
International Journal of Preventive Medicine and Care(IJPMC)
ISSN: 2994-032X | DOI: 10.33140/IJPMC

Research Article - (2025) Volume 3, Issue 1
Pathogen Prevalence Following Cervical Cerclage Insertion in High-Risk Singleton Pregnancies: Maternal and Fetal Outcomes
2Omidcarenet Inc, Calgary, Canada
Received Date: Jan 17, 2025 / Accepted Date: Feb 13, 2025 / Published Date: Feb 18, 2025
Copyright: ©Â©2025 Adedipe T.O, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Adedipe T.O., Chukwujama U.O., Adedipe A.O. (2025). Pathogen prevalence following cervical cerclage insertion in high-risk singleton pregnancies: Maternal and fetal outcomes. Int J Prev Med Care, 3(1), 01-07.
Abstract
Background: Cervical cerclage is a recognised treatment for cervical incompetence which carries a risk of preterm labour. Pathogen prevalence in post-cerclage populations is variable with varying outcomes on preterm birth. There is no strong guidance on screening this group of high-risk patients.
Methods: A single-centre retrospective study of singleton pregnancies that underwent a vaginal cerclage (n-45) for history- indicated (n-11), ultrasound- indicated(n-24) and physical examination -indicated reasons (n-10). Urogenital microbial assays were performed pre- and every 2-4 weeks in the post-cerclage cerclage period. Treatment depended on colony size, microbial sensitivity and recurrence vis-a-vis clinical symptomatology.
Primary aim was to identify global pathogen prevalence, pregnancy outcomes for individual arms of the cerclage placement, and identify the preterm birth risk <34 weeks gestational age having excluded other obstetric causes: with the secondary objective of identifying feto-maternal morbidity/ mortality.
Results: Age range of the cohort was 22-42 years with a median of 31 years. Positive post-cerclage urogenital cultures were identified in 80% of the population with the largest incidence in the ultrasound-indicated group. Birth after 34 weeks GA, gestational latency and birth-weights were reported in 84.6%, 78.3%, 71.4%: 144.2days, 118.7days, 109.5days: 2.98kg, 2.89kg, 2.4kg in the history-indicated, Ultrasound-indicated and physical-examination indicated groups respectively. There was a 2.8 times increased risk of delivery <34 weeks GA with a positive pathogen presence. (p= 0.042). The most common organisms were Candida spp, Group B Streptococcus and Escherichia Coli
Conclusions: There is a significant urogenital pathogen prevalence in post-cervical cerclage patients, with the ensuing risk of poor feto-maternal outcomes. Serial urogenital infection screening is a useful adjunct in the management algorithm which takes on board, timing and type of suture insertion with background obstetric risks, to mitigate cerclage failure and optimise fetomaternal outcomes.
Keywords
Preterm Birth, Cerclage, Infection, Vaginal Microbiome, Pregnancy Outcome, Urogenital Pathogen, Prematurity, Progesterone, Uterine Cervix
Introduction
Cervicalcerclage is a recognised treatment of cervical incompetence, a significant cause of preterm birth with associated sequelae which include significant neonatal morbidity such as long-term disability among survivors, including neurodevelopmental and cognitive disorders, visual and hearing impairment, motor disorders, risk of severe infections, long-term metabolic, cardiovascular, and mental health disorders, contributing to 40% of cerebral palsy cases, according to a population-based study with a £3billion cost within the United Kingdom NHS and resulting in considerable neonatal mortality. Preterm birth which occurs in 9.6% of pregnancies, is the delivery of a fetus before 37 completed weeks (1-3).
Cervical cerclages can be history-indicated, ultrasound -indicated and physical examination- indicated. Compared to progesterone use for preterm birth prevention, efficacy of a cerclage is equivocal and should be considered after robust risk assessment in line with the FIGO guidelines [4-7].
