
Research Article - (2022) Volume 7, Issue 1
Influence of Infant and Young Child Feeding Practices on Stunting in Children aged 6-23 months in Zambia
2University of Zambia, Department of Population Studies, Lusaka, Zambia
3Mulungushi University, Department of Economics, Kabwe, Zambia
4Peking University, Institute of Population Research, Beijing, China
Received Date: Dec 27, 2021 / Accepted Date: Feb 14, 2022 / Published Date: Feb 20, 2022
Copyright: ©Nkuye Moyo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Andrew Banda., Elizabeth T. Nyirenda., Chabila C., Mapoma, Bwalya B. Bwalya., Nkuye Moyo. (2022). Influence of Infant and Young Child Feeding Practices on Stunting in Children aged 6-23 months in Zambia. Adv Nutr Food Sci, 7(1), 117-127.
Abstract
Background: Infant and child nutrition in Zambia remains a pressing public health problem. The Zambia Demographic and Health Survey (ZDHS) indicates that 35% of children under-five and 36 % among those aged 6-23 months are stunted. This study set out to assess the influence of Infant and Child Feeding (IYCF) practices on child stunting (6-23 months) in Zambia.
Methods: The 2008 ZDHS children’s data were analysed to measure stunting among infants aged 6-23 months. We fitted a bivariate logistic regression to measure association between feeding practices and stunting in children. Pearson’s Chisquare test of proportions and adjusted odd ratios (AOR) with confidence intervals at 95% are reported.
Results: Findings indicate that 36% of children 6-23 months old were stunted. IYCF practices indicators remain relatively poor in Zambia with only 13% of children age 6-23 months having received minimum acceptable diet, 23% received minimum dietary diversity and 42% received minimum meal frequency. Breastfeeding and receipt of a minimum dietary diversity reduced the odds of stunting among children age 6-23 months by 38% and 33% respectively. A child’s perceived low birth size, being male, maternal anaemia status and mother’s use of the internet were significant predictors of stunting.
Conclusion: The study shows that IYCF practices have an influence on stunting in Zambia and that socio-economic and demographic factors are likewise associated with stunting although the main determinants are amendable to intervention. Promoting the recommended WHO IYCF practices; breastfeeding, minimum meal frequency, receiving foods with diverse dietary content and accelerated investment in nutrition programs is recommended.
Keywords
Stunting, Infant and Young Child Feeding, Nutritional Assessment
Introduction
Childhood stunting is one of the significant public health challeng-es and impediments to child development in Zambia and the world over, and reflects the country’s poor social and economic devel-opment[1]. Globally, 144 million children representing 21.3% are stunted or they are too short for their age [2]. Thirty-nine per cent of the worlds stunted children are in Africa[3]. According to the Africa Development Bank President Ainwumi Adesina “Africa is the only continent where the number of stunted children has in-creased over the last two decades: 58.5 million in 2018, up from 50.3 million at the turn of the century” [3]. In Zambia, 35% of children under five are stunted with Northern and Luapula Prov-inces having the highest prevalence – 36% and 45% respectively. Over the last two decades, childhood stunting has shown a posi¬tive downward trend from 53% in 2001-02 to 35 % in 2018 [4]. Despite the considerable decline, the levels of stunting in Zambia remain among the highest in the region and is barely 5 percentage points below the World Health Assembly resolution 65.6 aimed at reducing to below 40% the number of children under-5 who are stunted [1].
Stunting is defined as a height that is less than two standard de¬viations below the World Health Organization (WHO) Child Growth Standards [5]. It is generally a manifestation of chronic undernutrition which predisposes children to physical and cogni¬tive underdevelopment as well as exposes them to a greater risk of morbidity and mortality from common preventable infections as well as worsening the severity and chance of recovery from such infections. Whereas poor child health undermines societal devel-opment, improved health is the first step toward enabling children to break out of a cycle of ill health and poverty that may other¬wise continue for generations [6]. Literature suggests that mater¬nal, child-related factors and low socio-economic and households characteristics of mothers [7] as well as the prevalence of anaemia among mothers are associated with childhood stunting. In Zambia, it is unclear what drives the high prevalence of stunted children de¬spite considerable investment in Infant and Young Child Feeding (IYCF) practices policies, programmes and nutrition interventions [8].
