%) |
1.196 |
0.32 |
|
Yes |
155 (48.3%) |
166 (51.7%) |
|
|
|
No |
|
|
|
|
|
Characteristics |
Smoke exposure |
|
|
|
|
.021 |
Non-anaemic |
Anaemic |
X² |
p-value |
|
Smoking (cigarette) habits |
|
|
|
|
|
Smoker |
2 (66.7%) |
2.320 |
.501 |
|
|
Non-smoker |
198 (50.4%) |
|
|
Table 4: Correlation Between Predictive Factors and Anaemia Among Students of Cape Coast Technical University(N=400)
Discussion
This study assessed the prevalence of anaemia among students at Cape Coast Technical University and examined its association with various socio-economic, environmental, and lifestyle factors. The findings provide valuable insight into the burden of anaemia within this population and highlight key determinants that may inform targeted interventions.
The prevalence of anaemia in this study was 50.7%, which classifies it as a severe public health problem according to WHO standards [16]. Similar trends have also been observed in other tertiary institutions in Ghana and sub-Saharan Africa. For instance, a study by Amoaning et al. [17] reported that anaemia prevalence among tertiary students in Ghana increased from 20% at the beginning of the first semester to 45.1% by the latter part of the second semester. Additionally, research conducted among university students in Nigeria found an anaemia prevalence of 20.6% [18], while a study in Ethiopia reported a prevalence of 13.5% among female students in a health science college [19]. These findings suggest that anaemia is not only a localized issue but also a broader regional concern, necessitating targeted nutritional and health interventions among students. Moreover, Berhe et al. [20] attributed the variations in anaemia prevalence to differences in economic status, socio-cultural practices, and dietary habits.
Our study also found that the prevalence of anaemia was higher among females than males, a trend consistent with previous research [18, 21, 22]. The higher susceptibility of females to anaemia may be attributed to menstrual blood loss and other obstetric-related conditions [16]. A study by Fiorentino [23] further revealed that anaemia among female students could lead to increased morbidity, absenteeism, impaired cognition, and lower academic achievement.
Socio-economic factors also emerged as significant determinants of anaemia, with students from lower-income households being more vulnerable. This aligns with findings from a study in Ethiopia, where Swaminathan et al. [24] reported that individuals from economically disadvantaged backgrounds had a higher prevalence of anaemia due to limited access to nutrient-rich foods. Furthermore, parental education levels played a crucial role, as students whose parents had attained higher education were less likely to be anaemic. H.J. et al. [25] found that children of more educated mothers had significantly higher iron intake from animal sources (P = 0.0012), which was reflected in their greater consumption of meat, poultry, and related products (P < 0.0001). This ultimately led to improved haemoglobin levels among children.
Exposure to smoke from biomass fuel and cigarette smoke was also associated with an increased risk of anaemia. This finding is supported by Appiah-Dwomoh et al. [26] in Ghana, who reported that prolonged exposure to household air pollution, including smoke from cigarettes and biomass fuel, significantly increased the risk of anaemia due to chronic inflammation and impaired iron metabolism. They further indicated that living close to a major road, involvement in fish smoking, and exposure to other environmental smoke sources were also linked to haemoglobin levels. Additionally, a study conducted in Nepal by Dinas et al. [27] established a positive correlation between second-hand smoke exposure and reduced haemoglobin levels, reinforcing the association observed in the present study. These findings highlight the need for awareness campaigns on the health risks of smoke exposure and the implementation of smoke-free policies in student living environments.
This study also examined the intake of protein-rich foods, including organ meat, flesh meat, and fish/seafood, among students and compared the findings to existing literature on dietary diversity and micronutrient adequacy. Although a high proportion of participants incorporated protein-rich foods into their diet, a significant number had low intake frequencies. This variation in consumption patterns may have implications for overall dietary diversity and micronutrient sufficiency. Contrary to these findings, a study by Isabirye et al. [28] reported that a significant proportion of adolescents had high consumption of fats, oils, and beverages while exhibiting low intake of animal-source foods, micronutrient- rich fruits, and vegetables. Moreover, their study also revealed that individuals with low consumption of protein-rich foods and dietary fibre were more likely to belong to low socio-economic households. Furthermore, research by Channar et al. [29] indicated that meal frequency played a critical role, as students who frequently skipped meals especially breakfast due to economic constraints had a higher likelihood of being anaemic. Similarly, Heo et al. [30] found a strong association between meal skipping and lower haemoglobin levels. These findings emphasize the need for nutritional education and awareness programs in tertiary institutions to promote healthy eating habits among students.
Sanitation and hygiene practices also contributed to the prevalence of anaemia. The study observed that students who frequently experienced infections such as diarrhoea and parasitic infestations had a higher prevalence of anaemia. Our findings align with research by Chanimbe et al. [31], which demonstrated that individuals with access to basic sanitation facilities had a lower likelihood of developing anaemia. Furthermore, this association remained significant even after adjusting for potential confounders, including individual and household-level characteristics, as well as country-level influences.
