
International Journal of Endocrinology Research and Reviews(IJERR)
ISSN: 2993-656X | DOI: 10.33140/IJERR

Case Report - (2024) Volume 4, Issue 1
Postural Hypotension in a Patient with Spinal Canal Stenosis
Received Date: Jan 08, 2024 / Accepted Date: Jan 31, 2024 / Published Date: Feb 08, 2024
Copyright: ©©2024 Shahid Farooq. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Farooq, S. (2024). Postural Hypotension in a Patient with Spinal Canal Stenosis. Int J Endo Res & Rev, 4(1), 01-07.
Abstract
This case involves an elderly patient with a history of prostate cancer who was admitted to the hospital with a lower respiratory tract infection. Following recovery, he experienced recurrent falls due to a postural drop. Despite regular treatment and hydration, including fludrocortisone, the falls persisted. Various investigations, such as CT head, CT chest, abdomen and pelvis, transthoracic echocardiogram, HbA1c, renin-angiotensin ratio, cortisol, synacthen test, and carotid Doppler, were inconclusive and no apparent cause for the postural drop was found. However, an MRI of the entire spine revealed the presence of spinal stenosis and cauda equina without any accompanying symptoms of spinal disease. This discovery led to the diagnosis of autonomic neuropathy as the underlying cause of the patient's postural drop. The case highlights the importance of considering autonomic neuropathy in prostate cancer patients who experi- ence postural drops, even in the absence of obvious spinal disease symptoms.
Introduction
Orthostatic hypotension is defined as a drop-in blood pressure of over 20mmHg systolic or over 10mmH diastolic that occurs within 3 minutes of standing [1]. It negatively impacts the quality of life and increases the risks of falls, cardiovascular disease, depression and dementia. There are two main subtypes of orthostatic hypotension; neurogenic and no neurogenic, both result in reduced cardiac output or impaired vasoconstriction leading to a drop in blood pressure. Non-neurogenic orthostatic hypotension is caused by reduced cardiac output and/or impaired vasoconstriction without a primary autonomic disorder. On the other hand, neurogenic type typically results from inadequate vasomotor sympathetic release of norepinephrine due to autonomic dysfunction and can be associated with autonomic dysregulation of other organs including bowel and bladder dysfunction [2]. Neurogenic orthostatic hypotension is commonly reported in patients with neurological and autonomic disorders including Multiple Systems Atrophy, Parkinson’s disease and amyloidosis [3]. There are also a variety of metabolic, autoimmune, and neoplastic conditions that produce secondary neurogenic orthostatic hypotension [4]. There are multiple cases reporting neurogenic orthostatic hypotension after Spinal Cord Injury. Spinal cord injury causes orthostatic hypotension as there is a dysregulation of efferent sympathetic nerves and loss of vasoconstriction. A rarer cause of orthostatic hypotension is spinal canal stenosis, there are few published cases of patients with spinal canal stenosis resulting in orthostatic hypotension [5-7]. In this case discusses a patient with metastatic vertebral deposits from prostate cancer cause spinal canal stenosis resulting in neurogenic orthostatic hypotension.
Case Presentation
84-year-old man, retired and previously independent with a background of hypertension and prostate cancer with axial metastatic spread. He presented with a 2-week history of productive cough and recurrent falls. He reported increasing falls in 2 weeks prior to admission, falls occurred from standing or when mobilising. He didn’t report any significant preceding symptoms except a ‘funny sensation’ prior to the fall.
On examination, he is clinically euvolemic. His cardiovascular examination revealed heart sounds 1 and 2 present. His blood pressure 120/80 mmHg with a significant postural drop in systolic blood pressure (30-50mmHg drop in systolic blood pressure). There are no peripheral oedema, calves soft non-tender. Respiratory examination finding was coarse crepitation at right lung base with concomitant shortness of breath on standing. His gastrointestinal examination showed abdomen which was soft, non-tender, and presence of reducible periumbilical hernia. His full neurological did not show abnormal findings and motor, reflexes, and sensory function were intact.
