
International Journal of Cancer Research & Therapy(IJCRT)
ISSN: 2476-2377 | DOI: 10.33140/IJCRT
Impact Factor: 1.3

Research Article - (2024) Volume 9, Issue 2
Introduction and Problems of Robot-Assisted Surgery for Colorectal Cancer During the Covid-19 Pandemic in Japan: A Single-Institution Experience
2Department of Gastroenterological Surgery, Nippon Medical School, Tokyo, Japan
3Department of Gastroenterological Surgery, Nippon Medical School Chibahokusoh Hospital, Chiba, Japan
Received Date: Sep 12, 2024 / Accepted Date: Oct 10, 2024 / Published Date: Oct 16, 2024
Copyright: ©Â©2024 Ryo Ohta, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Ohta, R., Yokoyama, Y., Takeda, K., Sekiguchi, K., Shimizu, T., et al. (2024). Introduction and Problems of Robot-Assisted Surgery for Colorectal Cancer During The Covid-19 Pandemic in Japan: A Single-Institution Experience. Int J Cancer Res Ther, 9(2), 01-07.
Abstract
Introduction The colorectal robot-assisted surgery acquired insurance coverage in 2018, and its demand has increased significantly in Japan. The introduction of robot-assisted surgery should follow guidelines led by the Japanese Society for Endoscopic Surgery (JSES). The requirements are wide-ranging, including acquisition of certification through training courses, visits to other facilities by the medical team, necessity of inviting proctors, and acquisition of facility conditions. However, introducing robot- assisted surgery in accordance with these guidelines is not easy during COVID-19 pandemic.
Methods We considered the current situation and problems in our department, which recently introduced robot-assisted colorectal surgery. Furthermore, we examined the problems associated with introduction of robot-assisted surgery in Japan.
Results In our department, there was no doctor with experience in robot-assisted surgery, so we started by obtaining the certificates of operator and assistant. Due to the impact of the COVID-19 pandemic, there was a reservation limit for the certificate acquisition program, which caused a delay in taking the course. In addition, it was difficult to observe the operation as a team due to the number of people at the receiving hospital and the COVID-19 infection of the operating room staff in our hospital. At proctor, events such as the outbreak of COVID-19 clusters at the workplace of the invited doctor caused the schedule to be canceled suddenly.
Conclusion In anticipation of future infectious disease outbreaks similar to the COVID-19 pandemic, it is important to establish a system that can easily and smoothly introduce robot-assisted surgery in Japan.
Keywords
Robotic Surgery, Colorectal Surgery, Covid-19 Pandemic, Japan
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has profoundly affected society and healthcare worldwide. This negative impact includes effects on surgeries, with reports from various countries clearly showing a decline in surgical operations during the COVID-19 pandemic [1]. Most elective surgeries have been cancelled, and the number of surgeries for malignancies has also decreased [2]. Moreover, medical workers have been affected; the increase in the number of patients with COVID-19 has resulted in a shortage of medical staff [3]. These changes are expected to have a significant impact on robot-assisted surgery.
Robot-assisted total prostatectomy has been covered by Japanese national insurance since 2012. In the field of colorectal surgery, robot-assisted surgery for rectal cancer has been covered by public health insurance since April 2018 [4]. As a result, this procedure has become widely introduced at many institutions in Japan. Most recently, robot-assisted surgery for colon cancer was approved for coverage by public health insurance in 2022; thus, a further increase in the number of robot-assisted colorectal surgeries is expected. However, the introduction of robot-assisted surgery in Japan is complicated because it requires adherence to the guidelines of the Japan Society of Endoscopic Surgery (JSES).
We herein discuss the difficulties associated with introducing robot-assisted surgery for rectal cancer in our department during the COVID-19 pandemic and the problems encountered during its introduction in Japan.
Materials and Methods
Trends in COVID-19 Status in Japan
In Japan, there was an obligation to report the number of people with positive COVID-19 tests to public health centers from 16 January 2020 to 8 May 2023. Japan then downgraded the legal classification of COVID-19 infection on 8 May 2023, placing it in the same category as common infectious diseases such as seasonal influenza as a measure to ease COVID-19 prevention regulations. Thus, the data for 7 May 2023 represent the final aggregate value [5]. In this analysis, the number of newly confirmed positive cases of COVID-19 was based on the data published by the Ministry of Health, Labour and Welfare submitted from each local government in Japan.