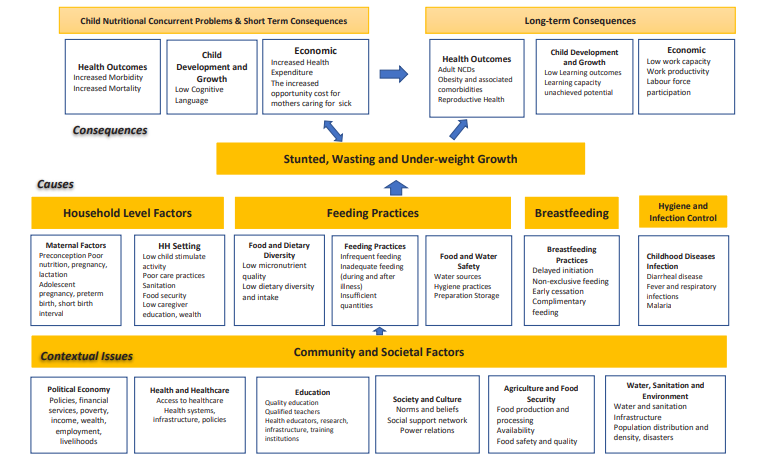
Feeding practices remain an important part of reducing childhood stunting. Thus, what, when and how children are fed particularly in the first two years of life is critical to their health, development and survival [9]. WHO recommends exclusive breastfeeding for the first 6 months of life because of its protective effect on the child from infections, malnutrition and obesity in later life [10, 11]. In Zambia, breastfeeding is very common with the majority of children 98% breastfed and 70% of children under six months exclusively breastfed. In addition to breastfeeding, vitamin A and iron supplementation are important to a child’s life. The 2018 ZDHS shows that 79% of children 6-23 months ate foods rich in vitamin A and about a three quarter (73%) of children 6-59 months received vitamin A supplements six months before the survey [4]. The WHO framework for childhood stunting (see appendix A) highlights four broad factors of stunting namely; household characteristics, inadequate complementary feeding, inadequate practice of breastfeeding and presence of childhood clinical and subclinical infections (diarrhoea and fever ) [12, 13].
Proper infant and young child feeding practices are central to prevent irreversible consequences of nutritional problems among children [14]. At least 200 million children living in developing countries fail to meet their developmental potential[3]. Along with undernutrition, related influences of infectious disease, environ¬mental hazards, and societal and household violence, all contribute to this loss of potential. Unlike many other influences that are im¬mutable or tremendously difficult to change, nutrition is something that can be controlled[15]. It is therefore important to prevent un-dernutrition during the critical 1000 days of life from conception up to two years of a child’s life by ensuring robust IYCF practices based on the 8 core indicators of early initiation of breastfeeding; exclusive breastfeeding for six months; continued breastfeeding at one year; introduction of solid, semi-solid or soft foods; minimum dietary diversity; minimum meal frequency; minimum acceptable diet; and consumption of iron-rich or iron-fortified foods [16]. This study, therefore, sought to examine the association between stunting (Nutritional status) and IYCF practices in Zambia. Con¬ceptual Framework
To examine the effect of IYCF practices on stunting, the study adapted an extract of the WHO conceptual framework of child¬hood stunting [12]. The key independent variables were based on the five IYCF indicators; currently breastfeeding, minimum dietary diversity, minimum meal frequency, minimum acceptable diet, and consumption of iron-rich foods controlled for other covariates such child, maternal and household characteristics (figure 1).
