


Case Report - (2019) Volume 4, Issue 3
Intravascular Papillary Endothelial Tumor of the Adrenal Gland: A Case Report and Review of Literature
2Division of Surgery, Assaf Harofeh Medical Center, Tzrifin, Israel
3Department of Pathology, Assaf Harofeh Medical Center, Tzrifin, Israel
Received Date: May 24, 2019 / Accepted Date: Jun 20, 2019 / Published Date: Jul 03, 2019
Copyright: ©Midhat Abu Sneineh, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Intravascular Papillary Endothelial Hyperplasia (IPEH) or Masson’s Tumor is a benign vascular tumor, most commonly seen on the skin and usually on the head, neck or extremities. It is more common in women with no age predilection. Visceral involvement is very rare, with about 30 intra-abdominal reports. We present a case report of a 58 year old woman who underwent a CT scan due to dysphagia complaints, with an incidental known finding of growth in the adrenal adenoma, which was 5 cm in diameter on hospitalization. The patient underwent laparoscopic adrenalectomy. Biopsy results demonstrated a brownish yellow lesion, 2.8 cm in diameter, composed of a blood clot and septate. Immunochemical staining for CD31 and CD34 was positive and the lesion was diagnosed as an IPEH of pure form. Our review of literature examines different forms of IPEH, previous reports and characteristics of Masson’s tumors in the adrenal gland and stratifies ways of differentiation it from other benign or malignant lesions of the adrenal.
Introduction
Intravascular Papillary Endothelial Hyperplasia (IPEH), also known as Masson’s Tumor, is a rare, benign, vascular tumor. It was first described in 1923 by Pierre Masson, as an intravascular papillary proliferation, formed within an inflamed hemorrhoidal plexus. He described it as a neoplasm- a proliferation of endothelial cells within a lumen, which is later followed by obstruction, secondary degeneration and necrosis [1]. Later on the lesion was defined as a hyperplasia rather than a neoplasm and was differentiated from similar proliferation of sarcomas, as being completely benign [2].
IPEH is most commonly seen in the skin of the head, neck and hands, representing 2% of all skin tumors [3]. The lesion is usually located in the deep dermal or subcutaneous tissue. Involvement of visceral organs with IPEH is rare. However, there are case reports of IPEH arising in various additional organs, including: liver, GI tract, renal sinus, as well as chest wall and lung [4-7]. The lesion could occur in both men and women, however although no explanations involving hormonal influence have been found, it is slightly more common in women (64%). The age range at which IPEH can be diagnosed is very broad; cases have been reported from the age of 7 months to 81 years, with the average age of 38.9 years [4].
The particular reactive process in IPEH consists of endothelial cells organizing and proliferating around an intravascular thrombus. Histologically IPEH appearance most resembles a granulation process. There are three forms of IPEH [4,8]:
a) Primary or pure form- the most common form (55.8%). It occurs in dilated blood vessels, more often veins than arteries, without a primary co-morbidity that could cause it’s arise.
b) Secondary or mixed form- composes 39.9% of IPEHs. This form of endothelial proliferation occurs around a pre-existing intravascular lesion, such as: arteriovenous malformations, pyogenic granulomatosis, venous thrombosis caused by different chronic illnesses but most commonly around haemangioma.
c) Extra-vascular form- The rarest form (4.3%). In this case, an extra-vascular pre-exciting hematoma, usually trauma- induced, serves as a template for the endothelial proliferation.
Surgical resection is considered curative if the resection in executed with clear margins or if the IPEH is of pure form. However, there is a 7-10% chance of recurrence in the mixed or extra-vascular forms [4,9].
The aim of this case report is to describe a highly uncommon presentation of Masson’s tumor, located in the adrenal gland. Using a search engine provided by Assaf Harofeh Medical Center to screen pub med, we searched for all reports of Masson’s tumor in the adrenal glands. The first description of IPEH was published in 1986 by Kawashima et al. [10], and only 7 additional cases have been describes since then [11-13].
Case Report
A 58 year old female with complaints of dysphagia and a suspected esophageal spasm was admitted to undergo a CT scan. Her medicalhistory was only significant for hypercholesterolemia and a previous asymptomatic radiological finding in her right adrenal gland, which was under periodic observation. Surgical history was unremarkable.
The current CT scan demonstrated a growth of the known adrenal adenoma, which was now measured to be 5 cm in diameter. The patient went through a full endocrine evaluation without any pathological findings. However, due to the estimated size of the adenoma, it was decided to perform a laparoscopic resection of the adrenal gland. The operation was performed under general anaesthesia and the detected mass was fully resected. Post-operative duration was normal without any complications.
Biopsy Results
A 45 gr. adrenal gland (5.5x4.3x1.3 cm) was harvested. Within the gland a brownish yellow lesion, soft and elastic, easily disseminated with a 2.8 diameter was observed. The lesion was composed of a blood clot and was septate. Immunochemical staining for CD31 and CD34 (markers of endothelial cells) were positive, while staining for CD40 was negative. Microscopic imaging detected short papillary structures laminated with a single layer of endothelial cells.
