



Research Article - (2021) Volume 6, Issue 3
Poor Trends in Glycemic, Weight and Blood Pressure Control during Screening in Population among Small town of Karachi
2FCPS, Medicine, Cardiology, Hamdard Medical University, Karachi, Pakistan
3MBBS, M.Phil., Bilawal Medical College, Jamshoro, Pakistan
Received Date: Jan 08, 2021 / Accepted Date: Oct 28, 2021 / Published Date: Nov 05, 2021
Copyright: ©Khalida Soomro, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Khalida Soomro, Sumera Nasim, Muhammad Ali Soomro (2021) Poor Trends in Glycemic, Weight and Blood Pressure Control during Screening in Population among Small town of Karachi. Cardio Open, 6(3): 155-160.
Abstract
Introduction: Diabetes is common cause of mortality in adults globally due to the increase in the risk of vascular complications. Pakistanis are an ethics group having an inherent predilection to develop diabetes. But this rise in incidence and prevalence is associated with demographics a social pattern, life style, unawareness due to low-literacy rate thus leading to obesity in the country. The high number of people in the pre-diabetic state or with undiagnosed diabetes represents large pool of individuals in rural areas than urban areas.
Aims and Objective: Knowing the prevalence of these comorbidities like Diabetes, obesity and Hypertension contributing with each other is important for determining the size of the population that may benefit from strategies that reduce blood pressure and weight while controlling blood glucose. Prevention and control need to be structured at all levels of prevention and through the Promotion of early detection of diabetes through screening and diabetes education.
Material and Methods: All persons aged 20-70 years attending the medical camps organized in small towns near to Karachi during (2017 June-2021 June) were tested for diabetes for free with help of Sindh Graduate Association and Go Red for Women Program Pakistan Cardiac Society. Data on their age, gender, height, weight, diabetes status and blood pressure were also taken. Basal mass Index was calculated and stratified as per WHO classifications. 2120 persons were screened but complete data for 1289 persons was available for analysis.
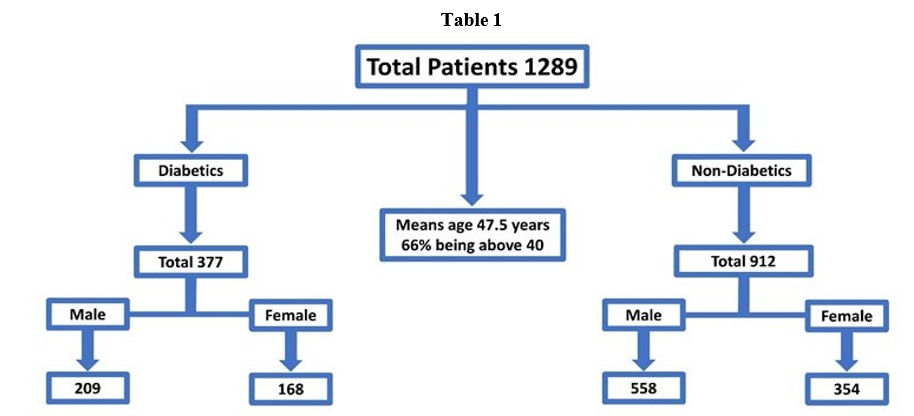
Result: Out of 1289 screened people who attended the medical camps, 377 were known diabetics with mean age was 47.5 years with 66% being above 40. 60.2% had poor glycemic control using an optimum of <7.8 mmol/L, 54.59% had poor glycemic control with blood sugars exceeding 10 mmol/L. patients with HBA1c<7%, 50% being hypertensive in spite of the treatment. 62% of women were either overweight or obese then 33.3% in men. BMI above 30 kg/m2 as measure of obesity was found in 32%. in all those who were known diabetics. 12% (92) of those not known to have diabetes had either impaired glucose tolerance or were newly diagnosed diabetics.
Conclusion: In our Study the Large proportion of diabetics were found with poor glycemic control. The majority of known diabetes patients were also at risk due to owning overweight, obesity and poorly controlled blood pressure, Emphasis should be on the promotion of early detection of diabetes through screening and diabetes education in under develop areas of Pakistan.