<img src="https://www.opastpublishers.com/scholarly-images/730-69ef43b0df8c3-influence-of-infant-and-young-child-feeding-practices-on-stu.png" width="500" height="300">
Figure 1: Conceptual Framework of child stunting (6-23 months) and IYCF Practices by Child, Maternal and Household Characteristics (Adapted from the WHO Childhood)
Methods
This study was based on a cross-sectional nationally representa-tive Survey (ZDHS 2018) to provide reliable estimates on the core health and demographic indicators at provincial and rural-urban level. The ZDHS captured a total of 10,094 children under-5. A sample was drawn from 9,606 children under-5 with valid mea-surement of height-for-age. To determine the effect of IYCF on stunting, the study used data for 2730 children age 6-23 months whose information on feeding practices was collected through in-terviews with their mothers in the ZDHS survey Variables.
Dependent Variable
The dependent variable, stunting (height-for-age) was categorised as 1 if the child had -2 SD and 0 if otherwise based on the WHO Child Growth Standards reference population (WHO, 2006). Stunting was computed from valid height-for-age Z-score. Chil-dren whose height-for-age Z-score was below minus two standard deviation (-2SD) from the median reference point were considered to be too short for their age (stunted) (WHO, 2009) and coded as 1 (1=stunted) and if otherwise not stunted and coded 0 (0= Not Stunted).
Independent Variables
The key independent variables were the five IYCF practices indi-cators: currently being breastfed, minimum dietary diversity, min-imum meal frequency, minimum acceptable diet, and consumption of iron-rich foods. These were defined into dummy binary vari¬ables, were 1 if the child was currently breastfeeding, received minimum dietary diversity, was fed at minimum meal frequency, received a minimum acceptable diet and received iron-rich foods and 0 if otherwise (e.g. 1= Yes, currently breastfeeding and 0= Not currently breastfeeding).
1. Minimum dietary diversity refers to the proportion of chil-dren age 6–23 months who received a minimum of 5 out of 8 food groups during the previous day. These include; i. breast milk; ii. infant formula, milk other than breast milk, cheese or yoghurt or other milk products; iii. foods made from grains, roots, and tubers, including porridge and fortified baby food from grains; iv. vitamin A-rich fruits and vegetables; v. other fruits and vegetables; vi. eggs; g. meat, poultry, fish, and shell¬fish (and organ meats); vii. legumes and nuts.
2. Minimum meal frequency denotes the proportion of children age 6-23 months who received solid, semi-solid, or soft food (including milk feeds for non-breastfed children) the mini-mum number of times or more during the previous day. The minimum is defined as two times for breastfed infants age 6-8 months, three times for breastfed children age 9-23 months, or four times for non-breastfed children age 6-23 months. “Meals” include both standard meals and snacks (other than trivial amounts), and frequency was based on caregiver report.
3. Minimum acceptable diet was measured based on the propor¬tion of children age 6–23 months who received a minimum acceptable diet. This indicator is a composite of children who met minimum dietary diversity and minimum meal frequency.
4. Consumption of iron-rich foods is defined as the proportion of children age 6-23 months who receive iron-rich food, which includes meat (and organ meat), fish, poultry, and eggs
5. Currently breastfed is defined as children age 6-23 months still being breastfed.
6. Covariates included were based on child’s characteristics such as: age, sex, perceived size of the child at birth and whether a child had received vitamin A recently as well as the presence of common child illness two weeks prior to the survey (diar¬rhoea and fever). Other covariates were maternal that included mother’s age, education level, employment status, number of antenatal visits, the birth interval between births and whether a mother had anaemia (below 11g/dl) and Household charac¬teristics included residence, wealth index and household wa¬ter and sanitation factors (source of drinking water, type of toilet facilities and disposal of child’s stool).
Statistical analysis
The study analysis was performed in two steps. The first step in¬volved descriptive and bivariate analysis to generate the average percentages of children with stunting by IYCF practices and child, maternal and household characteristics. The second step involved Survey-weighted logistic regression modelling was used to mea¬sure the effect of independent variables on the dependent variable stunting among children 6-23 months, adjusted odds ratios (AOR) and 95% confidence were used. Only significant variables from the bivariate analysis using the Pearson’s chi-square test (P<0.05) (5%) were added in the model. Some variables at p<0.1 (10%) lev¬el were permitted into the model, this was done to retain as many determinants as possible. All analyses were conducted using Stata version 14 and are based on weighted data.
