
Dermatology Journal of Cosmetic and Laser Therapy(DJCLT)
ISSN: 2835-7329 | DOI: 10.33140/DJCLT
Impact Factor: 0.98



Case Report - (2024) Volume 3, Issue 2
Laser Therapy as a Treatment Option for the Cutaneous Manifestations of Erdheim-Chester Disease
2Department of Neurology, Memorial Sloan Kettering, Cancer Center, New York, NY, USA
Received Date: Jun 11, 2024 / Accepted Date: Jun 25, 2024 / Published Date: Jul 15, 2024
Copyright: ©Â©2024 Anthony M. Rossi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Wilson, B. N., Lavin, L., Aleisa, A., Diamond, E. L., Lacouture, M., et al. (2024). Laser Therapy as a Treatment Option for the Cutaneous Manifestations of Erdheim-Chester Disease. Dearma J Cosmetic Laser Therapy, 3(2), 01-04.
Abstract
Erdheim-Chester disease (ECD) is a rare non-Langerhans cell histiocytosis with systemic and cutaneous findings, characterized by the accumulation of lipid-laden histiocytes and stromal fibrosis. We report two cases presenting with infiltrative, histiocytic xanthelasma-like plaques referable to ECD, persistent following medical therapy and/or surgical therapy, that were successfully managed with fractional carbon dioxide (CO2) 10,600 nm laser ablation. Our patients experienced improvement without any adverse effects. Collaborative work between dermatologists and oncologists is essential when treating patients with persistent cutaneous manifestations of Erdheim-Chester disease. In conjunction with systemic treatment, fractional CO2 laser therapy is valuable treatment option for the elimination of the cutaneous manifestations of ECD.
Keywords
Erdheim-Chester Disease, Histiocytosis, Non-Langerhans-Cell, Laser Therapy, Xanthelasma-Like, Fractional Carbon Dioxide Laser
Introduction
Erdheim-Chester disease (ECD) is a rare non-Langerhans cell histiocytosis first described by Jakob Erdheim and William Chester in 1930 [1]. The disease is characterized by xanthoma- tous or xanthogranulomatous infiltrates containing foamy lip- id-laden histiocytes surrounded by inflammatory and/or fibrotic stroma [2]. On immunohistochemical staining these histiocytes are CD68+, CD163+, CD1a−, and Langerin (CD207)− [2]. Although the exact pathogenesis is unknown, high prevalence of BRAFV600E and other mitogen-activated protein kinase (MAPK) pathway mutations in ECD patients has led to the hy- pothesis that neoplasia drive by MAPK pathway signaling may play a role in the development of this disease [3].
ECD characteristically affects the long bones of the legs thus leading to the most commonly presenting symptom of bone pain [1]. Approximately 25% of patients present with cutaneous in- volvement with most manifestations presenting as skin-colored to yellowish indurated papules and plaques mimicking xan- thelasma palpebrarum [1,2]. There is limited literature available concerning management of the cutaneous manifestations of ECD beyond systemic interferon, cobimetinib, and vemurafenib [2,4]. Herein we present two patients with improved but residu- al cutaneous manifestations of ECD while on cobimetinib who were successfully treated using fractional carbon dioxide (CO2) laser ablation.
Report of Cases
Case 1: A 52-year-old woman with BRAFV600E-mutated Erdheim-Chester disease presented to dermatologic surgery due to multiple coalescing periorbital and perioral xanthelasma-like plaques (Figure 1). Other manifestations of ECD including xan- thelasma-like plaques on the extremities and chest, as well as osseous disease in the tibias, had been well managed with co- bimetinib. After management options were reviewed including observation, surgical removal, and laser therapy, the patient opt- ed for laser therapy. CBC with differential were within normal limits prior to the initiation of laser therapy. Two treatments with fractional 10,600nm CO2 laser (UltraPulse, Lumenis, San Jose, CA) were performed at 8-week intervals. Deep FX setting con- sisted of a single pass with a fluence of 17.5mJ, density level 10; active FX setting consisted of a single pass with a fluence of 70mJ, density level 3. After one fractional CO2 laser therapy session, lesion size, thickness, color, and texture had markedly improved (Figure 1b). She reported a significant improvement in her self-esteem and quality of life, rating results as excellent at her 8 week follow up. At her 2-year follow up, results were sus- tained, and the patient was satisfied with the results; the patient made note of the added benefit of skin tightening and reduced periocular and periorbital rhytids. The patient did continue with cobimetinib therapy, thus the sustained improvements in her cu- taneous manifestations could be partially attributed to this back- ground therapy.