His chest x-ray (see figure 1) showed right-sided consolidation in keeping with community-acquired pneumonia. Blood showed raised inflammatory markers (table 1). He received IV antibiotics and steroids for community-acquired pneumonia. CT angiogram/ CAP Note is made of metastatic bony changes already recorded and described on a bone scan from 05/10/2022. I suspect further progression of the metastatic bony deposits now. Most of the thoracic vertebra are now affected by metastatic bony disease. There are also metastatic deposits in the sternum and the ribs - already recorded on the previous bone scan. Note is made of moderate rolling hernia of the stomach. Incidental note is made of 4.4 mm across opaque stone in the calyx of the upper moiety of the left kidney
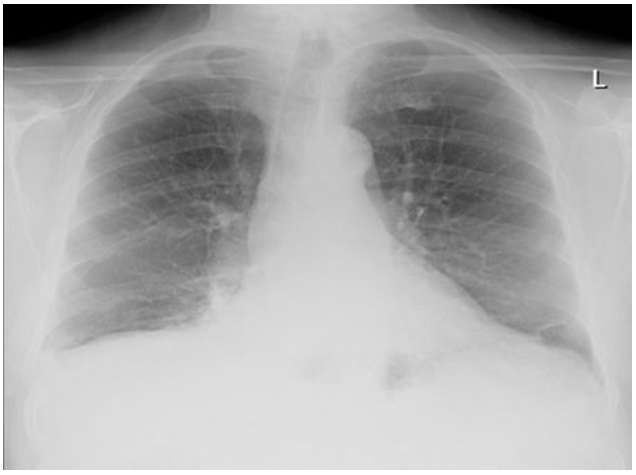
Figure 1: Chest x ray showing dense right sided consolidation in keeping with clinical examination and representing community acquired pneumonia
He completed 10 days of amoxicillin and made a full recovery from pneumonia, however, continued to be symptomatic of severe orthostatic hypotension and falls while in patient. His medications were rationalised and felodipine was stopped due to symptoms. He experiences multiple falls episodes per day, requiring assistance of 2 rendering him confined to sitting or remaining in bed. Clinical examination showed no abnormalities other than a systolic blood pressure drop of 140mmHg to 90mmHg on standing. His medications were rationalised and felodipine was stopped due to a drop-in blood pressure (table 1). Blood tests showed normal electrolyte status, thyroid function and adrenal function (table 2 and 3) Cardiovascular investigations including; Echo, ECG and Carotid Doppler showed no evidence of a cardiac cause for these events, Hba1c (table 3).
|
Admission bloods |
|
|
Parameters |
Results |
|
Hb |
118 |
|
White cell count |
15 |
|
Platelets |
298 |
|
Sodium |
138 |
|
Potassium |
3.6 |
|
Urea |
6.2 |
|
Creatinine |
93 |
|
eGFR |
>60 |
|
Bilirubin |
8 |
|
ALP |
126 |
|
ALT |
31 |
|
GGT |
72 |
|
Albumin |
30 |
|
Amylase |
17 |
|
CRP |
156 |
|
Phosphate |
0.64 |
|
Lactate |
1.9 |
|
Serum iron |
5.1 |
|
Serum ferritin |
673 |
|
Serum transferrin |
1.1 |
|
Percentage iron saturation |
19.0 |
Table 1: Blood tests on admission. Inflammatory markers raised in keeping with infection. Renal function and electrolytes within normal limits.