Moreover, our study revealed a significant association between anaemia and access to sanitation facilities. Students living in environments with poor sanitation were more susceptible to anaemia due to frequent infections that impair nutrient absorption. These findings align with research by Coffey et al. [32], which empirically examined the hypothesis that poor sanitation is a major contributor to low haemoglobin levels and anaemia in children. Their study emphasized the impact of open defecation on anaemia prevalence and highlighted the broader implications of inadequate sanitation on health and human capital outcomes.
Conclusion
This study demonstrates that anaemia is a significant public health concern among students of Cape Coast Technical University, with a prevalence of 50.7%. The condition was strongly associated with female sex, younger age, inadequate intake of protein-rich foods, low body mass index, limited physical activity, poor hand hygiene, and exposure to vehicular emissions. These findings suggest that both nutritional and environmental factors contribute to the burden of anaemia in this population. Addressing these determinants through targeted interventions, such as promoting balanced diets, improving hygiene practices, and mitigating exposure to environmental pollutants, could play a vital role in reducing anaemia and enhancing student health and academic performance.
What This Study Adds
• The study found that anaemia is highly prevalent among university students, with more than half of those surveyed affected, making it a serious public health concern.
• It reveals that anaemia in this population is influenced not only by diet and gender but also by broader socio-economic and environmental factors such as sanitation and smoke exposure.
• These findings suggest that addressing anaemia among students will require more than just nutrition-focused interventions, calling for a combination of health education, improved living conditions, and targeted support for vulnerable groups.
Implications for Policy and Practice
• Universities should implement targeted health and nutrition programs, especially for female students and those from low- income backgrounds, to reduce the burden of anaemia. This could include dietary counselling, affordable access to iron-rich meals on campus, and periodic health screenings.
• Policy makers and university health services need to prioritize awareness campaigns on the risks of anaemia and promote healthy lifestyle practices, including physical activity, handwashing, and safe living environments that limit exposure to pollutants.
• Collaboration between higher education institutions, the Ministry of Health, and non-governmental organizations is essential to integrate anaemia prevention and management into broader student health policies, ensuring sustainable support systems.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Ghana Health Service Ethics Review Committee (GHS-ERC) prior to the commencement of the study [approval number: GHS-ERC:019/12/22]. Permission to conduct the research was granted by the Ga South Health Directorate. Informed consent was obtained from all participants, with confidentiality assured. For those unable to read the consent form, it was explained in the presence of an impartial witness. Participants’ questions were answered, and those willing to participate signed or thumb printed the consent form.
Authors Contribution Statement
DEI conceived and designed the study. DEI and WAO were responsible for data curation and analysis. WAO prepared the first draft of the manuscript with input from DEI. Both authors contributed to the drafting and critical revision of the manuscript, and approved the final version for submission.
Funding
The study was self-funded
Declaration of Competing Interest
The authors declare that they have no known financial or non- financial competing interests that could have influenced the work reported in this paper.
Acknowledgements
The authors express their gratitude to the staff of Cape Coast Technical University Hospital, research assistants, and volunteers for their valuable contributions to the successful completion of the study.
References
- McLean, E., Cogswell, M., Egli, I., Wojdyla, D., & De Benoist, B. (2009). Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993– 2005. Public Health Nutrition, 12(4), 444–454.
- Kassebaum, N. J., Jasrasaria, R., Naghavi, M., Wulf, S. K., Johns, N., et al. (2014). A systematic analysis of global anemia burden from 1990 to 2010. Blood, 123(5), 615–624.
- Sadeghian, M., Fatourechi, A., & Lesanpezeshki, M. (2013). Prevalence of anemia and correlated factors in women of reproductive age in rural areas of Tabas. Journal of Family & Reproductive Health, 7(3), 139–144.
- Gebremedhin, S., & Enquselassie, F. (2011). Correlates of anemia among women of reproductive age in Ethiopia: Evidence from the Ethiopian DHS 2005. Ethiopian Journal of Health Development, 25(1), 22–30.
- Ghana Statistical Service, Ghana Health Service, & ICF International. (2015). Ghana demographic and health survey 2014. GSS, GHS, & ICF International.
- De Benoist, B., & McLean, E. (2008). Worldwide prevalence of anaemia 1993–2005: WHO global database on anaemia. World Health Organization.
- Petry, N., Olofin, I., Hurrell, R. F., Boy, E., Wirth, J. P., et al. (2016). The proportion of anemia associated with iron deficiency in low, medium, and high human development index countries: A systematic analysis of national surveys. Nutrients, 8(11), 693.
- Mishra, V., & Retherford, R. D. (2007). Does biofuel smoke contribute to anaemia and stunting in early childhood? International Journal of Epidemiology, 36(1), 117–129.
- Armo-Annor, D., Colecraft, E. K., Adu-Afarwuah, S., Christian, A. K., & Jones, A. D. (2021). Risk of anaemia among women engaged in biomass-based fish smoking as their primary livelihood in the central region of Ghana: A comparative cross-sectional study. BMC Nutrition, 7(1), 4.