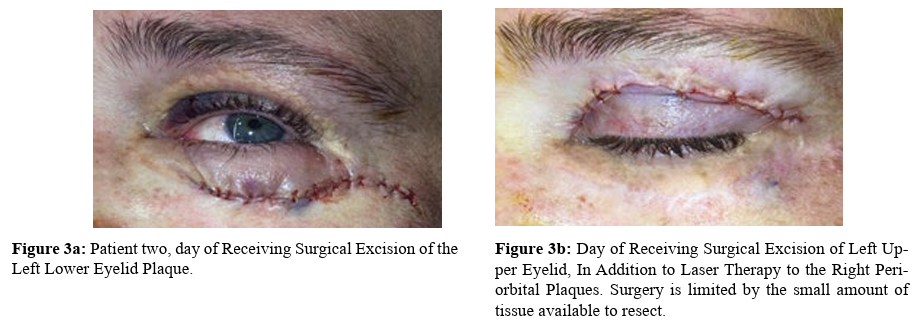
Case 2: A 42-year-old woman with BRAFV600-wildtype, MAP2K1-mutated Erdheim-Chester disease presented to derma- tologic surgery for the facial cutaneous manifestations of her dis- ease (Figure 2a-b). Treatment with cobimetinib failed to resolve the bilateral periorbital xanthelasmas, for which she presented to dermatologic surgery. Physical examination revealed bilateral periorbital yellow waxy papules and plaques. Prior medications targeting ECD, upper blepharoplasty, and surgical removal failed to improve the lesions in total. After management options were reviewed including observation, surgical re-attempt, and laser therapy, the patient consented to laser therapy. Complete bleed count (CBC) with differential were within normal limits prior to the initiation of laser therapy. Corneal shields were used for the patient. Substantial improvement was noted following only one treatment with a fractional 10,600nm CO2 laser (CO2RE, Candela, Marlborough, MA). Laser treatment utilized two pass- es of fusion settings with 40% fractional settings and a fluence of 60mj, wiping the char between passes. The patient was in- structed to utilize sun protection and to complete diluted acetic acid soaks and warm water washes daily to the affected area. At her four-week follow up, the patient noted satisfactory results consisting of improvement of the plaques bilaterally and perioc- ular skin tightening (Figure 2c-d). Two months later, the patient and physician opted to try a combination of laser therapy to the right periorbital plaques and surgical excision of the left lower eyelid plaque (Figure 3A). A follow-up visit three months later revealed substantial improvement (Figure 2c). A combination of laser therapy and surgical excision was performed once again, this time with surgical excision of the left upper eyelid plaque (Figure 3b), in addition to laser therapy to the right periorbital plaques at the same time. A follow-up visit four months later once again revealed substantial clearing and improvement (Fig- ure 2d-e). There were no adverse events reported or noted. The patient remains interested in continuing treatments as needed.
Discussion
In this report, we present two patients with cutaneous manifesta- tions of Erdheim-Chester disease persisting after medical and/or surgical therapy, successfully treated using fractional CO2 laser ablation. With the exception of a brief image correspondence, there is a paucity of publications documenting treatment of the cutaneous manifestations of ECD with laser therapy [5]. This correspondence featured a 53-year-old male with bilateral yel- low periocular nodules refractory to interferon-α, anakinra and vemurafenib successfully treated after two sessions of CO2 laser therapy (spot size 2–3 mm, fluence 10–12 W, pulse duration 0•1 s) [5].
