
Journal of ENT Surgery Research(JESR)

Case Report - (2025) Volume 3, Issue 1
Post-Traumatic Facial Palsy: Report of Two Clinical Cases and Review of the Literature
2Resident in Otorhinolaryngology–Head and Neck Surgery, Specialties Hospital, University Hospital Center of Rabat, Morocco
3Assistant Professor, Department of ENT and Head & Neck Surgery, Specialties Hospital, University Hospital Center of Rabat, Morocco
4Professor of Higher Education, Department of ENT and Head & Neck Surgery, Specialties Hospital, University Hospital Center of Rabat, Morocco
5Head of the ENT and Head & Neck Surgery Department, Professor of Higher, Specialties Hospital, University Hospital Center of Rabat, Morocco
Received Date: Nov 01, 2025 / Accepted Date: Nov 28, 2025 / Published Date: Dec 05, 2025
Copyright: ©©2025 Dr. Khalil Hjaouj, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Hjaouj, K., Ennouali, A., Mekkaoui, M., Elhafi, Z., Arkoubi, Z., et al. (2025). Post-Traumatic Facial Palsy: Report of Two Clinical Cases and Review of the Literature. J of ENT Surgery Research, 3(1), 01-08.
Abstract
Background: Post-traumatic facial paralysis is a rare but functionally and psychologically devastating complication of temporal bone fractures, occurring in approximately 6–10% of cases. Early recognition and appropriate management are crucial for optimizing outcomes.
Objective: To describe two cases of post-traumatic facial paralysis in paediatric patients and to discuss the diagnostic and therapeutic challenges associated with this condition.
Methods: Two children presenting with facial paralysis following temporal bone trauma were evaluated clinically, radiologically, and electrophysiologically. Their management strategies and outcomes were compared.
Results: The first patient presented with immediate and complete facial paralysis following a high-impact head injury and underwent surgical exploration with nerve repair. The second developed delayed and incomplete paralysis managed conservatively with corticosteroids, achieving full recovery. Both cases highlight the role of imaging and electrodiagnostic studies in guiding treatment decisions.
Conclusion: Management of post-traumatic facial paralysis requires an individualised approach guided by the severity and timing of onset. Early diagnosis, accurate topographical evaluation, and a multidisciplinary strategy remain essential for optimal functional recovery.
Keywords
Facial nerve, Temporal bone fracture, Paediatric trauma, Post-traumatic facial paralysis, Surgical decompression
Introduction
Post-traumatic facial paralysis represents a rare but serious consequence of craniofacial trauma with an estimated incidence of 1.5% among head injuries and 6–10% among temporal bone fractures [1,2]. Although road safety improvements have reduced its frequency, such cases remain regularly encountered in tertiary referral centers [3]. The management of this condition depends on the completeness and timing of onset of facial dysfunction. Immediate and complete paralysis often indicates a direct mechanical disruption of the facial nerve, warranting surgical exploration, whereas delayed or incomplete forms usually result from oedema, compression, or ischaemia and may respond to corticosteroid therapy [4,5]. However, the optimal timing for surgery and the prognostic significance of electrodiagnostic findings remain matters of debate [6].
This issue is even more complex in children. In paediatric patients, facial nerve palsy poses unique challenges due to diagnostic delay, greater bone elasticity, and potential long-term psychosocial consequences. Children often have incomplete or non-displaced fractures owing to the increased compliance of the temporal bone, which may mask the underlying nerve injury. Moreover, the assessment of facial function and compliance with electrophysiological testing can be difficult at this age.
Early identification and appropriate management are therefore crucial to ensure optimal neural recovery and to prevent permanent facial dysfunction. This paper reports two paediatric cases of post- traumatic facial paralysis with distinct clinical presentations and discusses their management in light of current literature.
Case Report
Case 1
A five-year-old boy presented to the emergency department following a motorcycle fall with a left temporo-parietal impact. Initial examination revealed left otorrhagia and a peripheral facial paralysis graded III on the House–Brackmann (HB) scale.

Figure 1: picture showing a post-traumatic left peripheral facial palsy
Impedance audiometry demonstrated an absent stapedial reflex on the affected side, suggesting a proximal lesion. High-resolution computed tomography (CT) of the temporal bone revealed a longitudinal fracture of the left petrous portion with an associated ipsilateral subdural haematoma and pneumocephalus deemed non- surgical.