Pathology
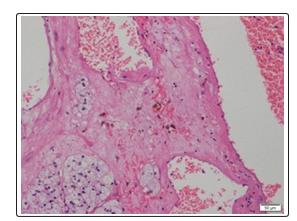
Figure 1: *40 H&E stain Blood filled space with fibrous stroma containing hemosiderin laden macrophages
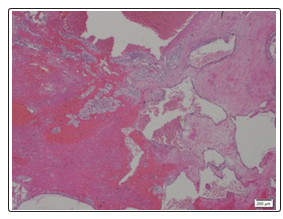
Figure 2B: *200 H&E blood filled spaces with papillary fronds proliferating into lumen
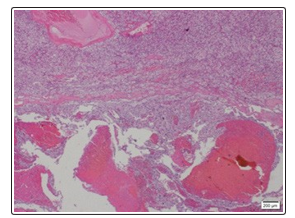
Figure 3: *100 H&E dilated blood filled spaces within vascular lumen
Discussion
IPEH was first described in 1923 as a neoplasm. However, 9 years later it was defined by Henschen to be more of a reactive causing proliferation process, rather than a neoplasm. It was not until 1976 when the definition of the tumour as an intravascular papillary endothelial hyperplasia gained wide acceptance [4].
Masson’s tumor is a benign tumor. It does not send metastases, nor does it infiltrate to the tissues in which it develops. It can, however, proliferate in the vascular lumen and rapture the vessel walls, similar to a malignant tumor, thus causing confusion with other clinical entities such as invasive angiosarcoma [11]. Other characteristics that help to differentiate Masson’s tumor from a malignant lesion are the absence of necrosis, cellular pleomorphism, and mitotic activity. Exceptionally, there may be minimal necrosis in cases where the lesion outgrows its blood supply [11,14].
Radiologic findings for IPEH are limited and mostly non-specific. Computed tomography, magnetic resonance imaging, and angiographic patterns of IPEH can mimic other benign and malignant processes, such as: pyogenic granuloma, Kaposi’s sarcoma, haemangioma, bacillary angiomatosis, and popular angiodysplasia [4]. Utilizing sonography imaging, IPEH usually appears uniform in echogenicity. Doppler sonography is helpful since demonstrating blood flow can confirm the intravascular location of the mass [15]. The resected lesion in our case was composed of papillary structures, laminated with a single layer of endothelial cells. Microscopic features of IPEH vary. It may consist of numerous papillae with a core of connective tissue and an endothelial surface. The lesion is usually well defined by a fibrous pseudo-capsule which contains smooth muscle tissue derived from the blood vessel wall. In rare cases of IPEH, a compromised pseudo-capsule could be detected in the extra-vascular space [11]. This encapsulation serves as a very important differentiating factor from the common angiosarcoma. Blood clots could be noticed within the lesion. The lesion may or may not exhibit small calcifications [16].
In the current case, a positive staining of CD31 and CD34 was observed. Those antigens are widely expressed on the cell surface of endothelial cells. Therefore utilizing immune-histochemical staining in order to characterize IPEH is most common. However, CD34 is also expressed on human hematopoietic cells and is thought to modulate adhesion in these cells, while CD31 is a glycoprotein expressed also by platelets, monocytes, granulocytes, B-cells, leukocytes, and endothelial cells [14].
It has been suggested that Factor VIII-related antigen (FVIII), which is synthesized by endothelial cells serving as an accurate marker for their differentiation and is not expressed in spindle shaped tumor cells of endothelial origin, could be used as a strong evidence of IPEH. However, FVII it can only be detected in mature lesions [14]. Other antigens which were identified by immune-histochemical staining in IPEH are Vimentin which has been reported to be positive in the stroma of Masson’s tumors, and the proliferation marker Ki-67 which was found to be weakly expressed)≤10%)) never over 10% [14-17].
Demographically, IPAH was found to be slightly more common in women and prevalent in patients of a wide age range. A review of literature published by Constantinou et al. (2008) examined specific characteristics of all reported cases of IPEH in the adrenal gland [8]. According to their review, the mean age of patients with adrenal IPEH was 64 years, most of them women. Average lesion size was 5.75 cm. Primary form of the lesion was reported in 5 of the 8 published cases, one was a rare extra vascular form, while none were of secondary form. Recurrence rates in various skin cases have been documented in a range of 7-10% and can appear for the mixed and extra vascular varieties [4].
Being a benign hyperplasia, these tumors are mostly asymptomatic. However, since they are located within blood vessels and can proliferate to create substantial mass, they can cause bleeding or obstruction. Among reported symptomatic Masson’s tumors are cases of IPEH in the urinary system which caused macroscopic hematuria and intermittent abdominal pain [18], IPEH located in the ligament of Treitz which caused GI bleeding and anemia [4], IPEH in the superior vena cava (SVC) which caused SVC syndrome an [19,20], a lesion on the vocal cord which caused hoarseness [17] and IPEH in the adrenal gland which was reported to cause back pain and gross hematuria [8].
Another finding reported in 60% of the patients is weight loss that is attributed to intermittent pain, mechanical obstruction of the GI tract or pharyngeal tumors, malabsorbtion in GI tumors and production of endothelial factors promoting satiety [5].