Keywords
Hypertension (HTN), Diabetes (DM), Weight Control (WC), Improperly High Plasma Glucose (IHPG), Body Mass Index (BMI), Random Plasma Glucose (RPG), Fasting Plasma Glucose (FPG); Oral Glucose Tolerance Test (OGTT), Systolic Blood Pressure (SBP).
Introduction
Diabetes is one of the five leading causes of death worldwide and remains to be an expanding global health crisis the world preva- lence of diabetes according to the International Diabetes Federa- tion (IDF). In age 20-79, was 6.4%, affecting 285 million in 2010, and expectedly increasing to 7.7% (439 million) by 2030. Between 2010 and 2030, there will be a 69% increase in numbers of adults with diabetes in developing countries and a 20% increase in de- veloped countries [1-3]. Pakistanis have rising diabetes incidence and prevalence which is associated with increase in life, demo- graphics and social conditions, consumption of unhealthy diets and physical inactivity leading to obesity and hypertension, due to the increasing urbanization and social development more than 46% of diabetes patients specially women s are unaware of their condition and a large pool of individuals are in the pre-diabetic state or with undiagnosed diabetes in small towns [4-8]. Chronic obesity leads to increased insulin resistance that can develop into type 2 diabetes, most likely because adipose tissue, (especially the intra-abdominal) is a source of hormones and cytokines. On the other hand, type 2 diabetes may cause obesity as an effect of the changes in metabolism and other deranged cell behavior atten- dant on insulin resistance. The combined environmental-genetic influence on developing DM can be evidenced. Knowledge and awareness about diabetes, its risk factors, complications and man- agement are important aspects for better control and better quality of life (QOL) in patients, especially in developing countries like Pakistan where diabetes its related hypertension and obesity are in escalation but still important differences in these risk factors have not been fully explored [9].
Aims and Objectives
Diabetes and its related risks are globally elevated in South Asians. Prevention and control of diabetes-related Hypertension and Obe- sity need to be structured. There is clear potential in reducing di- abetes Hypertension Obesity and their related mortality and mor- bidity by addressing risk which has not been fully evidenced yet at both primary and secondary prevention levels [9]. We conducted this study to explore the variations in the impact of risk factors, analyze the prevalence of prediabetes and diabetes and to evalu- ate the influence of some demographic criteria, weight, and blood pressure upon blood glucose among the Pakistani population of small towns.
Material and methods
Population based Cross-sectional survey (2017 June-2021 June). Participants visiting for the screening in medical camps from the nearby small towns of Karachi City with help of Sindh Gradu- ate Association and Go Red for Women Program Pakistan Cardi- ac Society. A total of 377 were screened out of 1289 individuals aged 15-70years but complete data for all persons was available for analysis Table 1.
Screening and risk assessment were performed with question- naires. which consists demographic criteria, e.g., age, marital status etc., life style, Chronic Diseases (perceived Health Status) risk factors, e.g., tobacco use, HTN, DM, BMI. The questionnaire takes 20 minutes to complete a signed consent to take part in the screening plan was obtained from participants [9,10]. An analysis based on the performed free measurement of blood glucose con- centration with enzymatic assay techniques, prediabetes screening analyses with fasting plasma glucose (FPG); the 75-g oral glucose tolerance test (OGTT), and casual (random) plasma glucose (RPG) level. The basal mass index was calculated and stratified as per WHO classification was defined in (kg/m²) l as underweight <20, normal weight 20-24.9, overweight 25-29.9, and obesity stag- es stage-1 (30 - 34.9), stage-2 (35 - 39.9), morbid obesity ≥40). Higher threshold cut off of BP for diabetic patients was kept at 130/80mmhg [11].
In the second phase of analysis, we examined the effect of the risk factors on RPG (measured) as a frank diabetes/prediabetes disease state, BP measurement and checked the BMI or any complication occurred during the period and Patients were reviewed for treat- ment and prevention achieved benefit of diabetic patients with re- lated risks. Analysis was performed with cross-tabulation, as in chi-square test. The SPSS software for Microsoft-version-20 was used for statistical analyses. The statistical analysis approach prin- cipally encompassed descriptive statistics.