History- indicated cerclage can be offered following a history of several mid-trimester losses whilst an ultrasound-indicated cerclage is usually indicated for cases with a cervical length below 25mm in a singleton pregnancy and below 15mm in a multiple gestation pregnancy. However, ongoing research support a growing consensus towards adoption of a cervical length of 15mm in all pregnancies. Physical examination-indicated cerclage is offered when an open cervical os with or without fetal membrane prolapse, is seen on speculum examination.
Cerclages can be placed vaginally or abdominally. Whilst abdominally-placed cerclages can be placed pre-conceptually and largely in the 1st trimester, vaginal cerclages are placed usually between 13-24 weeks with a possible consideration up to 27+6 weeks in the physical examination -indicated cohort, following individualized assessment. This is in response to a considerable reduction of preterm birth with a resulting difference in neonatal morbidity outcomes associated with delivery of the severely preterm as compared to a moderately preterm baby, in the absence of infection, as a sequelae of an incompetent cervix [3,5-9]. The estimated healthcare costs of a preterm baby surviving to the age of 18 triples for a very preterm baby and quadruples for an extremely preterm baby [3]. In addition, prolonged hospital admission, maternal morbidity risks of infection, sepsis and thrombotic events are important factors to be considered when utilizing an expectant management approach rather than a rescue Cerclage in this cohort of patients.
Other treatments for preterm birth prevention with varying success rates, include the use of Progesterone, vaginal placement of the Arabin pessary, and antibiotic treatment where indicated.
Post-cerclage insertion clinical surveillance is variable as per timing, type and frequency of interventions: and is usually in response to primary indication and sometimes driven by ongoing clinical context. Anecdotally, women with an elective cerclage may not have as many episodes of monitoring or interventions as compared to those with Rescue / Ultrasound-indicated cerclages in the absence of other obstetric concerns.
Though there is no strong guidance regarding post-operative follow-up, there is benefit from monitoring for all the factors that contribute in different degrees to the pathophysiology modelling leading to preterm birth which include Infection/ inflammation/ incompetent cervix/ disrupted progesterone-mediated action and additional obstetric/ iatrogenic factors.
This paper focuses on the presence of infection/ inflammation triggers listed below which include vaginal dysbiosis, urinary tract infections and genital tract infections- pre-existing, persistent and opportunistic.
Vaginal ecosystem surveillance is of benefit as it is well known that vaginal dysbiosis is linked with preterm labor and is often a contributing primary factor, given increased inflammatory response and premature cervical remodeling. An incompetent cervix provides inadequate mechanical support for the ongoing pregnancy, leading to further loss or disruption of the cervicovaginal barrier and cervical mucus, with inadequate prevention of ascending infection. This is further complicated with an ascending and evolving cervicovaginal dysbiosis with an increased risk of amnionitis/ funisitis [9-11].
Lower genital tract infection singularly is a recognized cause of Preterm labor.
Urinary tract infections increase preterm birth risk by as much as 1.4-2.0 times according to large population studies: one which involved close to 3 million hospital admissions [12,13]. However, women may not always be symptomatic given a 2-10% prevalence of asymptomatic bacteriuria with a concurrent 30% incidence of pyelonephritis leading to increased preterm birth, requiring antibiotic suppression till term [12-14]. Though a meta-analyses and systematic review showed antibiotic use in cases of asymptomatic bacteriuria reduced pyelonephritis, low birthweight babies and preterm birth, the estimate of the effect was uncertain due to the low-quality evidence [14].
Urogenital microbial screening is of benefit, particularly for those asymptomatic but high-risk women. Mitigating against the limitations of previous studies which included lack of homogeneity, lack of guidance as to timing and frequency of testing samples, clinical relevance of lower colony counts and impact of different pathogens some of whom are ubiquitous to the vagina, and regular screening use in a low-risk population, may help improve clinical outcomes and effect [14].
Vaginal dysbiosis risk, coexisting or opportunistic lower genital tract infection can be identified with regular wet mount microscopy of vaginal swab samples or the use of other infection screening tools such as urine and genital swab microscopy, to facilitate prompt treatment which may include antibiotics.
