
International Journal of Cancer Research & Therapy(IJCRT)
ISSN: 2476-2377 | DOI: 10.33140/IJCRT
Impact Factor: 1.3

Case Report - (2024) Volume 9, Issue 2
Low Grade Fibro-Myxoid Sarcoma: A Case Report on MUC4 as A Novel Immunohistochemistry Marker to Detect this Benign Mimic of Malignant Neoplasm
2Dr. Lal PathLabs Ltd., National Reference Lab, India
Received Date: May 02, 2024 / Accepted Date: May 27, 2024 / Published Date: Jun 10, 2024
Copyright: ©Â©2024 Sumedha Dey, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Sumedha, D., Jayitri, D., Zeenat, A., Monika, P., Mallika, G., et al. (2024). Low Grade Fibro-Myxoid Sarcoma: A Case Report on MUC4 as A Novel Immunohistochemistry Marker to Detect this Benign Mimic of Malignant Neoplasm. Int J Cancer Res Ther, 9(2), 01-07.
Abstract
Low-grade fibromyxoid sarcoma(LGFMS) is a rare type of malignant fibroblastic and myofibroblastic tumor that is characterized by benign appearing histologic features but with a paradoxically aggressive clinical course and metastasis. These tumors generally occur in young and middle aged adults. Most common sites of involvement are proximal extremities and trunk and are usually subfascial in-depth. Less common locations include central body sites and superficial soft tissues. It has a male predilection. Here we describe a case of low-grade fibromyxoid sarcoma affecting the left thumb of a 39 year old male . The duration of the disease spans over 2 years with one history of recurrence after excision. On gross examination the specimen was firm, irregular, elongated swelling measuring 3.5 x 2 x 1 cm. Microscopically the tumor was composed of collagenous hypocellular areas alternating with hypercellular myxoid areas in nodules with abrupt transition between the two. Immunohistochemistry revealed strong positivity for Vimentin, CD99, focal SMA and very strong cytoplasmic positivity for MUC4 confirming the diagnosis of low-grade fibromyxoid sarcoma. After initial healing of the surgical wound, the patient went for radiotherapy and there is no recurrence till date. However long-term follow up is necessary as there is history of metastasis that has occurred as long as 45 years after primary excision.
Keywords
Low-Grade Fibro-Myxoid Sarcoma, Proximal Extremity, Recurrence, Metastasis, Immunohistochemistry
Introduction
Low-grade fibromyxoid sarcoma as described by Evans in 1987, is a rare variant of fibrosarcoma with high metastasizing potential despite the benign histologic appearance [1,2]. Tumor usually occurs in proximal extremities and trunk. It is usually subfascial in-depth. Less common locations include abdominal cavity, retroperitoneum, mediastinum, and superficial soft tissues with latter being relatively more common in children [3]. It is rare in head and neck areas [4]. Although rare among sarcomas the true incidence was underestimated before the availability of ancilliary diagnostic markers and due to its propensity to mimic other benign soft tissue neoplasms. There is slight male predilection. The tumor generally occurs in young adults but the age ranges wide and as many as 20% of the cases occurs in patients less than 18 years of age.
The low-grade fibromyxoid sarcoma shows low rates of recurrence (10%) and metastasis (5%) in first 5 years after excision of the primary tumor . However rates are much higher with long-term follow up. Metastasis can occur as long as 45 years after primary excision and the median interval to tumor related deaths is 15 years [5]. The most common metastatic sites are lungs and pleura. Histological features do not correlate with clinical behavior.
MUC4 is a transmembrane or membrane bound mucin which provides a protective layer of mucus. It normally acts as a barrier to apical surface of epithelial cells, playing a protective and regulatory role. Positive staining is noted in tracheobronchial mucosa, colon, stomach, cervix, lung and normal salivary glands. Positive staining in disease is observed in pancreatic, colonic, pulmonary and gastric carcinoma. However, the tumor cells of low-grade fibro myxoid sarcoma shows strong, diffuse cytoplasmic expression of MUC4, an epithelial glycoprotein in approximately 99% of cases. MUC4 is highly sensitive and specific for low-grade fibro myxoid sarcoma and sclerosing epithelioid fibrosarcoma among the fibroblastic and myofibroblast tumors.
Here we describe a case of low-grade fibro myxoid sarcoma affecting the left thumb of a 39 year old male. The duration of the disease spans over 2 years with one history of recurrence after excision.
Materials and Methods
A 39 year old patient who is also a health care worker by profession presented with an irregular swelling in the radial aspect of his left thumb (Figure 1). On clinical examination the growth was irregular, elongated, fleshy and adhered to the underlying structures with restricted joint mobility. The skin over the tumor was taut and shiny but with no ulceration. For this he was referred for a musculoskeletal ultrasound where the lesion was reported as well defined, lobulated , hypoechoic lesion 35x12x9mm along radial aspect of thumb. Lesion showed increased vascularity and was closely adherent to flexor tendon sheath. Underlying bony cortex was intact. Possibility of tenosynovial giant cell tumour was reported. He had undergone operation and mass was excised but no histological examination was not done. The swelling reappeared within 2 months and repeat excision biopsy was performed and the specimen was sent for histopathology (Figure 2). Microscopically the tumour was composed of bland looking spindle cells with a certain pattern. There were collageneous hypocellular areas and more myxoid cellular nodules with abrupt transition between the two. The spindle cells are bland and arranged in a whirling pattern. Few arcades of small vessels with perivascular sclerosis seen. No increased mitosis, necrosis or cellular pleomorphism detected. (Figure 3a, b) It was reported as spindle cell neoplasm with advice of immunohistochemistry for further categorization. In the primary immunohistochemistry panel Vimentin was strongly positive (Figure 4), Ki67 was focally high (Figure 7), PAN CK and S100 were negative. In the next panel SOX 10 was negative , CD34 was positive in the arcades of blood vessels, SMA was positive, Beta catenin was negative, TLE-1 was negative and CD99 was strongly positive (Figure 5). In the last panel, Desmin was negative, EMA was positive and MUC4 showed strong cytoplasmic positivity thus confirming the diagnosis of low-grade fibro myxoid sarcoma(Figure 6). After initial healing of the surgical wound, the patient went for radiotherapy and there is no recurrence till date. The patient is under close follow up.