Nationwide Survey of Endoscopic Surgery in Japan
Since 1990, the JSES has conducted a national survey every 2 years to evaluate the status of endoscopic surgery in Japan [6-11]. The questionnaire survey is conducted at institutions that perform endoscopic surgery in Japan and contains items on the number of cases and surgical outcomes of endoscopic and robotic surgery. In the 16th nationwide survey, the questionnaire was sent to 3,940 institutions, and responses were received from 1,313 institutions or departments (response rate of 33.3%) [11]. Lower gastrointestinal surgery cases were extracted from the responses, and the trends in the number of laparoscopic and robot-assisted surgery cases were tabulated.
Introduction of Robot-Assisted Colorectal Surgery at our Hospital
Our hospital did not introduce robot-assisted surgery until we moved to a new hospital in September 2021. In June 2022, the da Vinci X surgical system (Intuitive Surgical, Sunnyvale, CA, USA) was introduced for robot-assisted surgery. The urology department of our hospital was the first to start performing robotic surgery, followed by our department of gastrointestinal and hepato-biliary-pancreatic surgery. During the COVID-19 pandemic, our department began performing robot-assisted surgery for rectal cancer in August 2022 and robot-assisted surgery for colon cancer in July 2023.
Results
Changes In Number of Endoscopic Surgeries in Japan During Covid-19 Pandemic
Figure 1 shows the trends in the number of endoscopic surgeries for colorectal cancer compiled from the 16th JSES questionnaire survey. The number of laparoscopic colorectal surgeries in Japan increased markedly over the years. However, the number of these surgeries clearly decreased starting in 2019, when the COVID-19 pandemic began. The cancellation of health checkups and avoidance of medical institutions because of the COVID-19 pandemic were thought to be the reasons for the decrease in these surgeries. By contrast, robot-assisted surgery for colorectal cancer remained unaffected and continued to increase steadily in Japan (Fig. 2).

Figure 1: Trends in the Number of Laparoscopic and Robot-Assisted Surgeries for Colorectal Cancer Compiled from the 16th JSES Questionnaire Survey
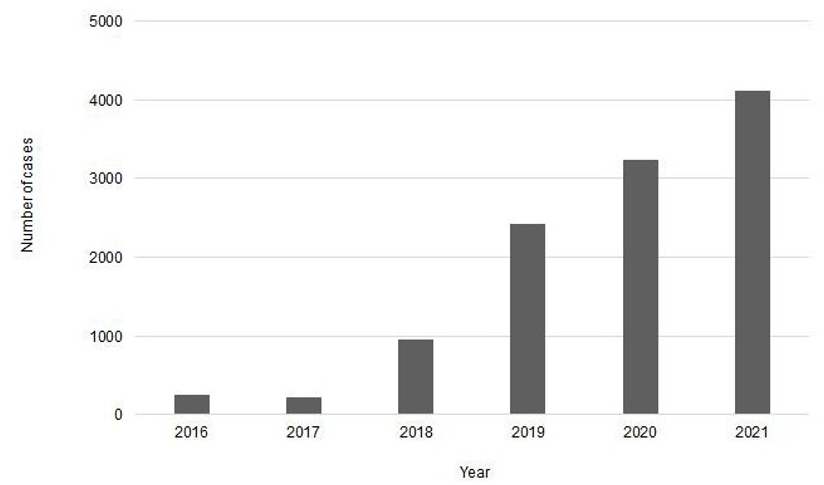
Figure 2: Trends in the Number of Robot-Assisted Surgeries for Colorectal Cancer Compiled from the 16th JSES Questionnaire Survey
Guidelines for Introduction of Robot-Assisted Surgery for Colorectal Cancer in Japan
The JSES has produced a publication titled ''Guidelines for the Introduction of Robot-Assisted Endoscopic Surgery'' to safely introduce and popularize robot-assisted surgery in Japan. The guidelines consist of cross-disciplinary guidelines and department- specific guidelines. The cross-disciplinary guidelines stipulate conditions for surgeons and facilities (Table 1). Regarding the conditions for surgeons, operators are required to take a training course set by the manufacturer and obtain certification for robotic-assisted surgery. Surgeons are also recommended to perform their first procedure within 30 days of obtaining the certificate. Regarding the conditions for facilities, the medical team (including the surgeon, assistant, and surgical nurse) must sufficiently observe robotic surgery at other facilities before starting to perform robotic surgery in their own facility. Additionally, a JSES-certified proctor must be invited for the first robotic surgery procedure, and the procedure must be performed under the proctor's guidance. Furthermore, each facility must create guidelines for introducing new surgical techniques to ensure safe introduction.