Conclusion
IPEH is a rare vascular proliferative process that usually involves the head, neck and extremities, while visceral involvement is very rare. Adrenal IPEH is an entity described in 8 previous case studies. Our report of adrenal IPEH shares the common characteristics described in these previous reports: our patient was a woman, 58years of age, with a 5 cm lesion as was demonstrated in a CT scan. After total excision of the adrenal gland the pathology report showed that the lesion was in fact an IPEH of pure form, and immunochemical staining for CD31 and CD34 was positive.
Our review of literature demonstrates the similarity of Masson’s tumor to both benign and malignant tumors, specifically angiosarcoma, and presents several differentiating factors, whether immune-histochemical, radiologic or histologic.
References
- Mahapatra QS, Sahai K, Malik A, Mani NS (2015) Intravascular papillary endothelial hyperplasia: An unusual histopathological entity. Indian Dermatol Online J 6: 277-279.
- Narwal A, Sen R, Singh V, Gupta A (2013) Masson’s hemangioma: A rare intraoral presentation. ContempClin Dent 4: 397-401.
- Joaquin Amérigo, Colin L Berry (1980) Intravascular papillary endothelial hyperplasia in the skin and subcutaneous tissue. Virchows Arch. A Path.Anat.And Histol 387: 81-90.
- Meadows MC, Sun X, Dardik M, Tarantino DR, Chamberlain RS (2010) Intra abdominal intravascular papillary endothelial hyperplasia (Masson’s tumor): A rare and novel cause of gastrointestinal bleeding.Case Rep Gastroenterol 4: 124-132.
- Johraku A, Miyanaga N, Sekido N, Ikeda H, Michishita N (1997) A case of intravascular papillary endothelial hyperplasia (Masson’s tumor) arising from renal sinus. Jpn J Clin Oncol 27: 433-436.
- Choi YD, Kim Y, Kim SS, Kim JH, Nam JH, et al. (2013) Intravascular papillary endothelial hyperplasia of the chest wall misdiagnosed as a malignancy on fine needle aspiration. Korean J Pathol 47: 499-501.
- Yanagawa N, Shiono S, Abiko M, Katahira M, Ogata SY, et al. (2014) Intravascular papillary endothelial hyperplasia of the lung. Kyobu Geka 67: 533-535.
- Constantinou C, Sheldon D (2008) Papillary endothelial hyperplasia of the adrenal gland: report of a case and review of the literature. Am Surg 74: 813-816
- Avellino AM, Grant GA, Harris AB, Wallace SK, Shaw CM (1999) Recurrent intracranial Masson’s vegetant intravascular hemangioendothelioma. J Neurosurg 91: 308-312.
- Kawashima A, Johsen T, Murayama S, Russell WJ (1986) Intravascular papillary endothelial hyperplasia of the adrenal gland.Br J Radiol 59: 610-613.
- Nassif AE, Pozzobon HJ, Azevedo EZ, Taguchi WS, Gomes RX (2009) Papillary endothelial hyperplasia of adrenal: case report. Rev Col Bras Cir 36: 277-278.
- Gaffey MJ, Mills SE, Fechner RE, Bertholf MF, Allen MS Jr (1989) Vascular adrenal cysts. A clinicopathologic and immunohistochemical study of endothelial and hemorrhagic (pseudocystic) variants.Am J SurgPathol 13: 740-747.
- Jennings TA, Ng B, Boguniewicz A, Khan M, Rice D, et al. (1998) Adrenal Pseudocysts: Evidence of their posthemorrhagicnature. EndocrPathol 9: 353-361.
- Akdur NC, Donmez M, Gozel S, Ustun H, Hucumenoglu S (2013) Intravascular papillary endothelial hyperplasia: histomorphological and immunohistochemical features. Diagn Pathol 8: 167.
- Schwartz SA, Taljanovic MS, Harrigal CL, Graham AR, Smyth SH (2008) Intravascular papillary endothelial hyperplasia: sonographic appearance with histopathologic correlation. J Ultrasound Med 27: 1651-1653.
- Mahapatra QS, Sahai K, Malik A, Mani NS (2015) Intravascular papillary endothelial hyperplasia: An unusual histopathological entity. Indian Dermatol Online J 6: 277-927.
- Tedla M, Bežová M, Biró C, Tedlová E, Eng CY, et al. (2014) Intravascular papillary endothelial hyperplasia of larynx: case report and literature review of all head and neck cases. Otolaryngol Pol 68: 200-203.
- Garber BB, Prestipino AJ, Pollack HM, Levine SR, Whitmore KE (1990) Masson’s tumor of the kidney: a new renal lesion. J Urol 143: 344-346.
- Park JY, Chung-Park M, Snow M (1991) Intravascular papillary endothelial hyperplasiaof superior vena cava: a rare cause of the superior vena cava syndrome. Thorax 46: 272-273.
- O, Adeoye A, Akang E (2012) Orbital intravascular papillary endothelial hyperplasia in a Nigerian child: A case report and review of the literature. J Med Case Rep 6: 300