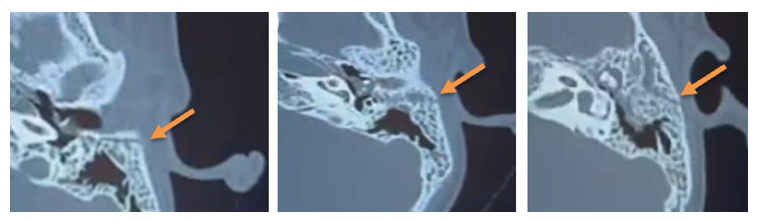
Figure 2: Axial CT scan of the temporal bone showing a simple transverse fracture line of the petrous portion of the temporal bone, sparing the otic capsule, with haemorrhagic opacification of the tympanic cavity and mastoid air cells
Electro-neuromyography (ENMG) performed ten days post- trauma showed severe axonotmesis with more than 70% axonal loss.
Based on the imaging findings and the severity of the electrophysiological lesion, surgical exploration was performed through a transmastoid approach one month after the trauma. A cortical mastoidectomy was first performed, followed by an antro-atticotomy to expose the short process of the incus, a key landmark for identifying the facial nerve. A wide posterior tympanotomy was then carried out, allowing decompression of the facial nerve at the level of its genu and mastoid segment. Intraoperative findings revealed a severely contused facial nerve at the second genu, consistent with axonotmesis, while neural continuity was preserved. Decompression of the tympanic and mastoid segments was achieved, and a temporalis fascia graft was interposed to protect and support the injured segment.

Figure 3: Per-operative image showing decompression of the facial canal at its second genu using a diamond burr
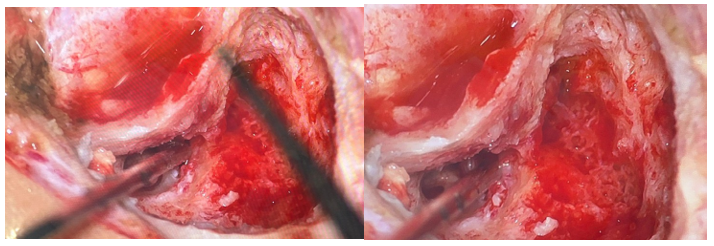
Figure 4: Per-operative image showing the appearance of the facial nerve after decompression
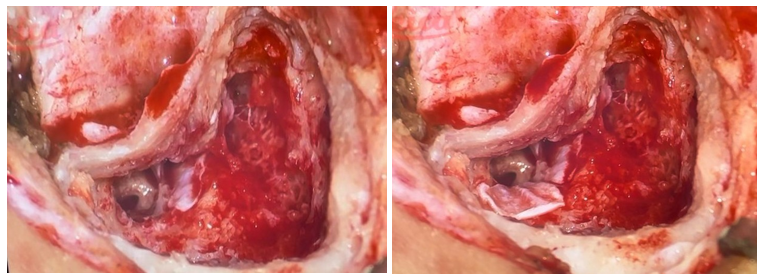
Figure 5: Per-operative image showing two aponeurotic grafts at the genu and the mastoid (third) segment of the facial nerve, through the posterior tympanotomy, the round window niche, the pyramidal eminence, and the stapes tendon were clearly visualized
Post-operative management consisted of ocular protection, a one- month course of corticosteroids with progressive tapering, vitamin therapy, and facial physiotherapy.


Figure 6: Same patient after facial nerve decompression and repair showing improved eye closure and smile symmetry
The patient is currently under follow-up with near complete recovery.

Figure 7: Three-month follow-up revealing near-complete recovery of facial symmetry and voluntary movements
Case 2
A fourteen-year-old girl was referred to our department from the emergency service, where she had been admitted following a road traffic accident with a left temporo-facial impact. On the day of the accident, a brain CT scan was performed and appeared normal. Her physical and neurological examinations revealed no abnormalities, and she was discharged.
Five days after the trauma, her family noticed immobility of the left corner of the mouth and an inability to close the left eye, prompting a second visit to the emergency department.