Methods And Materials
This study carried out a single-center retrospective review of electronic patient records alongside microbiological assays - urine and genital swabs, performed every 2-4 weeks- of 45 consecutive patients who attended a vaginally placed high cervical cerclage or occlusion cerclage in 2 cases under the care of 1 surgeon supported post-operatively with ongoing Preterm Prevention input alongside other Obstetric interventions over a 2year period ending February 2023.
The cerclages were placed from 13 to 27+4 weeks gestational age following negative urogenital assays and/ or exclusion of ongoing infection. Routine amniocentesis was not included as part of the local protocol whilst exclusion criteria for cerclage placement included multiple gestation, preterm labor signs, vaginal bleeding,chorioamnionitis, non-viable fetus and diagnosed lethal fetal anomalies. Literature review of Post-Cerclage infection using PubMed, Medline and other databases to identify and inform current practice, was performed.
Pre-cerclage failed progesterone therapy or mitigating obstetric concerns such as poorly controlled diabetes preceding surgery were identified.
Cerclage insertion protocol was similar to a previously described protocol whilst urogenital microbiological assays were performed in asymptomatic persons, pre-operatively and post-operatively in a 2-4 weekly fashion till 36- 37 weeks at the time of cerclage removal, sometimes supported by hematological tests if indicated [15].
Adjunctive use of progesterone and reduced physical activity relative to their situation, with militant management of other obstetric concerns was performed.
Institutional ethics obtained for this retrospective study, was designed to look at primary objectives of cerclage success: (birth after 34 weeks GA) depending on indication and impact of pathogen presence in different cohorts with a sub-group analysis of gestational latency ( time delay from diagnosis of cervical incompetence to birth) in relation to vaginal fetal membrane prolapse. Statistics was by Excel Microsoft Corporation. (2018) . and Claude 3.5 Sonnet (October 2024 version), Anthropic accessed on January 9th, 2025
Results
There were 45 participants with an age range of 22-42yrs with a median of 31 years.
Previous Mid-trimester deliveries (22.2%) were the commonest contributor followed by a short cervix (<25mm) in 17.7%.
The distribution of the group is in table 1- with cerclage success listed accordingly, below.
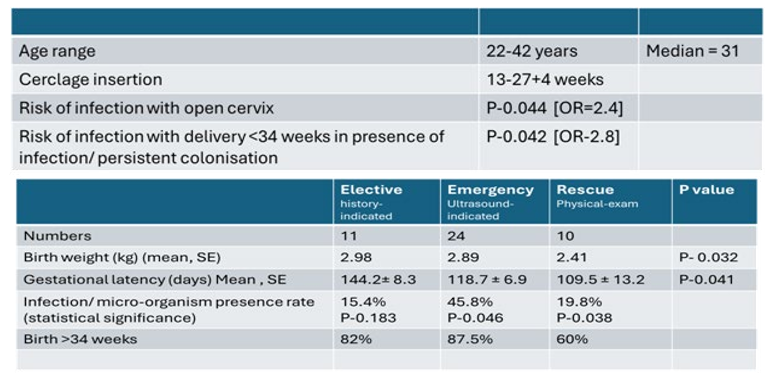
Table 1: Demographics and Outcomes/ Cerclage Cohort
Pathogen prevalence was 80%, with overall maternal infection requiring systemic intravenous antibiotics and antifungals in 13.3%; and a 4.4% miscarriage rate.
Pathogen prevalence rates were 15.4%, 45.8% and 60% in the history-indicated, ultrasound-indicated and physical examination-indicated cerclage groups consecutively with Gestational latencies of 144.2; 118.7; 109.5 days respectively.
Analysis of the infections showed a prevalence of genital Candidiasis (35.5%) alongside E Coli, Trichomonas, Enterococcus and Group B Streptococcus. These infections were seen mostly in the ultrasound-indicated cerclage cohort.