Results
A total of 377 out of 1289 people who attended the screening camps were known diabetics with median age was 46.7 (QR 11.9) years with 66% being above 40 years. 60.2% people had poor gly- cemic control using an optimum of <7.8 mmol/L. (>140mg/dl) and 54.59% with blood sugars exceeding 10 mmol/L (>180mg/ dl). Newly diagnosed Diabetics with Impaired glucose tolerance were 90 (12%) on sugar above (>140mg/dl) vs 20 (03%) sugar (>180mg/dl) Table 2.
Table 2
|
Diabetes Prevalence |
|
|
Known Diabetics |
Not Known Diabetics |
|
Poor Glycemic Control |
Newly diagnosed Diabetics with Impaired glucose tolerance |
|
62.2% <7.8 mmol/L (>140mg/dl) |
90 (12%) |
|
54.59% 10 mmol/L (>180mg/dl) |
20 (03%) |
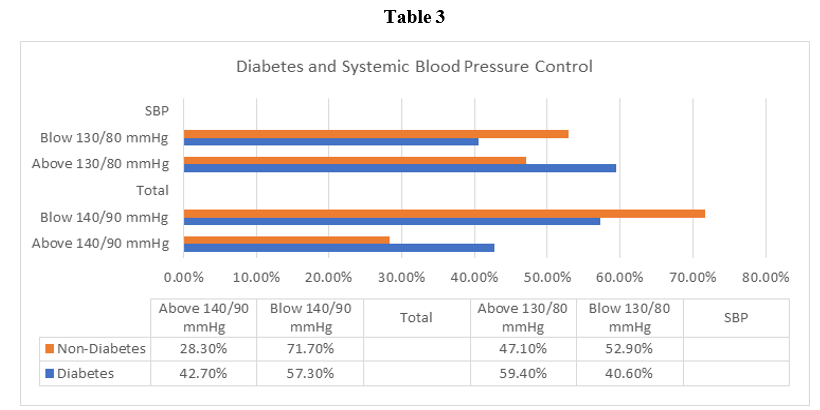
Among screened persons 32% (419) were hypertensive, 42% (161) were diabetics and 28.3% were non-diabetics. HBA1c < 7% was about 50% in persons being hypertensive in spite of the treatment when a higher threshold of 130/80 mmHg as recommended in care diabetics was used. When a BP cut off of 140/90 mmHg was used,59.4% of diabetics were found to have coexisting hypertension that was poorly controlled Table 3.
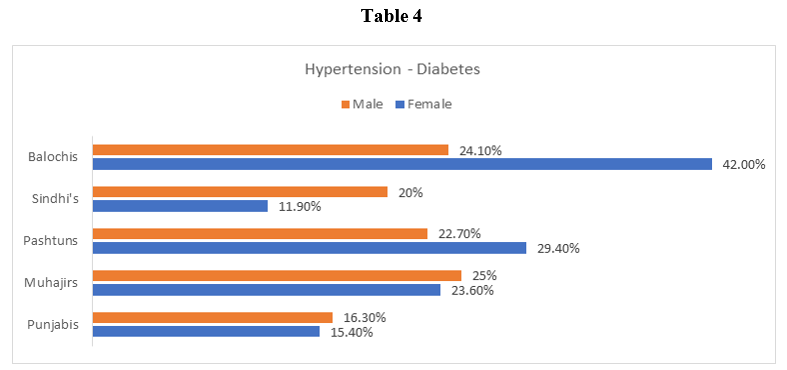
Prevalence of the Hypertension varied in the different ethnic groups and areas. The age-standardized prevalence of hypertension was highest among Balochis (25.3% in men and 41.4% in women), then Pashtuns (23.7% in men and 28.4% in women), Muhajirs (24.1% in men and 24.6% in women), and lowest among Punjabis (17.3% in men and 16.4% in women) and Sandhi’s (19.0% in men and 9.9% in women) (P = 0.001) Table 4.