|
Postural hypotension investigation bloods |
|
|
Parameter |
Result |
|
Thyroid stimulating hormone |
1.1 |
|
Aldosterone |
127 |
|
Renin |
6.98 |
|
Cortisol (early morning) |
594 |
|
Adjusted calcium |
2.45 |
|
Serum phosphate |
1.13 |
|
Magnesium |
0.83 |
|
HBA1C |
47 |
Table 2: Further blood tests to investigate cause of postural hypotension. Normal thyroid function, normal adrenal function with no adrenal insufficiency. renin aldosterone ratio normal
|
Cardiac investigations |
|
|
24-hour tape |
Normal sinus rhythm, no significant ectopics |
|
ECG |
Normal sinus rhytym |
|
Ct Brain |
Normal |
|
Carotid Doppler |
Normal |
|
ECHO |
Normal |
Table 3 : Cardiac investigations to rule out cardiac disease-causing postural hypotension. No evidence of cardiac disease
Initially, non-pharmacological and lifestyle changes were trialled including, increasing oral intake, sleeping with head up and compression stockings. The patient was commenced on intravenous fluids, both fluid boluses and maintenance fluids aiming to increase the intravascular pressure however this showed little improvement. He was then commenced on fludrocortisone 100mcg. Orthostatic hypotension improved slightly however he remained symptomatic with recurrent falls, which led is to investigate further, so the dose increased to 200mcg. Despite the increased dose of fludrocortisone, as well as midodrine, which was commenced to improve his postural bp which did improve blood pressure, unfortunately, he continues to have falls. Cardiology and endocrine input were sought and advice Various investigations, such as CT head, CT tap, echo, HbA1c, renin-angiotensin ratio, cortisol, synechine test, and carotid Doppler, 24-hour tape, ECHO, were inconclusive no apparent cause for the postural drop was found except spinal metastasis on CTTAP, CTTA note is made of metastatic bony changes already recorded and described on a bone scan from 05/10/2022. I suspect further progression of the metastatic bony deposits now. Most of the thoracic vertebra are now affected by metastatic bony disease. There are also metastatic deposits in the sternum and the ribs - already recorded on the previous bone scan. Note is made of moderate rolling hernia of the stomach. Incidental note is made of 4.4 mm across opaque stone in the calyx of the upper moiety of the left kidney.
Initially, it was unclear whether the presence of spinal metastasis was the primary cause of the postural drop. However, after an MRI, it became more apparent that the level of stenosis the patient had was the main contributing factor to the postural drop. However, an MRI of the entire spine revealed the presence of spinal stenosis and cauda equina without any accompanying symptoms of spinal disease. This discovery led to the diagnosis of autonomic neuropathy as the underlying cause of the patient's postural drop
An MRI spine was performed given metastatic spread to the vertebra evident in CTAP, MRI spine (figure 3) showed T3/ T4 lesion with significant spinal canal stenosis and cauda equine impairment, with no cord compression. Neurological examination is normal, with no neurological deficit or pathology. The patient was discussed with neurosurgery and was transferred under their care for further management.
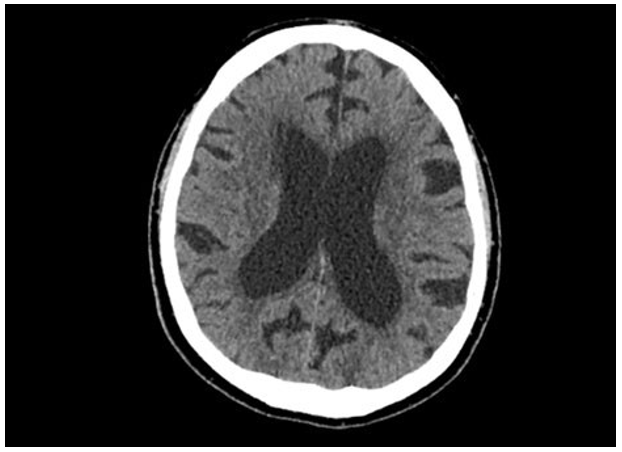
Figure 2: CT brain showing no intracranial pathology or evidence of metastatic spread CT pulmonary angiogram (20/01/23): Dense consolidation right lower dorsal and basal segment. No pulmonary embolism identified. Metastatic bony changes with progression from previous scan in 5/10/22. Most of thoracic vertebra affected by bony disease. Metastatic deposits in sternum and ribs.