Clinical examination showed a left peripheral facial nerve palsy graded IV on the House–Brackmann (HB) scale, associated with otorrhagia and conductive hearing loss. Temporal bone CT demonstrated a horizontal fracture line passing through the anterior wall of the tympanic bone, sparing the carotid canal, and associated with partial hemotympanum and mastoid opacification. Pure-tone audiometry confirmed a moderate conductive hearing loss on the left side. Electroneuromyography revealed severe axonal injury without evidence of neurotmesis.
A course of oral corticosteroids (prednisone 1 mg/kg/day for one month, with gradual tapering) was initiated. Clinical improvement was noted within one week, with complete resolution of both facial dysfunction and hearing deficit after one month of follow-up.

Figure 8: Audiometric assessment showing a conductive hearing loss predominantly on the left side (“40dB” at 1kHz)
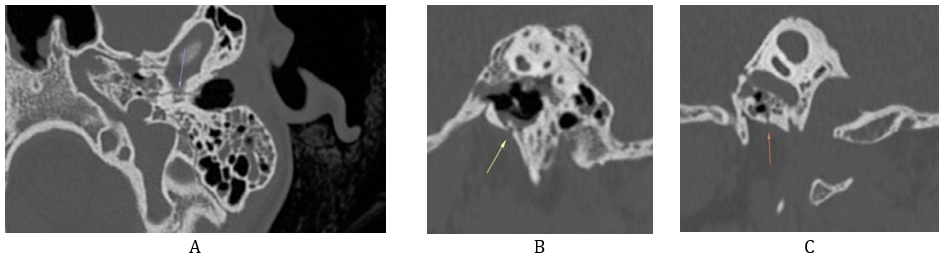
Figure 9: Axial (A) and sagittal (B, C) CT images of the temporal bone showing a transverse fracture of the petrous portion sparing the otic capsule
Discussion
Facial paralysis following temporal bone trauma is an uncommon but significant complication, particularly in children, due to its aesthetic, functional, and psychosocial consequences [7]. The incidence of petrous fractures in paediatric head trauma ranges from 30–75%, with facial nerve palsy occurring in 3–9% of cases [8]. High-velocity lateral impacts transmit shock waves through the temporal bone, exposing the intrapetrous facial nerve to various injury mechanisms. The segments most commonly involved, in decreasing order of frequency, are the geniculate ganglion (66-80%), the first genu (20%), the tympanic segment (4- 8%), and the mastoid segment (6-16%). Concomitant involvement of the geniculate ganglion and the mastoid segment is frequently observed [9-11].
The newer classification, which correlates more closely with functional prognosis, distinguishes fractures involving the otic capsule (translabyrinthine) from those sparing it (extralabyrinthine) [11]. According to this classification, 85–96% of temporal bone fractures are classified as otic capsule–sparing. [12,13]
Facial nerve paralysis occurs more frequently in fractures involving the otic capsule (39-50%) compared with capsule-sparing fractures (2-21%) [11].
Immediate-onset paralysis generally reflects direct mechanical injury to the nerve—by transection, contusion, or traction- whereas delayed forms result from secondary phenomena such as compression from oedema or haematoma, or microvascular ischaemia similar to Bell’s palsy [9,14].
In children, incomplete ossification of the skull increases cranial compliance, reducing the likelihood of overt fractures but not excluding significant nerve injury. Fracture lines often propagate indirectly from distant impact points, involving weaker bony regions such as the squamous and tympanic parts, while sparing the dense labyrinthine bone. This may explain the occasional mismatch between mild imaging findings and substantial neurological deficits.