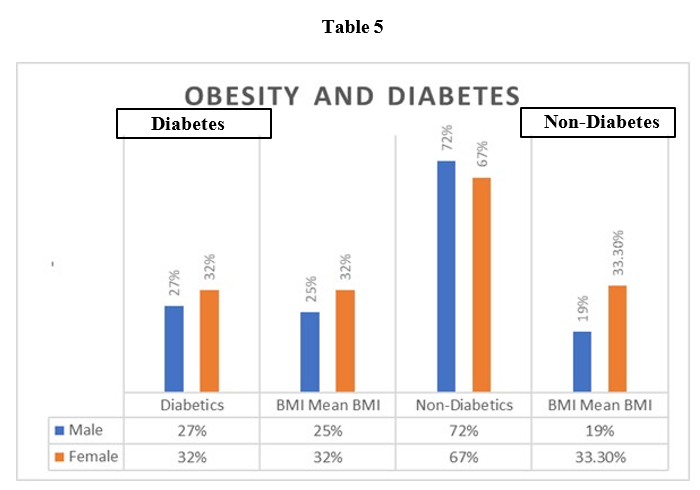
Almost two-thirds of screened patients for the Diabetes were either overweight (34.7%) or obese (29.9%). The mean BMI is among the non-diabetics was 26.75kg/m2. 58% of diabetics had a BMI of above 25 with a mean BMI of 27.13 kg/m2and in 32% diabetics BMI was above 30 kg/m2 as a measure of obesity was found in 62% of women and 52%men were either overweight or obese with 33.3% of the women. 92 (12%) were those not known to have diabetes or with impaired glucose tolerance newly diagnosed diabetics women had BMI of above 30 as compared to 19% in men. The mean waist circumference (WC) was 94.7 ± 13.3 cm; and 27.9% had central obesity (WC ≥102 cm) in screened group Table 5.
The BMI increased with age and 65% of these >41 years were either overweight or obese.
In the second phase of analysis, the prevalence of the ultimate re- search outcome, which is prediabetes/diabetes, among the study population was examined. Age, and SBP were significantly related to the development of prediabetes/diabetes; BMI was not. The ten- dency for recording high BMI levels (>25 and ≥40 kg/m2 among those with reported history of DM was higher than with recording normal.
Discussion
HTN, DM, Obesity is an exacerbating public health problem in developing countries like Pakistan, is most likely result of an im- balanced diet, lack of physical activity, and various other social and demographic factors like age, and family history etc. Mur- ray & Lopez, et al (1997), Jafar, et al (2003), Jafar, et al (2005), Rahman, et al (2006), Abbas, et al (2009). [12-17], in the present study of 377 out of 1289 adults with diabetes with poor glycemic control, hypertension and BMI acted as a random audit record of screening at medical camps of clinical services. As the effective- ness of screening depends on the setting in which it is performed and should the positively screened fail to obtain appropriate fol- low-up care. so, these patients of our study were screened during the medical camps criteria for the screening met 1-4 of the follow- ing conditions in asymptomatic populations [18,19].
• The disease represents an important health problem that im- poses a significant burden on the population,
• The natural history of the disease is understood
• There is a recognizable preclinical stage during which the dis- ease can be diagnosed
• Reliable tests are available that can detect such preclinical stage
• Treatment after early detection yields benefits superior to those obtained when treatment is delayed,
• The costs of treatment are reasonable and are balanced in rela- tion to health expenditures, and resources are available to treat newly diagnosed cases,
• Screening will be a systematic ongoing process and not mere- ly an isolated one-time effort. The data revealed that majority of known diabetes patients are at a risk of long-term complications owing to Overweight and obesi- ty (58%), Poor controlled blood pressure (59.4%), Poor glycemic control (60.2%). The high number of people in the pre-diabetic’s state or with undiagnosed diabetes represented a large pool of in- dividuals who were supposed to be at risk of presenting with long- term complications of Diabetes. Importantly, age was strongly correlated with all the risks, including WC, BMI, and SBP. Asso- ciation of glycemic control on the basis of fasting plasma glucose was also assessed and hypertension was significantly found to be associated with poor glycemic control. Two third of our subjects with type 2 diabetes were obese with a BMI>25 Kg/m; according to the recommendations of the WHO Asia-Pacific Regional Office. with females more obese as compared to males’ similar pattern in other Asian Countries. and a strong correlation between BMI and WC was observed in study.