Figure 1: Clinical Presentation- Irregular Swelling of the Thumb

Figure 2: Macroscopy- Firm , Irregular Swelling
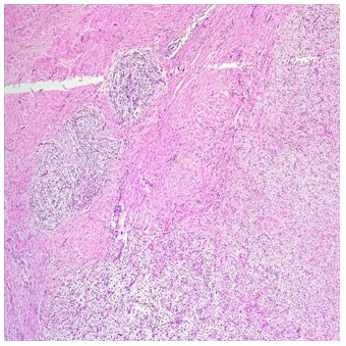
Figure 3a: HPE(10X)-Collageneous Hypocellular Areas with more Myxoid Cellular Nodules with Abrupt Transition Between the Two

Figure 3b: HPE(40X)-The Spindle Cells are Mostly Bland and Arranged in a Whirling Pattern.
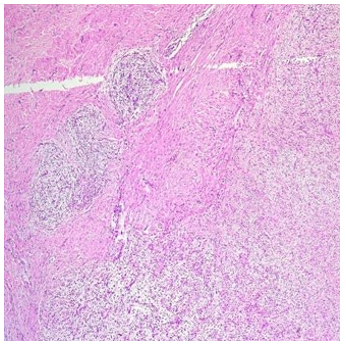
Figure 3a: HPE(10X)-Collageneous Hypocellular Areas with more Myxoid Cellular Nodules with Abrupt Transition Between the Two
Figure 3b: HPE(40X)-The Spindle Cells are Mostly Bland and Arranged in a Whirling Pattern.
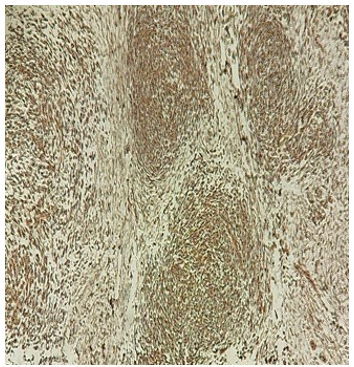
Figure 4: HPE 10X-Vimentin-Positive

Figure 5: HPE 40X-CD99-Positive
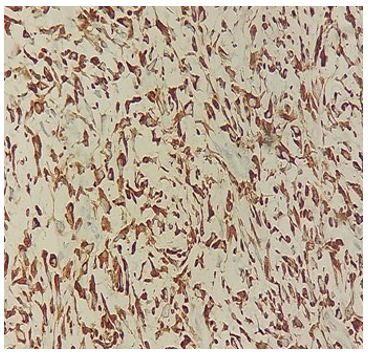
Figure 6: HPE (40X)-MUC4 –Strong and Diffuse Cytoplasmic Positivity