|
cross-disciplinary guidelines |
|
|
conditions for surgeons
conditions for facilities |
Attended a training course and obtained certification in robot-assisted endoscopic surgery It is recommended that the first case be performed within 30 days of obtaining the certificate
The medical team, including the surgeon, assitant, and surgical nurse, conducts sufficient case obsevation The first case should be conducted under the guidance of the JSES-certified proctor Participate in the registry system established by theJSES or related societies Create guidelines for introducing new surgical procedures at each facility and ensure safe introduction |
Table 1: Cross-Disciplinary Guidelines for the Introduction of Robot-Assisted Colorectal Surgery in Japan
In the department-specific guidelines, additional conditions are imposed in the field of gastrointestinal robotic surgery (Table 2). Console surgeons must have experience assisting in 10 cases of gastrointestinal robotic surgery before being able to introduce robotic surgery under the guidance of a JSES-certified proctor. However, if a console surgeon is a specialist certified by the Japanese Society of Gastroenterological Surgery, the above assistant experience is not required.
|
department-specific guidelines |
|
|
conditions for surgeons
conditions for facilities |
Console surgeons will have experience assisting in 10 cases of robot-assisted endoscopic surgery in the gastrointestinal surgery field. However, the above-mentioned assistant experienece is not required for gastrointestinal surgery specialists of the Japanese Society of Gastroenterological Surgey
Console surgeons must be fully proficient in general open and laparoscopic surgical techniques, perioperative management, and treatment of complications
When introducing robot-assisted endoscopic surgery, at least one case should observe the relevant procedure
In order to start robot-assisted endoscopic surgery as an independent team, the team must have someone who has JSES technical certification, at least one case of robot-assisted endoscopic surgery at another facility for the relevant procedure, and one case under the guidance of the JSES-certified proctor |
Table 2: Department-Specific Guidelines for the Introduction of Robot-Assisted Colorectal Surgery in Japan
Introduction of Robot-Assisted Surgery for Rectal Cancer in our Department and Status of Covid-19 in Japan
Figure 3 shows the introduction of robot-assisted surgery for rectal cancer in our department and the trends in COVID-19 in Japan. In accordance with the JSES guidelines for the introduction of robotic surgery, we first took a training course provided by the manufacturer and planned to obtain certification. However, the number of available reservations for the basic training required to obtain certification was reduced because of the COVID-19 pandemic, resulting in a delay in obtaining the certification. Furthermore, we observed robot-assisted surgery for rectal cancer at another facility as a case observation. Like the basic training reservation status, the number of facilities designated by the JSES to accept case observations was reduced because of the COVID-19 pandemic, making it difficult to make such reservations.

Figure 3: Status of Introduction of Robot-Assisted Surgery for Rectal Cancer in our Department and Trends in the Number of COVID-19 Infections in Japan
Although the original plan to introduce robot-assisted surgery for rectal cancer had been unexpectedly delayed, robotic support equipment was introduced to our hospital in June 2022. We were able to obtain certification in July 2022, and we performed the first case of robot-assisted surgery for rectal cancer within 30 days of obtaining certification. For case observation by the medical team, the number of participants was limited at the designated facility; therefore, several case observations were conducted with a small number of participants. Although we planned onsite training using robotic support equipment at our hospital, the training was postponed because the person in charge of instructing had developed COVID-19. After overcoming many obstacles, we managed to perform the first robot-assisted surgery for rectal cancer on time under the difficulties imposed by the COVID-19 pandemic. With the assistance of the proctor, we successfully performed the first robotic-assisted surgery for rectal cancer with no complications. Robot-assisted surgery for colon cancer became covered by public health insurance in April 2022, and the number of cases has since been significantly increasing nationwide in Japan. Accordingly, our department introduced robot-assisted surgery for colon cancer in July 2023. Because robotic-assisted rectal surgery had already been introduced, robotic-assisted colectomy was easy to implement, and the number of cases is steadily increasing.
Discussion
We experienced several challenges in our introduction of robot-assisted surgery for rectal cancer during the COVID-19 pandemic. From this experience, we identified three issues that should be improved upon for successful introduction of robot-assisted surgery in Japan: difficulties in obtaining certification in robot-assisted surgery, difficulties in conducting case observations at other facilities, and difficulties in inviting certified proctors from other facilities.