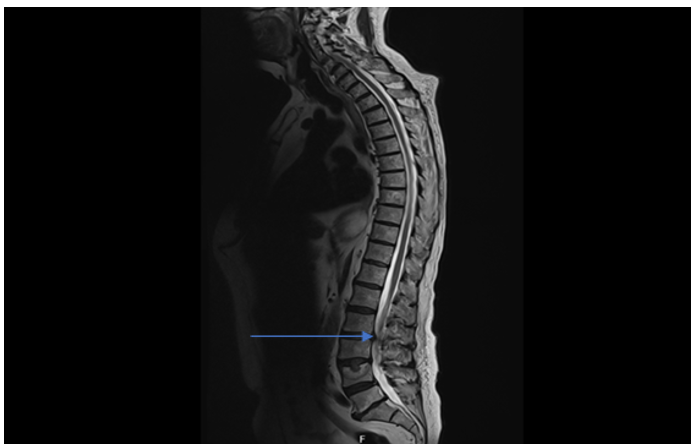
Figure 3: MRI whole spine showing metastatic deposits resulting in significant canal stenosis and impingement of cauda equine (blue arrow). Severe posterior disc protrusion at level L3/L4 causing significant canal stenosis and impinging of cauda equina with right sided predominance. Multiple marrow replacing metastatic deposits with no evidence of cord compression
Differential Diagnosis
Possible differential diagnoses for the cause of this patient’s orthostatic hypotension included; dehydration, electrolyte abnormalities, medication cardiac disease, thyroid disorders and adrenal insufficiency spinal Metastasis?
Treatment
The patient was treated with 10 days of antibiotics and hydrocortisone for community-acquired pneumonia (CURB3) according to NICE guidelines and made a full recovery from pneumonia. Initially, non-pharmacological treatments were trialled for orthostatic hypotension; increasing oral intake, compression stockings and rationalisation of medications (table 1). Patients with treated intravenous fluids both maintenance fluids and fluid bolus, showed little improvement in postural drop. He was commenced on midodrine hydrochloride 2.5mg 3 times daily initially however this showed only minor improvement in orthostatic hypotension and so was increased on a weekly basis according in line with symptoms and blood pressure up to a maximum of 10mg 3 times daily. Alongside midodrine patient was treated with fludrocortisone, initially 100mcg once daily increased to 200mcg one daily.
Outcome and Follow-Up
After a subsequent review, it was noted that James continued to experience falls as a result of a postural drop in his blood pressure. Following consultation with cardiology, as patient was started on midodrine and floourdrocortisone it was decided to stop the use of midodrine, as it is contraindicated in patients with prostate cancer and spinal stenosis according to the BNF. Additionally, his fludrocortisone was increased to the maximum dose. Although this led to a mild improvement in his blood pressure, he continued to experience postural drops when standing. Its almost 6 month he was still waiting to be seen by spinal surgeon, due to ongoing symptoms his GP made another referral to the ICAT team and an orthopaedic physiotherapist specialist. Their assessment indicated that patient had no signs or symptoms of neurological deficiency, cord signs, reflexes, clonus, or abnormal Babinski reflex. Currently, he walks with the aid of a walking aid and his main complaint is a feeling of tightness around his back, as he stands which leads to postural drops necessitating him to sit down to avoid falling. As a result, a referral was made to a spinal surgeon on an urgent basis once again. The specialists believe that all symptoms are related to spinal stenosis, which is causing the postural drop. Patient due to see spinal team in February 2024.Given all history of falls and frequent postural drop despite all treatment including Ted stocking, physio, as well fludrocortisone. This information strengthen the case that spinal stenosis was the cause of postural drop increasing risk of fall.
Discussion
In a person without spinal cord injury or spinal stenosis, certain cortical structures, particularly the insula and the hypothalamus, contribute to the autonomic regulation of cardiovascular control [8]. The medullary neurons localised within the rostral ventrolateral medullar (RVLM) are thought to be responsible for the maintenance of peripheral vascular tone and arterial blood pressure [9]. RVLM neurons normally provide tonic innervation to the sympathetic preganglionic neurons (SPN) located within the lateral horns of the spinal grey matter of the thoracic and upper lumbar spinal segments [10-12]. The axons of the SPN exit through the ventral roots and synapse on postganglionic sympathetic neurons located within the spinal prevertebral ganglia. The postganglionic neurons then send their axons within the peripheral nerves and innervate the target organs, the heart and blood vessels.
Any disruption of the descending spinal cardiovascular pathways, as a cause by spinal tenosis or spinal cord injury, will result in sympathetic hypo activity and unopposed prevalence of the intact vagal parasympathetic control [13]. Sympathetic hypo activity results in low resting blood pressure, loss of regular adaptability of blood pressure, and disturbed reflex control [14].