Figure 7: HPE (10X)- Ki67 Index Focally High
Discussion
Low grade fibro myxoid sarcoma is a malignant fibroblastic neoplasm characterized by alternating collagenous and myxoid areas with deceptively bland spindle cells with a whirling growth pattern and arcades of small vessels [2]. Most common site of involvement being proximal extremities and trunk, usually sub fascial in depth. Presentation is typically of a painless mass which can be present for >5years.There is slight male predominance and tumors typically arise in young adults but overall age range is wide with as many as 20% of cases occur in patients who are <18 years age. The cytogenetic hallmark of low grade fibro myxoid sarcoma is t (7;16) (q33; p11).Another 25% show supernumerary ring chromosomes. Both aberrations result in fusion of the 5' part of the FUS gene in 16p11 with the 3'part of CREB3L2 in 7q33; a chimeric FUS-CREB3L2 transcript is seen in >90% of the cases [6].
Macroscopically the tumors are well circumscribed, fibrous and often focally mucoid. Tumor size ranges from 1 to >20 cm in greatest dimension. Microscopically it is composed of collagenous hypocellular areas and more cellular myxoid nodules with abrupt transitioning between these two areas is typical. Tumor cells are bland, spindled and sometimes plump and they grow in short fascicles or in a whirling pattern. Mitotic activity is generally inconspicuous. Arcades of small vessels with perivascular sclerosis are seen. Approximately 30% of the cases contain collagen rosettes [7]. In some cases, areas of sclerosing epithelioid fibrosarcoma are present. Unusual patterns including focal pleomorphism or nuclear atypia, hypercellularity and heterotopic ossification is present in 10% of the cases [7]
By immunohistochemistry tumor cells show strong, diffuse and cytoplasmic expression of MUC4, an epithelial glycoprotein in 99% of the cases. MUC4 is highly sensitive and specific for low grade fibro myxoid sarcoma and sclerosing epithelioid fibrosarcoma among fibroblastic and neural tumors [8]. Expression of EMA is present in 80% of cases and focal expression of SMA in approximately 30% cases.
Diagnostic molecular pathology includes diagnosis of FUS gene re-arrangement [6].
Although low grade fibromyxoid sarcoma shows low rates of recurrence and metastasis in the first 5 years after excision of the primary tumor, rates are much higher with long term follow up. Most common site of metastasis is lung and pleura. Metastasis occurred as long as 45 years after primary excision (median being 5 years).Median interval from primary excision to tumor related death is 15 years. Histological features generally do not correlate with clinical behavior although tumors with areas of sclerosing epitheloid fibrosarcoma or round cell morphology tend to pursue a more aggressive clinical course. Differential diagnosis includes inflammatory myofibroblast tumor, low-grade myofibroblastic sarcoma, superficial CD34 positive fibroblastoma, myxoinflammatory fibroblastic sarcoma, adult fibrosarcoma, myxofibrosarcoma, sclerosing epithelioid sarcoma, desmoid fibromatosis, dermatofibrosarcoma protuberans, neurofibroma, perineuroma, neurothekoma, nodular fasciitis and acral superficial fibromyxoma [9].
References
- Folpe, A. L., Lane, K. L., Paull, G., & Weiss, S. W. (2000). Low-grade fibromyxoid sarcoma and hyalinizing spindle cell tumor with giant rosettes: a clinicopathologic study of 73 cases supporting their identity and assessing the impact of high-grade areas. The American journal of surgical pathology, 24(10), 1353-1360.
- Abe, Y., Hashimoto, I., & Nakanishi, H. (2012). Recurring facial low-grade fibromyxoid sarcoma in an elderly patient: a case report. The Journal of Medical Investigation, 59(3.4), 266-269.
- Billings, S. D., Giblen, G., & Fanburg-Smith, J. C. (2005). Superficial low-grade fibromyxoid sarcoma (Evans tumor): a clinicopathologic analysis of 19 cases with a unique observation in the pediatric population. The American journal of surgical pathology, 29(2), 204-210.
- Pandey, M., Thomas, G., Mathew, A., Abraham, E. K.,Somanathan, T., Ramadas, K., ... & Nair, M. K. (2000). Sarcoma of the oral and maxillofacial soft tissue in adults. European journal of surgical oncology, 26(2), 145-148.
- Evans, H. L. (2011). Low-grade fibromyxoid sarcoma: a clinicopathologic study of 33 cases with long-term follow-up. The American journal of surgical pathology, 35(10), 1450-1462.
- Lindberg, G. M., Maitra, A., Gokaslan, S. T., Saboorian, M. H., & Albores-Saavedra, J. (1999). Low grade fibromyxoid sarcoma: Fine-needle aspiration cytology with histologic, cytogenetic, immunohistochemical, and ultrastructural correlation. Cancer Cytopathology: Interdisciplinary International Journal of the American Cancer Society, 87(2), 75-82.
- Rekhi, B., Deshmukh, M., & Jambhekar, N. A. (2011). Low-grade fibromyxoid sarcoma: a clinicopathologic study of 18 cases, including histopathologic relationship with sclerosing epithelioid fibrosarcoma in a subset of cases. Annals of diagnostic pathology, 15(5), 303-311.
- Doyle, L. A., Möller, E., Dal Cin, P., Fletcher, C. D., Mertens, F., & Hornick, J. L. (2011). MUC4 is a highly sensitive and specific marker for low-grade fibromyxoid sarcoma. The American journal of surgical pathology, 35(5), 733-741.
- Qiu, X., Montgomery, E., & Sun, B. (2008). Inflammatory myofibroblastic tumor and low-grade myofibroblastic sarcoma: a comparative study of clinicopathologic features and further observations on the immunohistochemical profile of myofibroblasts. Human pathology, 39(6), 846-856.