In Japan, surgeons receive a certificate after undergoing training courses provided by robotic equipment companies in accordance with the JSES guidelines. The training course to obtain the certificate of robot-assisted surgery requires the completion of online training, on-site training using an actual robot system, case observation of actual robot-assisted surgery at another facility, and basic training using actual robot equipment in animals. To obtain a certificate for Intuitive Surgical's da Vinci robot system, which is the most frequently used robot system worldwide, there is a waiting period of 3 to 6 months for reservations to undergo basic training using animals in Japan. During the height of the COVID-19 pandemic, reservation slots were reduced and the number of participants per training session was limited. To efficiently obtain certificates under these circumstances, the number of training facilities in Japan should be increased and a system that would allow certificates to be obtained overseas should be established.
COVID-19 spread not only to patients but also to healthcare workers [12]. To prevent further spread of infection, medical institutions placed restrictions on pharmaceutical companies and medical device manufacturers. As a result, tours of operating rooms at other facilities were restricted, and the number of facilities accepting case observations, which are mandatory before introducing robotic surgery, decreased. However, the COVID-19 pandemic has fostered the advancement of online medical consultations and conferences for the purpose of preventing infection [13]. To improve this situation, a different form of case observation should be constructed. For example, it is possible to introduce remote live surgical observation using recently developed imaging systems and simulated surgical observation using virtual reality [14]. In a comparative study of training methods for robotic surgery, virtual reality was found to be more effective than e-learning; therefore, the introduction of a virtual reality system should also be considered [15]. Moreover, such training methods have the advantage of reducing the time and costs associated with on-demand observation and viewing from a distance, along with improving infection control measures [16].
The JSES guidelines state that to introduce robot-assisted surgery as an independent team, the team must include a member with JSES technical certification, performance of at least one case of robot-assisted endoscopic surgery at another facility for the relevant procedure, and performance of one case under the guidance of a JSES-certified proctor. During the COVID-19 pandemic, however, it was difficult to invite the proctor because his movement to other medical institutions was restricted. No other proctors were available nearby, so a proctor located approximately 1,160 km away from our hospital was invited. Although the number of JSES-certified proctors is increasing, an optimal method for inviting and making reservations for proctors has not been established.
A system that can be easily adapted to facilities that newly introduce robotic surgery is needed. A remote surgery guideline was recently established in Japan. The purpose of this guideline is to set appropriate standards for leading physicians to utilize information and communication technology for providing support and guidance for surgeries performed at various medical institutions. This includes telementoring and telesurgical support, which may enable remote proctor guidance in robotic surgery.
Since COVID-19 was classified as a common infectious disease in Japan, various restrictions in the medical industry have been eased. As a result, the number of robot-assisted surgeries is expected to increase further. Additionally, new models of robots have been developed and are beginning to appear on the market. Although the process of obtaining a da Vinci system certificate is the same worldwide, the systems used to introduce robotic surgery differ between Japan and other countries [17]. Standards for introducing robotic surgery should be created according to the medical circumstances of each country, and a system for introducing robotic surgery through training in other countries should be devised.
Conclusion
In conclusion, it is expected that medical situations similar to COVID-19 will continue to arise in future with the spread of unknown infectious diseases. Even in such situations, it is necessary to create a system that allows for the simple and smooth introduction of robot-assisted surgery in Japan.
Acknowledgment
We thank Angela Morben, DVM, ELS, from Edanz (https:// jp.edanz.com/ac) for editing a draft of this manuscript. This work was supported by the Department of Gastroenterological Surgery, Nippon Medical School.
Author Contributions
All authors contributed to the study conception and design. Material preparation and data collection and analysis were performed by Ryo Ohta, Yasuyuki Yokoyama, Kohki Takeda, Kumiko Sekiguchi, Takao Shimizu, Keisuke Minamimura, Takeshi Yamada, Nobuhiko Taniai, and Hiroshi Yoshida. The first draft of the manuscript was written by Ryo Ohta, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Statements And Declarations
Not applicable.
Ethical Considerations
The Ethics Committee of the The Ethics Committee of Nippon Medical School waived the need for ethics approval and patient consent for the collection, analysis and publication of the retrospectively obtained and anonymised data for this non-interventional study.
Declaration Of Conflicts Of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding Statement
The authors received no financial support for the research, authorship, and publication of this article.