Clinical evaluation remains paramount in assessing post-traumatic facial dysfunction. It begins with a detailed analysis of facial symmetry at rest and during voluntary movement, evaluating forehead wrinkling, eye closure, nasolabial fold depth, and oral commissure excursion. In comatose patients, the Pierre-Marie and Foix maneuver which consists of applying a painful stimulus and observing the grimace response, where asymmetry indicates facial paralysis on the affected side. Associated signs such as otorrhagia, hypoacusis, otoliquorrhoea, or vestibular symptoms should be systematically sought, as they may indicate concomitant temporal bone fracture or ossicular chain disruption. [15]
The House–Brackmann (HB) grading system, introduced in 1985, provides a standardized and universally adopted scale for grading facial motor dysfunction. It ranges from Grade I (normal function) to Grade VI (complete paralysis):
|
Grade I: Normal facial symmetry and movement. |
Normal facial symmetry and movement. |
|
Grade II: Mild dysfunction |
Rest: normal symmetry and tone. Forehead: slight to normal movements. Eye: complete closure with minimal or maximal effort. Secondary abnormalities: very mild and inconsistent synkinesis, no contracture. |
|
Grade III: Moderate dysfunction |
Rest: normal symmetry and tone. Forehead: slight or absent movements. Eye: complete closure with maximal effort, though with evident asymmetry. Secondary abnormalities: noticeable but non-severe synkinesis and/or contracture. |
|
Grade IV: Moderately severe dysfunction |
Rest: normal symmetry and tone. Forehead: no movement. Eye: incomplete closure with maximal effort. Secondary abnormalities: severe synkinesis and/or contracture |
|
Grade V: Severe dysfunction |
Rest: asymmetry present. Forehead: no movement. Eye: slight movement with maximal effort. Secondary abnormalities: synkinesis and contracture usually absent. |
|
Grade VI: Total paralysis |
Rest: complete loss of tone. Forehead: no movement. Eye: no movement. Secondary abnormalities: absent. |
This system remains the reference for initial assessment and follow-up. An HB grade ≥ IV typically suggests significant axonal injury and a less favorable prognosis, especially in the context of immediate paralysis. [6,16].
In addition, the absence of the stapedial reflex on impedance audiometry supports a proximal lesion, located above the branch to the stapedius muscle (usually in the labyrinthine or geniculate segment). This finding, combined with electrophysiological testing, helps refine the topographical diagnosis and predict the likelihood of spontaneous recovery.
High-resolution computed tomography (CT) of the temporal bone is the reference imaging tool for assessing post-traumatic facial dysfunction. It precisely identifies the type and orientation of the fracture and its relationship with the facial canal, helping to locate possible sites of nerve injury. CT also reveals associated lesions such as ossicular disruption, hemotympanum, or pneumolabyrinth. [17-19].
An arterial and/or venous CT angiography is indicated for any fracture involving the carotid canal, jugular foramen, or venous sinuses, or in the presence of clinical signs suggestive of vascular injury. Magnetic resonance imaging (MRI) has no role in the emergency assessment of temporal bone fractures and should be performed secondarily to evaluate their complications [20].
Electroneurography (ENoG) and electromyography (EMG) provide valuable prognostic information and help guide management decisions [21].
Electroneurography (ENoG): ENoG assesses the percentage of inactive fibres and quantifies the degree of denervation. It is performed and repeated between day 3 and day 21 after the onset of facial paralysis. A degeneration exceeding 90–95% of fibres is considered a poor prognostic indicator.
Electromyography (EMG): EMG evaluates the proportion of active fibres and monitors neural recovery. It is typically performed between two weeks and three months after the onset of paralysis. The appearance of polyphasic reinnervation potentials suggests incomplete nerve transection.
Additional topographic assessments—such as the Schirmer test, gustometry, and evaluation of the stapedial reflex—have also been proposed by several authors to help localise the site of traumatic injury [9].
Medical treatment is systematically indicated in all cases of traumatic facial dysfunction. It combines systemic corticosteroid therapy, administered at a dose of at least 1 mg/kg per day [15]. A retrospective study reported a higher rate of facial function recovery in patients who initiated corticosteroid therapy within the first 24 hours and continued it for more than two weeks [22]. However, the use of high-dose corticosteroids in patients with concomitant intracranial injuries has been associated with increased mortality, supported by a high level of evidence therefore, the risk–benefit balance of corticosteroid therapy in such settings must be carefully evaluated [23]. Antiviral therapy (e.g., aciclovir) has been suggested in select cases where viral reactivation is suspected, although its efficacy remains unproven [24,25]. Supportive management includes ocular protection with lubricants and eye closure techniques to prevent keratitis, and facial physiotherapy to preserve muscle tone and reduce synkinesis. The recovery period under medical treatment varies from one day to one year: 59 % of patients recover within the first month, and 88 % within three months [1].