Table 2: Organisms and Prevalence Globally
Maternal outcomes include 27 episodes (60%) of maternal infection which included Klebsiella, Pseudomonas, E. coli UTIs and heavy vaginal Candida growth which were treated accordingly. There were 4 episodes of asymptomatic bacteriuria, 3 UTIs- with mild symptoms, 1 Sexualy Transmitted Infection and a case of pyelonephritis in a severely obese, poorly controlled type 2 Diabetic with polyhydramnios. She responded to IV antibiotic use, going on to deliver a 3.6kg baby at 35 weeks, 4 weeks after antibiotic treatment. This reiterated the need for screening despite having received a history-indicated cerclage with no initial concerning urogenital colonisation.

However, in the physical examination-indicated cerclage the outcomes were varied as seen in the table above. Poor fetal outcomes following a short gestational latency were often seen in those with fetal membrane prolapse to middle or lower third of the vagina, resulting in significant maternal infections in 13.3%.
Discussion
Post-Cerclage infection screening has not been addressed robustly in literature. This in addition to several widely available patient advice leaflets which often state a post-operative return to normal activities which include swimming, and conjugal relations, there are concerns about possible de Novo/ occult infection which largely goes unrecognised without adequate urogenital screening. Patient expectations often collide with clinical advice given the contrasting patient information available in print and elictronic media [16]. There are varied datasets regarding pathogen prevalence in literature with Romero et al stating as much as 50% following amniocentesis.
As there is a strong association between urogenital pathogen prevalence and adverse pregnancy outcomes, effective screening and treatment interventions in this cohort of high-risk women should offer some degree of protection, as it is recognised that infection escalates quickly from a subclinical status to preterm membrane rupture with possible preterm labour, poor neonatal and maternal outcomes [9-11].
There is recognised association between a short or incompetent cervix and intra-amniotic inflammation or infection but limited data identifying a strong correlation between post-cerclage insertion with increased pathogen prevalence as a cause of ensuing preterm birth alone as there are often other confounding factors such as isolated peri-operative risks, fetal wellbeing problems and other obstetric challenges [9,10].
Despite lack of confirmatory causation data, a cautious approach using serial cost-effective, non-invasive tools such as urogenital assays should be considered given our findings of 80% pathogen prevalence and a 2.8 times increased risk of associated birth before 34 weeks GA. Our prevalence seems to be in keeping with mainstream literature but differs from the study by Seys et al, which stipulated a 43% prevalence and a statistically relevant lack of benefit with antibiotic therapy or serial routine urogenital cultures of asymptomatic women post cerclage insertion [17].
In our study, we observed that the commonest prevalence was Candida (35.5%) followed by Group B Streptococcus (15.5%) and Escherichia Coli (13.3%).
There was a case of post-cerclage insertion asymptomatic new-onset vaginal Trichomonas infection and another: - E Coli Pyelonephritis in a very poorly controlled and severely obese type 2 diabetic mother with a previous 22-week fetal loss. Both cases were promptly treated, resulting in good outcomes.
Candida, E Coli, Group B Streptococcus and Pseudomonas aeruginosa were observed to be the prevailing organisms in miscarriages and deliveries before 34 weeks GA.
However, preterm birth etiology is often a mix of varying degrees of inflammation, infection and cervical incompetency with dysfunctional progesterone-mediated activity:- a postulation supported by several animal and human studies. This supports the role of adjunctive progesterone use, in this group of women, as there is growing evidence to suggest a beneficial role of progesterone as a treatment for cervical incompetence, an adjunct to a cervical cerclage and treatment for failed cerclages [15,18-20].
Though there were 6 cyclogest failures in our cohort prior to the cerclage insertion, all the women were placed on regular vaginal progesterone (the locally available option) as adjunctive therapy except one who had reported a sensitivity reaction. Risk factors such as vaginal soreness, excessive discharge, labile moods, impaired glucose metabolism were carefully monitored and mitigated.
We reported 4 cases of membrane rupture: 2 of whom resulted in non-viable fetal losses and deliveries of live fetuses at 28 and 33 weeks, both of whom occurred many days after initial membrane rupture. Both babies were discharged home and currently doing well after treatment for infection and prematurity- related concerns The option of delaying removal of a cerclage following a preterm membrane rupture should be considered after a risk-benefit assessment given the sequelae or effects of severe prematurity. A recent meta-analysis suggests a careful consideration of continuing with pregnancy given extreme to severe prematurity- related concerns, in the absence of contractions as there was no difference in maternal and perinatal outcomes once initial chorioamnionitis risk and low APGAR scores were excluded [21].