Treatment for xanthelasma palpebrarum, which shares features similar to the cutaneous manifestations of ECD, include surgi- cal resection, trichloroacetic acid, peeling, and laser therapy [6]. Because the morphological features of xanthelasmas are due to lipid laden histiocytes tightly adhering to the walls of small hy- perpermeable vessels, CO2 laser therapy in this setting works through thermal energy destroying perivascular foam cells and coagulate dermal vessels leading to the blockage of lipid leakage in tissue [7,8]. Surgery is limited given the amount of tissue ac- ceptable to resect before issues with ectropion occur.
Although we successfully treated the xanthelasma-like lesions in our ECD patients with fractional CO2 laser therapy, it should be noted that certain classes of medication used in the manage- ment of ECD may contribute to adverse effects in the setting of laser therapies. Prior to presenting to dermatology, our first patient was treated with IFN-α/PEG–IFN-α, which is often used for ECD in patients with high-burden disease without access to targeted therapies [9]. Interferon therapy can cause a reduction in white blood cell counts causing absolute neutrophil and lym- phocyte counts to decrease by 30% to 50% of baseline [10]. In the setting of laser therapy, this can increase the risk of infection [10]. In patients undergoing treatment with cobimetinib, a MEK inhibitor, it should be noted that the antiangiogenic and anti-EG- FR properties associated with this class of drugs could impair wound healing [9,11]. Vemurafenib, a drug that is often taken in combination with cobimetinib has a side effect of photosen- sitivity. Although the mechanism of drug-induced photosensi- tivity does not overlap with the wavelengths used by lasers in medicine, the photosensitivity in the setting of vemurafenib and importance of sun protection should be emphasized [9,12].
Conclusion
Collaborative efforts between dermatologists and oncologists should be considered when treating patients with persistent cutaneous manifestations of Erdheim-Chester disease. Clini- cians treating patients with cutaneous manifestations of Erd- heim-Chester disease can consider fractional CO2 laser therapy as a treatment option. However, when treating patients undergo- ing immunosuppressive and targeted therapies, it is important to be aware of the different adverse effects that can occur with treatments involving laser therapy.

Figure 1a: Multiple Periorbital and Perioral Xanthelasma-like Plaques.

Figure 1b: Significant Improvement of Periorbital and Perioral Xanthelasma-like Plaques.
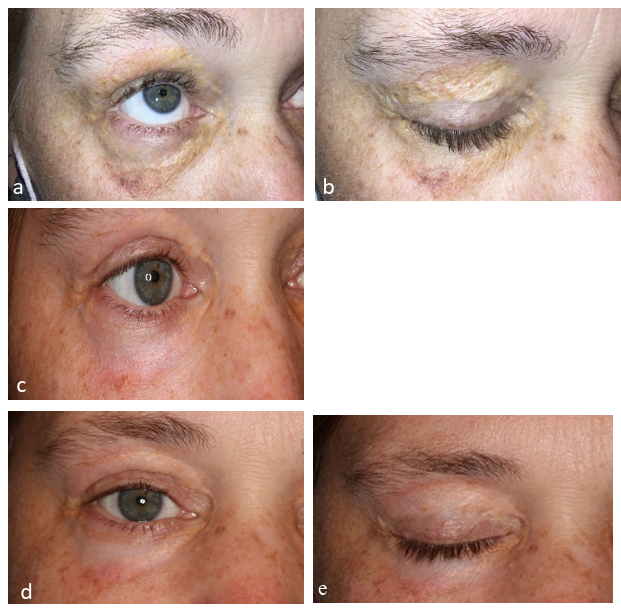
Figure 2a-b: Initial Presentation of Patient Two with Xanthelasma-Like Plaques, Right Eye Before Laser and Surgical Interventions in our Clinic.
Figure 2c: Patient two, three months after Laser Treatment to right eye (shown) with Concomitant Excision of Left Lower Eyelid (not shown).