The optimal timing of surgical intervention remains debated. Most authors advocate early exploration, ideally within the first 14 days in cases of complete and immediate paralysis with poor electrophysiological prognosis [26]. Early decompression limits the risk of irreversible Wallerian degeneration and promotes more complete reinnervation. Beyond three weeks, fibrotic changes and canal ossification may reduce the likelihood of functional recovery. Several surgical approaches can be adopted depending on hearing status and lesion topography. When hearing is preserved, a combined transmastoid and middle cranial fossa approach allows access to the labyrinthine and geniculate segments without compromising cochlear function. In contrast, a translabyrinthine approach is reserved for patients with non- serviceable hearing, offering wider exposure at the cost of cochlear sacrifice. Decompression should extend at least two contiguous segments of the facial canal, and in cases of nerve discontinuity, direct anastomosis or autologous grafting (commonly with sural or great auricular nerve) is recommended [27,28].
Recovery after traumatic facial paralysis depends on the initial severity of injury, timing of intervention, and adequacy of decompression. Reported rates of satisfactory recovery (House– Brackmann grades I–II) range from 60 to 90% in incomplete or delayed forms managed medically, and 50 to 70% in surgically treated complete cases [29]. Improvement may continue for up to one year due to gradual axonal regeneration at approximately1 mm per day. Long-term follow-up with serial clinical and electrophysiological assessments is essential to document reinnervation, guide rehabilitation, and detect complications such as synkinesis or gustolacrimal reflex (“crocodile tears”) [30].
Conclusion
Post-traumatic facial paralysis remains a rare but challenging complication of temporal bone fractures. Its management should be guided by the mechanism of injury, the timing and severity of paralysis, and electrodiagnostic and imaging findings. Early recognition, multidisciplinary evaluation, and appropriate therapeutic stratification-medical or surgical—are key to optimizing functional recovery and minimizing long-term sequelae.
Conflict of Interest
The authors declare no conflicts of interest.
Ethical Approval and Consent
Written informed consent for publication of this case report and accompanying images was obtained from the patient’s parents.
References
- Brodie, H. A., & Thompson, T. C. (1997). Management of complications from 820 temporal bone fractures. Otology & Neurotology, 18(2), 188-197.
- Dahiya, R., Keller, J. D., Litofsky, N. S., Bankey, P. E., Bonassar, L. J., & Megerian, C. A. (1999). Temporal bone fractures: otic capsule sparing versus otic capsule violating clinical and radiographic considerations. Journal of Trauma and Acute Care Surgery, 47(6), 1079.
- Asha’ari, Z. A., Ahmad, R., Rahman, J., Yusof, R. A., & Kamarudin, N. (2012). Patterns of intracranial hemorrhage in petrous temporal bone fracture. Auris Nasus Larynx, 39(2), 151-155.
- Kansu, L. (2018). Post-traumatic delayed peripheral facial palsy. The Journal of Pediatric Research.
- Gantz, B. J., Rubinstein, J. T., Gidley, P., & Woodworth,G. G. (1999). Surgical management of Bell's palsy. The Laryngoscope, 109(8), 1177-1188.
- Khangwal, M., Solanki, R., Bali, A., Khanna, Y., Kumar, D., & Tanwar, R. DELAYED POST TRAUMATIC FACIAL NERVE PALSY ON CONTRA LATERAL SIDE OF ISOLATED MANDIBULAR FRACTURE: A RARE.
- Brown J, Hohman MH, Noreikaite G, et al. (2025). Facial Nerve Intratemporal Trauma. In: StatPearls. Treasure Island (FL): StatPearls Publishing.
- Yadav, S., Panda, N. K., Verma, R., Bakshi, J., & Modi, M. (2018). Surgery for post-traumatic facial paralysis: are we overdoing it?. European Archives of Oto-Rhino- Laryngology, 275(11), 2695-2703.
- Darrouzet, V., Duclos, J. Y., Liguoro, D., Truilhe, Y., De Bonfils, C., & Bebear, J. P. (2001). Management of facial paralysis resulting from temporal bone fractures: our experience in 115 cases. Otolaryngology—Head and Neck Surgery, 125(1), 77-84.