The type of pathogen on urogenital assay might also play a part in prognostication and is addressed below, with a focus on the 3 most prevalent pathogenic strains, described below.
Candida SPP
Largely considered a vaginal commensal, with morbidity limited to persistent discharge and vaginitis-related symptoms, there have been a few reported cases of adverse outcomes. Poliquin et al described 3 cases of poor fetal outcomes and significant maternal infections following post-cerclage Candida albicans infection/ colonization despite pre-cerclage negative cultures. This is a rare prevalence of intra-amniotic infection risk given its ubiquity in the vagina demonstrated to be a 0.65% prevalence in 773 amniocentesis samples [22,23].
E Coli E.
coli is one of the commonest infections in pregnancy (43% prevalence in a retrospective study in Australia) and can be transmitted from poor hygiene, eating undercooked meat, swimming in infected waters, close contact with infected animals and usually presents as bloody diarrhoea. However serious sequelae such as maternal sepsis, preterm birth and low birth weight with hemolytic uremic syndrome have been reported [24,25]. Jin et al postulated the need for infection screening as they identified an association between the ultrasound -indicated group (short cervix) and a post-cerclage vaginal acquisition of Escherichia coli and mixed anaerobes; with each colony having a statistically significant association with preterm birth. In addition, previously acquired and persistent E. coli infection showed an association with birth before 37 weeks whilst post-cerclage-acquired mixed anaerobes and recently acquired E. coli showed an association with birth before 34 weeks [25].
Group B Streptococcus
Though a vaginal colonization- usually asymptomatic- is not associated with maternal morbidity, associations with chorioamnionitis and early onset neonatal sepsis are well recognized. A systematic review and meta-analyses suggest there is evidence that preterm birth is associated with maternal GBS colonization, especially in scenarios of ascending infection (bacteriuria) as might be found with a short/ incompetent cervix. They arrived at a consensus that though there were limitations brought on by confounders, the associated burden of neonatal morbidity and mortality, could not be ignored [26].
Open Cervix with Membrane Prolapse
There was a 2.4 increased risk of preterm birth < 34 weeks in women who had a physical examination-indicated cerclage in this study. Pathogen prevalence which was higher for both the ultrasound-indicated and Physical examination-indicated cerclage cohort as compared to History-indicated cerclage; was found to be statistically significant. In addition, 2 significant predictors of poor outcomes for the group with an open cervix, were fetal membrane prolapse into lower and middle third of the vagina and type +/-persistence of organism, which is historically well-recognised.
Conclusions
There is a significant urogenital pathogen prevalence in post-cervical cerclage parturient, with ensuing poor feto-maternal outcomes. Serial urogenital infection screening which is less invasive than amniocentesis, is a useful adjunct in the management algorithm which takes on board, timing and type of suture insertion with background obstetric risks, to mitigate cerclage failure and optimise fetomaternal outcomes. This area needs further work to enable guideline formulation. Regular urogenital screening is affordable and transferable, particularly in the low-resource setting.
Limitations
Limitations of this study, include the small sample size with co-existing significant poor obstetric outcome confounders though some statistically significant associations have been identified to further characterize the at-risk group.
Serum leucocyte count was not routinely offered unless clinically indicated. Whether it might help identify a small group with subacute chorioamnionitis following a hematogenous spread secondary to factors such as non-genital etiology systemic infection or poor periodontal care as seen in smokers, is yet to be established.
Unavailability of the wet mount microscopy limited opportunities to identify all cases of vaginal dysbiosis with no formal pathogen presence whilst current advances in Microbiome typing in pregnancy and other ongoing research, might provide additional information to further identify those at significant risk.
This paper supports the role of infection screening in this group of women.