Figure 2d-e: Patient two, four months after Laser Therapy to right eye (shown), with Concomitant Excision of Left Upper Eyelid.
Conflicts of Interest: The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Acknowledgement: This research was funded, in part, by NIH/ NCI Cancer Center Support Grant P30 CA008748 and NIH/NCI R37 CA259260-01 (ELD, the Frame Family Fund (ELD), Joy Family West Foundation (ELD), and Applebaum Foundation (ELD). The funders had no role in the design and conduct of the study: collection, management, analysis, and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication.
References
- Kobic, A., Shah, K. K., Schmitt, A. R., Goyal, G., Go, R. S., Guo, R., ... & Mayo Clinic Histiocytosis Working Group. (2020). Erdheim–Chester disease: expanding the spectrum of cutaneous manifestations. British Journal of Dermatolo- gy, 182(2), 405-409.
- Chasset, F., Barete, S., Charlotte, F., Cohen-Aubart, F., Ar- naud, L., Le Pelletier, F., ... & Haroche, J. (2016). Cutane- ous manifestations of Erdheim-Chester disease (ECD): clin- ical, pathological, and molecular features in a monocentric series of 40 patients. Journal of the American Academy of Dermatology, 74(3), 513-520.
- Haroche, J., Charlotte, F., Arnaud, L., Von Deimling, A., Hélias-Rodzewicz, Z., Hervier, B., ... & Emile, J. F. (2012). High prevalence of BRAF V600E mutations in Erd- heim-Chester disease but not in other non-Langerhans cell histiocytoses. Blood, The Journal of the American Society of Hematology, 120(13), 2700-2703.
- Volpicelli, E. R., Doyle, L., Annes, J. P., Murray, M. F., Jacobsen, E., Murphy, G. F., & Saavedra, A. P. (2011). Erdheim–Chester disease presenting with cutaneous in- volvement: a case report and literature review. Journal of cutaneous pathology, 38(3), 280-285.
- Elosua-González, M., López-Estebaranz, J. L., Pampín- Franco, A., García-Zamora, E., & Villalón-Blanco, L. (2018). Image Gallery: Cutaneous lesions of Erdheim– Chester disease treated with carbon dioxide laser therapy. British Journal of Dermatology, 179(6), e228-e228.
- Fusade, T. (2008). Treatment of xanthelasma palpebrarum by 1064-nm Q-switched Nd: YAG laser: a study of 11 cases. British journal of dermatology, 158(1), 84-87.
- Al-Kady, N. A. S., Hamdino, M., & Abdel Kawy, F. A. W. (2021). Fractional CO2 laser versus trichloroacetic acid 50% for xanthelasma palpebrarum therapy. Journal of cos- metic dermatology, 20(3), 763-768.
- Karsai, S., Czarnecka, A., & Raulin, C. (2010). Treatment of xanthelasma palpebrarum using a pulsed dye laser: a prospective clinical trial in 38 cases. Dermatologic surgery, 36(5), 610-617.
- Goyal, G., Heaney, M. L., Collin, M., Cohen-Aubart, F.,Vaglio, A., Durham, B. H., ... & Diamond, E. L. (2020). Erdheim-Chester disease: consensus recommendations for evaluation, diagnosis, and treatment in the molecular era. Blood, The Journal of the American Society of Hematology, 135(22), 1929-1945.
- Soza, A., Everhart, J. E., Ghany, M. G., Doo, E., Heller, T., Promrat, K., ... & Hoofnagle, J. H. (2002). Neutropenia during combination therapy of interferon alfa and ribavirin for chronic hepatitis C. Hepatology, 36(5), 1273-1279.
- Shah, D. R., Dholakia, S., & Shah, R. R. (2014). Effect of tyrosine kinase inhibitors on wound healing and tissue re- pair: implications for surgery in cancer patients. Drug safe- ty, 37, 135-149.
- Kerstein, R. L., Lister, T., & Cole, R. (2014). Laser therapy and photosensitive medication: a review of the evidence. Lasers in medical science, 29, 1449-1452.