Data Availability
Data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- Mattingly, A. S., Rose, L., Eddington, H. S., Trickey, A. W., Cullen, M. R., Morris, A. M., & Wren, S. M. (2021). Trends in US surgical procedures and health care system response to policies curtailing elective surgical operations during the COVID-19 pandemic. JAMA Network Open, 4(12), e2138038-e2138038.
- Collaborative, G., & COVIDSurg Collaborative. (2021). SARS-CoV-2 vaccination modelling for safe surgery to save lives: data from an international prospective cohort study. The British journal of surgery, 108(9), 1056.
- Mascha, E. J., Schober, P., Schefold, J. C., Stueber, F., & Luedi,M. M. (2020). Staffing with disease-based epidemiologic indices may reduce shortage of intensive care unit staff during the COVID-19 pandemic. Anesthesia & Analgesia, 131(1), 24-30.
- Minamimura, K., Hara, K., Matsumoto, S., Yasuda, T., Arai, H., Kakinuma, D., ... & Yoshida, H. (2023). Current status of robotic gastrointestinal surgery. Journal of Nippon Medical School, 90(4), 308-315.
- Kitahara, K., Nishikawa, Y., Yokoyama, H., Kikuchi, Y., & Sakoi, M. (2023). An overview of the reclassification of COVID-19 of the Infectious Diseases Control Law in Japan. Global Health & Medicine, 5(2), 70-74.
- Ohta, R., Yokoyama, Y., Takeda, K., Sekiguchi, K., Shimizu,T., Minamimura, K., ... & Yoshida, H. (2024). Introduction and problems of robot-assisted surgery for colorectal cancer during the COVID-19 pandemic in Japan: a single-institution experience.
- Bandoh T, Shiraishi N, Yamashita Y, Terachi T, Hashizume M, et al. (2017) Endoscopic surgery in Japan: The 12th national survey(2012-2013) by the Japan Society for Endoscopic Surgery. Asian J Endosc Surg 10: 345-353.
- Shiroshita H, Inomata M, Bandoh T, Uchida H, Akira S, et al. (2019) Endoscopic surgery in Japan: The 13th national survey (2014-2015) by the Japan Society for Endoscopic Surgery. Asian J Endosc Surg 12: 7-18.
- Inomata M, Shiroshita H, Uchida H, Bandoh T, Akira S, et al. (2020) Current status of endoscopic surgery in Japan: The 14th National Survey of Endoscopic Surgery by the Japan Society for Endoscopic Surgery. Asian J Endosc Surg 13: 7-18.
- Shiroshita H, Inomata M, Akira S, Kanayama H, Yamaguchi S, et al. (2022) Current Status of Endoscopic Surgery in Japan: The 15th National Survey of Endoscopic Surgery by the Japan Society for Endoscopic Surgery. Asian J Endosc Surg 15: 415-426.
- Shiroshita H, Inomata M, Takiguchi S, Akira S, Kanayama H, et al. (2024) Update on endoscopic surgery in Japan: Results of the 16th National Survey of endoscopic surgery by the Japan Society for Endoscopic Surgery. Asian Journal of Endoscopic Surgery 17.
- Razzak JA, Bhatti JA, Tahir MR, Pasha-Razzak O (2020) Initial estimates of COVID-19 infections in hospital workers in the United States during the first wave of pandemic. PLoS One 15: e0242589.
- Chick RC, Clifton GT, Peace KM, Propper BW, Hale DF, et al. (2020) Using Technology to Maintain the Education of Residents During the COVID-19 Pandemic. J Surg Educ 77: 729-732.
- Din N, Chan CC, Cohen E, Iovieno A, Dahan A, et al. (2022) Remote Surgeon Virtual Presence: A Novel Telementoring Method for Live Surgical Training. Cornea 41: 385-389.
- Eley CL, Palaniappan V, Carter A, Sogaolu O, Horwood J, et al. (2024) Randomized controlled trial of the CMR immersive virtual reality (IVR) headset training compared to e-learning for operating room configuration of the CMR versius robot. J Robot Surg 18: 143.
- El-Sabawi B, Magee W, 3rd (2016) The evolution of surgical telementoring: current applications and future directions. Ann Transl Med 4: 391.
- Nacul MP, Melani AGF, Zilberstein B, Benevenuto DS, Cavazzola LT, et al. (2020) Educational note: teaching and training in robotic surgery. An opinion of the Minimally Invasive and Robotic Surgery Committee of the Brazilian College of Surgeons. Rev Col Bras Cir 47: e20202681.