Limitations
Limitations of this study, include the small sample size with co-existing significant poor obstetric outcome confounders though some statistically significant associations have been identified to further characterize the at-risk group.
Serum leucocyte count was not routinely offered unless clinically indicated. Whether it might help identify a small group with subacute chorioamnionitis following a hematogenous spread secondary to factors such as non-genital etiology systemic infection or poor periodontal care as seen in smokers, is yet to be established.
Unavailability of the wet mount microscopy limited opportunities to identify all cases of vaginal dysbiosis with no formal pathogen presence whilst current advances in Microbiome typing in pregnancy and other ongoing research, might provide additional information to further identify those at significant risk.
This paper supports the role of infection screening in this group of women.
No Declarations
TOA designed the study, collected the data and wrote the paper, UOC helped with corrections whilst AOA delivered on statistics
References
- Blencowe, H., Lee, A. C., Cousens, S., Bahalim, A., Narwal, R., Zhong, N., ... & Lawn, J. E. (2013). Preterm birth–associated neurodevelopmental impairment estimates at regional and global levels for 2010. Pediatric research, 74(1), 17-34.
- Chen, R., Sjölander, A., Johansson, S., Lu, D., Razaz, N., Tedroff, K., ... & Cnattingius, S. (2021). Impact of gestational age on risk of cerebral palsy: unravelling the role of neonatal morbidity. International journal of epidemiology, 50(6), 1852-1863.
- Mangham, L. J., Petrou, S., Doyle, L. W., Draper, E. S., & Marlow, N. (2009). The cost of preterm birth throughout childhood in England and Wales. Pediatrics, 123(2), e312-e327.
- Shennan, A., Story, L., Jacobsson, B., Grobman, W. A., FIGO Working Group for Preterm Birth, Simpson, J. L., ... & Mol, B.W. (2021). FIGO good practice recommendations on cervical cerclage for prevention of preterm birth. International Journal of Gynecology & Obstetrics, 155(1), 19-22.
- Namouz, S., Porat, S., Okun, N., Windrim, R., & Farine, D. (2013). Emergency cerclage: literature review. Obstetrical & gynecological survey, 68(5), 379-388.
- Wierzchowska-Opoka, M., Kimber-Trojnar, Å»., & LeszczyÅ?ska-Gorzelak, B. (2021). Emergency cervical cerclage. Journal of clinical medicine, 10(6), 1270.
- Alfirevic, Z., Stampalija, T., & Medley, N. (2017). Cervical stitch (cerclage) for preventing preterm birth in singleton pregnancy. Cochrane database of systematic reviews, (6).
- Gulersen, M., Lenchner, E., Nicolaides, K. H., Otsuki, K., Rust, O. A., Althuisius, S., ... & Berghella, V. (2023). Cervical cerclage for short cervix at 24 to 26 weeks of gestation: systematic review and meta-analysis of randomized controlled trials using individual patient-level data. American journal of obstetrics & gynecology MFM, 5(6), 100930.
- Romero, R., Gonzalez, R., Sepulveda, W., Brandt, F., Ramirez, M., Sorokin, Y., ... & Cotton, D. B. (1992). Infection and labor: VIII. Microbial invasion of the amniotic cavity in patients with suspected cervical incompetence: prevalenceand clinical significance. American journal of obstetrics andgynecology, 167(4), 1086-1091.
- Lee, S. E., Romero, R., Park, C. W., Jun, J. K., & Yoon, B.H. (2008). The frequency and significance of intraamniotic inflammation in patients with cervical insufficiency. American journal of obstetrics and gynecology, 198(6), 633-e1.
- Galaz, J., Romero, R., Greenberg, J. M., Theis, K. R., Arenas-Hernandez, M., Xu, Y., ... & Gomez-Lopez, N. (2023). Host-microbiome interactions in distinct subsets of preterm labor and birth. Iscience, 26(12).
- Qobadi, M., & Dehghanifirouzabadi, A. (2015). Urinary tract infection (UTI) and its association with preterm labor: Findings from the Mississippi Pregnancy Risk Assessment Monitoring System (PRAMS), 2009–2011. Open Forum Infectious Diseases, 2(suppl_1).