Postural blood pressure changes in patients with spinal stenosis can be a significant clinical manifestation of autonomic dysfunction. Spinal stenosis refers to the narrowing of the spinal canal, resulting in compression of the spinal cord and nerve roots. While it is commonly associated with symptoms such as back pain, leg pain, and weakness, postural blood pressure changes may also occur. But our patient had none of these symptoms.
Autonomic dysfunction in spinal stenosis can result from the compression of nerve structures responsible for regulating blood pressure and heart rate. The autonomic nervous system plays a crucial role in maintaining blood pressure stability during postural changes, ensuring appropriate vasoconstriction and heart rate adjustments. However, in patients with spinal stenosis, compression of nerve structures can disrupt these normal autonomic responses.
Postural blood pressure changes in patients with spinal stenosis typically involve a drop in blood pressure upon assuming an upright position, resulting in symptoms such as dizziness, light-headedness, or syncope. This can significantly impact the patient's quality of life and increase the risk of falls and related injuries.
Diagnosing autonomic dysfunction in patients with spinal stenosis and postural blood pressure changes can be challenging. Other potential causes, such as cardiovascular disorders or medication side effects, should be ruled out through thorough clinical evaluation and investigations. Imaging studies, such as MRI of the spine, are crucial in identifying spinal stenosis as the underlying cause.
Treatment for postural blood pressure changes in patients with spinal stenosis and autonomic dysfunction primarily focuses on managing the symptoms and addressing the underlying spinal pathology. This may involve a multidisciplinary approach, including physical therapy, pain management, and surgical interventions in severe cases.
In conclusion, postural blood pressure changes can occur in patients with spinal stenosis due to autonomic dysfunction resulting from compression of nerve structures. Recognizing this association is crucial in the management of these patients, as it can help guide appropriate treatment strategies and improve their overall well-being. Further research is warranted to better understand the mechanisms and optimal management of autonomic dysfunction in patients with spinal stenosis.
Learning Points/Take Home Messages 3-5 Bullet Points
1. Consider autonomic dysfunction as a cause of patient postural hypotension when other causes are not identified in initial investigations.
2. Conduct a comprehensive clinical evaluation to rule out other potential causes of postural drop in blood pressure, such as cardiovascular disorders or medication side effects. This evaluation should include a detailed medical history, physical examination, and appropriate investigations.
3. MRI is a valuable tool in identifying structural abnormalities and can help guide treatment decisions.
4. Multidisciplinary approach to treatment: Adopt a multidisciplinary approach to the management of patients with postural drop in blood pressure and spinal stenosis.
5. Symptom management lifestyle modifications, and physical therapy to improve balance and reduce the risk of falls.
6. Individualized treatment plans: Tailor treatment plans to the specific needs of each patient. The severity of spinal stenosis and the degree of autonomic dysfunction can vary among individuals, so treatment approaches should be personalized based on the patient's condition and response to interventions.
7. Long-term follow-up: Establish a long-term follow-up plan to monitor the patient's symptoms Remember, the management of postural drop in blood pressure in patients with spinal stenosis requires a comprehensive and individualized approach. Collaboration between healthcare professionals and ongoing monitoring is essential to achieve the best possible outcomes for patients.
8. In this case, the patient did not exhibit any symptoms of spinal disease, yet had metastasis. Performing an MRI of the whole spine early on could have been sufficient to identify the spinal stenosis and cauda equina caused by the metastatic spread. This would have allowed for a timely diagnosis and avoided unnecessary investigations, potentially reducing the patient's hospital stay.