- Gautam, S., Min, H., Kim, H., & Jeong, H.-S. (2019). Determining factors for the prevalence of anemia in women of reproductive age in Nepal: Evidence from recent national survey data. PLOS ONE, 14(6), e0218288.
- Harding, K. L., Aguayo, V. M., Namirembe, G., & Webb, P. (2018). Determinants of anemia among women and children in Nepal and Pakistan: An analysis of recent national survey data. Maternal & Child Nutrition, 14(2), e12478.
- Horton, S., & Ross, J. (2003). The economics of iron deficiency. Food Policy, 28(1), 51–75.
- Ukkirapandian, K., Natarajan, N., Prassanaraghavan, K., Mohan, P., & Selvam, L. (2014). Iron deficiency anaemia and cognitive function among undergraduate paramedical students. International Journal of Medical Science and Public Health, 3(6), 1–5.
- Commey, J. O., & Dekyem, P. (1995). Childhood deaths from anaemia in Accra, Ghana. West African Journal of Medicine, 14(2), 101–104.
- Cochran, W. G. (1977). The estimation of sample size in experiments: II. Using comparisons of proportions. Dental Research Journal, 32(5), 606–612.
- World Health Organization. (2015). The global prevalence of anaemia in 2011. WHO.
- Amoaning, R., Frempong, M. T., Osei, M., Amoako-Atta, K., Owusu, A., et al. (2022). Anaemia prevalence and associated factors among tertiary students in Ghana. Journal of Public Health Research, 11(4), 22799036221128642.
- Ayele, B. H., Taye, B. W., & Ayele, M. B. (2019). Prevalence of anaemia and associated factors among university students in Nigeria. International Journal of Africa Nursing Sciences, 11, 100167.
- Hussen, H., Wondim, A., & Melaku, T. (2023). Anaemia and associated factors among female students of health science colleges in Ethiopia. BMC Hematology, 23, 5.
- Berhe, K., Fseha, B., & Gebremariam, A. (2022). Variation in anaemia prevalence across sub-Saharan Africa: A review of economic, cultural, and dietary factors. African Health Sciences, 22(3), 1–12.
- Al-Alimi, A. A., Bashanfer, S., & Morish, M. A. (2018). Prevalence of iron deficiency anaemia among university students in Hodeida Province, Yemen. Anemia, 2018, 4157876.
- K. R., Arlappa, N., Venkaiah, K., & Brahmam, G. N. V. (2016). Prevalence of anaemia among adult men in India: A nationally representative cross-sectional study. Journal of Postgraduate Medicine, 62(4), 252–258.
- Fiorentino, M., Perignon, M., Kuong, K., Burja, K., Parker, M., et al. (2018). Anaemia among female students: Impact on cognition and academic performance. Nutrients, 10(8), 997.
- Swaminathan, S., Thomas, T., & Kurpad, A. V. (2019). Poverty, diet quality, and anaemia in developing countries. Food & Nutrition Bulletin, 40(2), 180–188.
- H. J. F., Allen, L. H., Correa, A., Black, A. K., & Perrine, C. G. (2011). Maternal education and dietary intake: Relationship with haemoglobin levels among children. Journal of Nutrition, 141(3), 453–459.
- Appiah-Dwomoh, E. K., Armo-Annor, R., Adjei-Mensah, E., & Kusi-Mensah, A. (2024). Household air pollution and anaemia risk in Ghana: Evidence from exposure to biomass and cigarette smoke. Environmental Science and Pollution Research, 31(2), 2345–2355.
- Dinas, P. C., Fadelu, T., & Bhandari, G. P. (2014). Second- hand smoke exposure and haemoglobin levels in Nepal: Evidence from a population-based study. BMC Public Health, 14, 1279.
- Isabirye, N., Atukunda, P., Ssentongo, R., & Mupere, E. (2020). Dietary diversity and anaemia among adolescents in sub-Saharan Africa. Journal of Health, Population and Nutrition, 39, 1–9.
- Channar, P. A., Mangi, R. A., Shahani, N., & Raza, S.H. (2023). Meal frequency, dietary habits, and anaemia prevalence among university students. Cureus, 15(6), e40872.
- Heo, M., Kim, R., Wylie-Rosett, J., Allison, D. B., Heymsfield,S. B., et al. (2021). Meal skipping and anaemia risk: Evidence from university populations. British Journal of Nutrition, 126(5), 745–752.
- Chanimbe, F., Mugisha, J., Habumugisha, T., Ndayambaje, E., & Tuyisenge, G. (2023). Access to sanitation and its association with anaemia in sub-Saharan Africa: A multi- country study. Tropical Medicine & International Health, 28(3), 212–221.
- Coffey, D., Geruso, M., & Spears, D. (2018). Sanitation, open defecation, and anaemia: Empirical evidence from India. Economics & Human Biology, 29, 25–38.