- Baer, R. J., Nidey, N., Bandoli, G., Chambers, B. D., Chambers,C. D., Feuer, S., ... & Jelliffe-Pawlowski, L. L. (2021). Risk of early birth among women with a urinary tract infection: a retrospective cohort study. American journal of perinatology reports, 11(01), e5-e14.
- Smaill, F. M., & Vazquez, J. C. (2019). Antibiotics for asymptomatic bacteriuria in pregnancy. Cochrane database of systematic reviews, (11).
- Adedipe, T. O., Akintunde, A. A., & Chukwujama, U. O. (2022). Management of an incompetent mid-second (mid-2nd) trimester absent ecto-cervix: a case series. Cervical amplification pre-cerclage insertion. Archives of Gynecology and Obstetrics, 306(4), 969-975.
- Adedipe T.O Assessing patient information leaflets on cervicalcerclage treatment ( to be published).
- Seys, E., Page, A. S., Deprest, J., Lannoo, L., van Calsteren, K., Devlieger, R., & van der Merwe, J. (2024). Urogenital cultures and preterm birth in women with cervical cerclage: a single center retrospective cohort study. BMC Pregnancy and Childbirth, 24(1), 324.
- Conde-Agudelo, A., Romero, R., Da Fonseca, E., O’Brien,J. M., Cetingoz, E., Creasy, G. W., ... & Nicolaides, K. H. (2018). Vaginal progesterone is as effective as cervical cerclage to prevent preterm birth in women with a singleton gestation, previous spontaneous preterm birth, and a short cervix: updated indirect comparison meta-analysis. American journal of obstetrics and gynecology, 219(1), 10-25.
- Roman, A., Da Silva Costa, F., Júnior, E. A., & Sheehan, P. (2018). Rescue adjuvant vaginal progesterone may improve outcomes in cervical cerclage failure. Geburtshilfe Und Frauenheilkunde, 78(08), 785–790.
- Fonseca, E. B., Celik, E., Parra, M., Singh, M., & Nicolaides, K.H. (2007). Progesterone and the Risk of Preterm Birth among Women With a Short Cervix. Obstetrical & Gynecological Survey, 62(12), 769.
- Zullo, F., Di Mascio, D., Chauhan, S. P., Chrysostomou, S., Suff, N., Pecorini, F., ... & Brunelli, R. (2023). Removal versus retention of cervical cerclage with preterm prelabor rupture of membranes: Systematic review and meta-analysis. European Journal of Obstetrics & Gynecology and Reproductive Biology, 288, 83-89.
- Poliquin, V., Al-Sulmi, E., & Menticoglou, S. (2015). Intraâ?Amniotic Infection Involving Candida albicans Subsequent to Emergency Cerclage: A Case Series. Canadian Journal of Infectious Diseases and Medical Microbiology, 26(5), 245-246.
- Chaim, W., Mazor, M., & Wiznitzer, A. (1992). The prevalence and clinical significance of intraamniotic infection with Candida species in women with preterm labor. Archives of gynecology and obstetrics, 251, 9-15. 1992;251:9–15.
- Mother To Baby | Fact Sheets [Internet]. Brentwood (TN): Organization of Teratology Information Specialists (OTIS);1994-. Escherichia coli (E. coli) 2023 Apr.
- Jin, W., Hughes, K., Sim, S., Shemer, S., & Sheehan, P. M. (2022). Abnormal vaginal flora and spontaneous preterm birth in high-risk singleton pregnancies with cervical cerclage. The Journal of Maternal-Fetal & Neonatal Medicine, 35(25), 9983-9990.
- Bianchi-Jassir, F., Seale, A. C., Kohli-Lynch, M., Lawn,J. E., Baker, C. J., Bartlett, L., ... & Rubens, C. E. (2017). Preterm birth associated with group B Streptococcus maternal colonization worldwide: systematic review and meta-analyses. Clinical Infectious Diseases, 65(suppl_2), S133-S142.