In practice, WC has been widely used to endorse the presence of “central obesity”, which is a pivotal factor contributing to insu-lin resistance. Different cut-off points for obesity, ranging from 78 cm, as in assessing some male Asian populations with one or more cardiovascular risk factors and for identifying those with a BMI above normal to 102 cm, which is the generally international cutoff for male obesity (and 88 cm for obesity in females), have been in use, based on ethnicity, risk profile, anthropometric and demographic traits, as well as the prevailing dietary behavior [20].
In Osaimi and collaborates (2007) worked to determine the prev- alence and CVD risks in a suburban community in eastern Ri- yadh district, KSA, 71/451 (15.8%) of those surveyed had type 2 diabetes [21]. The findings of study suggest that complications are more in subjects with Diabetes and Hypertension and obesity. Obese subjects had a positive association with systolic and diastol- ic blood pressure suggesting that losing weight could also have a beneficial effect on blood pressure in diabetic subjects. This was evident by association of hypertension with FPG and of diastolic hypertension with hyperglycemia. Systolic blood pressure had an association with those subjects who had any microvascular com- plications. Diastolic blood pressure was only associated with those having nephropathy. So, tight control of Blood pressure is manda- tory [20, 22,23].
Explanations for the discrepancy between adequacy of DM man- agement. Improperly high plasma glucose (IHPG) in diabetics of- ten accompanies comorbid conditions, such as infection, stress or other health challenges. Which need to keep our diabetic group under close surveillance and guidance by an efficient health edu- cation plan in order to reduce fluctuation of plasma glucose level [24,25]. So, that complication can be postpone Adopting an inte- grated diabetes management strategy which appreciates the role of continuous patient and family education and close follow up bridges the gap between policy and the health outcomes, e.g., in terms of better control of diabetes Hypertension, body mass and abdominal size, and glucose level monitoring at different age phases of our community [26].
Conclusion
In conclusion this study shows the mostly diabetics were having poor glycemic, Hypertension and Weight control. As the majority of known diabetes patients are at risk of long-term complications owning to overweight and obesity (58%), Poorly controlled blood pressure (59.4%), Poor glycemic control (60.2%). Prediabetes and uncontrolled diabetes are relatively prevalent among the study group. This information could be very helpful in planning health- care strategies. A preventive approach to revert the predisposition of prediabetes in WD recruit’s population is quite promising. Em- phasis should be on the promotion of early detection of diabetes through screening and diabetes education. Weight control, Strict blood pressure and glycemic control essential for prevention of long-term complications of diabetes in under develop areas of Pa- kistan.
References
- Wild S, Roglic G, Green A, Sicree R, King H (2004) Global Prevalence of Diabetes: Estimates for the Year 2000 and Pro- jections for 2030. Diabetes Care 27: 1047-1053.
- International Diabetes Federation (IDF) (2016) Diabetes: A Global Emergency. The Global Picture. 7th Edition 51.
- Centers for Disease Control and Prevention (CDC) (2004) Prevalence of Overweight and Obesity among Adults with Di- agnosed Diabetes, United States, 1988-1994 and 1999-2002. Morbidity and Mortality Weekly Report 53: 1066-1068.
- Haider Z, Obaidullah S, Maqbool K (1980) Hypertension in Pakistani patients with diabetes mellitus. J Trop Med Hyg 83: 251-253.
- Haider Z, Obaidullah S (1981) Clinical diabetes mellitus in Pakistan. J Trop Med Hyg 84: 155-158.