- Lambert, P. R., & Brackmann, D. E. (1984). Facial paralysis in longitudinal temporal bone fractures: a review of 26 cases. The Laryngoscope, 94(8), 1022-1026.
- Ishman, S. L., & Friedland, D. R. (2004). Temporal bone fractures: traditional classification and clinical relevance. The Laryngoscope, 114(10), 1734-1741.
- Montava, M., Masson, C., Lavieille, J. P., Mancini, J., Soussan, J., Chaumoitre, K., & Arnoux, P. J. (2016). Temporal bone fracture under lateral impact: biomechanical and macroscopic evaluation. Medical & biological engineering & computing, 54(2), 351-360.
- Schubl, S. D., Klein, T. R., Robitsek, R. J., Trepeta, S., Fretwell, K., Seidman, D., & Gottlieb, M. (2016). Temporal bone fracture: Evaluation in the era of modern computed tomography. Injury, 47(9), 1893-1897.
- SanuÅ?, G. Z., Tanriöver, N., Tanriverdi, T., Uzan, M., & Akar, Z. (2007). Late decompression in patients with acute facial nerve paralysis after temporal bone fracture. Turkish neurosurgery, 17(1), 7-12.
- Tankéré. Paralysie faciale périphérique. CrossRef Listing Deleted DOIs. Epub ahead of print 2000. DOI: 10.1016/ s0246-0351(22)87762-x.
- Gladwell, M., & Viozzi, C. (2008). Temporal bone fractures: a review for the oral and maxillofacial surgeon. Journal of oral and maxillofacial surgery, 66(3), 513-522.
- Saraiya, P. V., & Aygun, N. (2009). Temporal bone fractures. Emergency radiology, 16(4), 255-265.
- Coker, N. J., Kendall, K. A., Jenkins, H. A., & Alford,B. R. (1987). Traumatic infratemporal facial nerve injury: management rationale for preservation of function. Otolaryngology–Head and Neck Surgery, 97(3), 262-269.
- https://matilda.science/work/76765c83-f87f-4a54-a1f2- e6cc1c942b14?l=fr
- Bentan, M. A., Thacker, L., & Coelho, D. H. (2023). Vascular injury arising from lateral skull base fractures. American Journal of Otolaryngology, 44(2), 103729.
- DOI: 10.1016/s0246-0351(24)46946-8.
- Shankar, A., George, S., & Somaraj, S. (2022). Evaluation of clinical outcome in traumatic facial nerve paralysis. International Archives of Otorhinolaryngology, 26(01), e010-e019.
- CRASH Trial Collaborators. (2005). Final results of MRC CRASH, a randomised placebo-controlled trial of intravenous corticosteroid in adults with head injury—outcomes at 6 months. The Lancet, 365(9475), 1957-1959.
- Gordin, E., Lee, T. S., Ducic, Y., & Arnaoutakis, D. (2015). Facial nerve trauma: evaluation and considerations in management. Craniomaxillofacial trauma & reconstruction, 8(1), 1-13.
- Goudakos, J. K., & Markou, K. D. (2009). Corticosteroids vs corticosteroids plus antiviral agents in the treatment of Bell palsy: a systematic review and meta-analysis. Archives of Otolaryngology–Head & Neck Surgery, 135(6), 558-564.
- Gilden, D. H. (2004). Bell's palsy. New England Journal of Medicine, 351(13), 1323-1331.
- Sullivan, F. M., Swan, I. R., Donnan, P. T., Morrison, J. M.,Smith, B. H., McKinstry, B., ... & Daly, F. (2007). Early treatment with prednisolone or acyclovir in Bell's palsy. New England Journal of Medicine, 357(16), 1598-1607.
- Honnurappa, V., Vijayendra, V. K., Mahajan, N., & Redleaf,M. (2019). Facial nerve decompression after temporal bone fracture—the bangalore protocol. Frontiers in Neurology, 10, 1067.
- Birgfeld, C., & Neligan, P. (2011). Surgical approaches to facial nerve deficits. Skull Base, 21(03), 177-184.Quaranta, Giuseppe Campobasso, Fabio Piazza, Nicola
- Quaranta, Ignazio Salonna, A. (2001). Facial nerve paralysis in temporal bone fractures: outcomes after late decompression surgery. Acta oto-laryngologica, 121(5), 652-655.