Patients Perspective
Tips:
• This is an important section and gives the patient/next of kin the opportunity to comment on their experience. This enhances the case report and is strongly encouraged
• This section is written by the patient (or close family) in their own words, in the first-person. This is an opportunity for us to understand the signs and symptoms the patient experienced, their thoughts and concerns, their experience of the treatment they received, recovery and adjustment to life after or with illness or disability
• Spelling and grammar should be corrected where necessary (as per the rest of the manuscript) by the authors and non-English perspectives should be translated by the authors. Please make clear who has written the perspective and indicate when this has been translated by the authors. Patients who prefer to share an audio or video perspective should have this transcribed by the authors. For the purposes of anonymity audio and video recordings are not published
• Please check that details that reveal the identity of the patient are avoided. These include calendar dates, locations and details of other family members
• Some published articles are picked up by the wider non-medical media and patients should be made aware of this, especially, when they contribute their perspective and when they give consent for publication
• Single sentences or statements of thanks to the clinical teams will not be published
Intellectual Property Rights Assignment or Licence Statement
I, The Author has the right to grant and does grant on behalf of all authors, an exclusive licence and/or a non-exclusive licence for contributions from authors who are: i) UK Crown employees; ii) where BMJ has agreed a CC-BY licence shall apply, and/or iii) in accordance with the relevant stated licence terms for US Federal Government Employees acting in the course of the their employment, on a worldwide basis to the BMJ Publishing Group Ltd (“BMJ”) and its licensees, to permit this Work (as defined in the below licence), if accepted, to be published in BMJ Case Reports and any other BMJ products and to exploit all rights, as set out in our licence author licence.
References
- Freeman, R., Wieling, W., Axelrod, F. B., Benditt, D. G., Benarroch, E., Biaggioni, I., ... & Van Dijk, J. G. (2011). Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Autonomic Neuroscience, 161(1-2), 46-48.
- Keating, G. M. (2015). Droxidopa: a review of its use in symptomatic neurogenic orthostatic hypotension. Drugs, 75, 197-206.
- Kalra, D. K., Raina, A., & Sohal, S. (2020). Neurogenic orthostatic hypotension: state of the art and therapeutic strategies. Clinical Medicine Insights: Cardiology, 14, 1179546820953415.
- Palma, J. A., & Kaufmann, H. (2017). Epidemiology, diagnosis, and management of neurogenic orthostatic hypotension. Movement disorders clinical practice, 4(3), 298-308.
- Canosa-Hermida, E., Mondelo-García, C., Ferreiro-Velasco,M. E., Salvador-de la Barrera, S., Montoto-Marqués, A., Rodríguez-Sotillo, A., & Vizoso-Hermida, J. R. (2018). Refractory orthostatic hypotension in a patient with a spinal cord injury: Treatment with droxidopa. The Journal of Spinal Cord Medicine, 41(1), 115-118.
- Claydon, V. E., Steeves, J. D., & Krassioukov, A. (2006). Orthostatic hypotension following spinal cord injury: understanding clinical pathophysiology. Spinal cord, 44(6), 341-351.
- Mojtahedzadeh, M., Taghvaye-Masoumi, H., Najafi, A., Dianatkhah, M., Sharifnia, H., & Shahrokhi, M. (2019). Management of hypotension and bradycardia caused by spinal cord injury. The usefulness of midodrine and methylxanthines. Iranian journal of pharmaceutical research: IJPR, 18(4), 2131.
- Verberne, A. J., & OWENS, N. C. (1998). Cortical modulation of thecardiovascular system. Progress in neurobiology, 54(2), 149-168.
- Calaresu, F. R., & Yardley, C. P. (1988). Medullary basal sympathetic tone. Annual Review of Physiology, 50(1), 511-524.
- Krassioukov, A. V., & Fehlings, M. G. (1999). Effect of graded spinal cord compression on cardiovascular neurons in the rostro-ventro-lateral medulla. Neuroscience, 88(3), 959-973.
- Lebedev, V. P., Krasyukov, A. V., & Nikitin, S. A. (1986). Electrophysiological study of sympathoexcitatory structures of the bulbar ventrolateral surface as related to vasomotor regulation. Neuroscience, 17(1), 189-203.
- Reis, D. J., Morrison, S., & Ruggiero, D. A. (1988). The C1 area of the brainstem in tonic and reflex control of blood pressure. State of the art lecture. Hypertension, 11(2_pt_2), I8.
- Furlan, J. C., Fehlings, M. G., Shannon, P., Norenberg, M.D., & Krassioukov, A. V. (2003). Descending vasomotor pathways in humans: correlation between axonal preservation and cardiovascular dysfunction after spinal cord injury. Journal of neurotrauma, 20(12), 1351-1363.
- Mathias, C. J., & Bannister, R. (Eds.). (2013). Autonomic failure: a textbook of clinical disorders of the autonomic nervous system. OUP Oxford.