- Shera AS, Rafique G, Khwaja IA, Ara J, Baqai S, et al. (1995) Pakistan national diabetes survey: prevalence of glucose in- tolerance and associated factors in Shikarpur, Sindh Province. Diabet Med 12: 1116-1121.
- Shera AS, Rafique G, Ahmed KI, Baqai S, Khan IA, et al. (1999) Pakistan National Diabetes Survey prevalence of glucose intolerance and associated factors in North West at Frontier Province (NWFP) of Pakistan. J Pak Med Assoc 49: 206-211.
- Shera AS, Rafique G, Khawaja IA, Baqai S, King H (1999) Pakistan National Diabetes Survey: prevalence of glucose in- tolerance and associated factors in Baluchistan province. Dia- betes Res Clin Pract 44: 49-58.
- Wee CC, Hamel MB, Huang A, Davis RB, Mittlemn MA, et al. (2008) Obesity and Undiagnosed Diabetes in the U.S. Dia- betes Care 31: 1813-1815.
- Basit A, Hydrie MZI, Ahmed K, Hakeem R (2002) Preva- lence of Diabetes, Impaired Fasting Glucose and associated risk factors in a rural area of Baluchistan province according to new ADA Criteria. J Pak Med Assoc 52: 351-360.
- The Asia-Pacific perspective: redefining obesity and its treat- ment, WHO.
- Parvez Hossain, Bisher Kawar, Meguid El Nahas (2007) Obe- sity and Diabetes in the Developing World- A Growing Chal- lenge. N Engl J Med 356: 213-215.
- Vazquez G, Duval S, Jacobs DR, Silventoinen, K (2007) Com- parison of Body Mass Index, Waist Circumference, and Waist/ Hip Ratio in Predicting Incident Diabetes: A Meta-Analysis. Epidemiol Rev 29: 115-128.
- Murray CJL, Lopez AD (1997) Mortality by cause for eight regions of the world: Global burden of disease study. Lancet 349: 1269-1276.
- Jafar TH, Jessani S, Jafary FH, Ishaq M, Orakzai R, et al. (2005) General practitioner’s approach to hypertension in urban Pakistan: disturbing trend in practice. Circulation 111: 1278-1283.
- Jafar TH, Levey AS, Jafary FH, White F, Gul A, et al. (2003) Ethnic subgroup differences in hypertension in Pakistan. J Hypertens 21: 905-912.
- Rahman S, Nasir K, Hussain ZJ, Shujaat A, Zafar IM (2006) Non-occupational lead exposure and hypertension in Paki- stani adults. J Zhejiang Univ Sci B 7: 732-737.
- Saydah SH, Geiss LS, Tierney Ed, Benjamin SM, Engelgau M, et al. (2004) Review of the performance of methods to identify diabetes cases among vital statistics, administrative, and survey data. Ann Epidemiol 14: 507-516.
- U.S. Preventive Services Task Force (2008) Screening: Type 2 Diabetes Mellitus in Adults.
- Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, et al. (2002) Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 346: 393-403.
- Osaimi S, AL-Gelban KS (2007) Diabetes Mellitus-Preva- lence and Associated Cardiovascular Risk Factors in a Saudi Sub-Urban Community. Biomedical Research 18: 147-153.
- Gregg EW, Cadwell BL, Cheng YJ, Cowie CC, Williams DE, et al. (2004) Trends in the prevalence and ratio of diagnosed to undiagnosed diabetes according to obesity levels in the U.S. Diabetes Care 27: 2806-2812.
- Hu FB (2003) Sedentary Lifestyle and Risk of Obesity and Type 2 Diabetes. Lipids 38: 103-108.
- UKPDS Group (1998) Intensive blood glucose control with sulphonylureas or insulin compared with conventional treat- ment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 352: 837-853.
- UKPDS Group (1998) Effect of intensive blood-glucose con- trol with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 352: 854-865.
- Wildman RP, Gu D, Reynolds K, Duan X, He J (2004) Appro- priate Body Mass Index and Waist Circumference Cutoffs for Categorization of Overweight and Central Adiposity among Chinese Adults. Am J Clin Nutr 80: 1129-1136.