Results
Child Stunting and Infant and Young Child Feeding Practices in Zambia
The 2018 Zambia Demographic and Health Survey shows that out of the 9609 children under five (0-59 months) with valid measure¬ment for height and age, 35% were stunted. Of the 2730 children ages 6-23 months, 2694 had valid measurement for height and age and of those, 36% were stunted (Table 1).
Table 1: Summary of Child Nutritional Status (Stunting) among children 0-59 and 6-23 months, 2018 ZDHS
|
|
Stunting (Height-for-Age) (0-59 months) |
Stunting (Height-for-Age) (6-23 months) |
|
Total children age 6-23 months |
|
2730 |
|
Number and % of children with valid measurements |
9,609 (95%) |
2694 (27%) |
|
Number children Stunted |
3322 |
959 |
|
Per cent of children Stunted |
34.6% |
35.6% |
Zambia’s childhood stunting levels have declined over the succes-sive demographic health surveys (between 2001/2 and 2018). The highest stunting levels were reported in 2001/02 with one in every two children under five (53 %) being stunted (Figure 2). A similar depiction is observed for underweight and wasting levels over the same period.
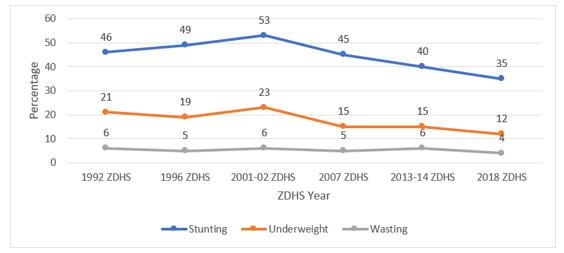
Figure 2: Trends in Nutritional Status of Children under five based on 2006 WHO Child Growth Standards
Minimum dietary Diversity, Minimum meal Frequency and Min-imum Acceptable diet and Stunting among children 6-23 months. Figure 3 shows the prevalence of IYCF practices among children 6-23 months in Zambia over the successive demographic and health surveys. The results show that 11% and 13% of children were fed on a minimum acceptable diet in the 24 hours preceding the interview in 2013/14 and 2018 respectively. Four in 10 chil-dren in both surveys (2013/14 and 2018) were fed the minimum meal frequency appropriate for their age. A similar pattern is ob-served for children who received an adequate diverse diet, (22 % in 2013/14 and 23% in 2018). Overall, the results appear to show minimal improvement in absolute terms in the three IYCF practic-es indicators between the two successive surveys.
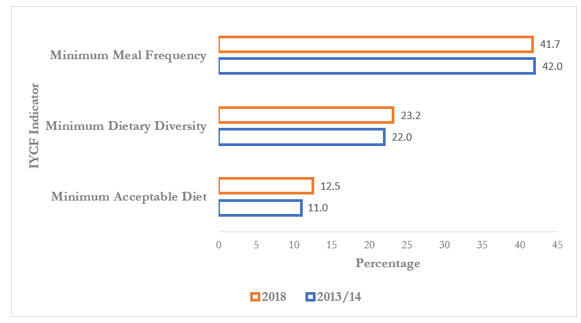
Figure 3: Prevalence of infant and Young Child Feeding Practices (IYCF) among children ages 6-23 months, ZDHS 2013/14 and 2018
Figure 4 demonstrates that about three in 10 children ages 6-23 months were stunted across the three IYCF practices indicators, however, stunting was generally more prevalent among children who were not fed on iron-rich foods, did not receive diverse di¬etary meals, did not receive an acceptable diet and were not fed frequently. Similarly, more children were stunted among those who were not currently breastfed (see table 2).
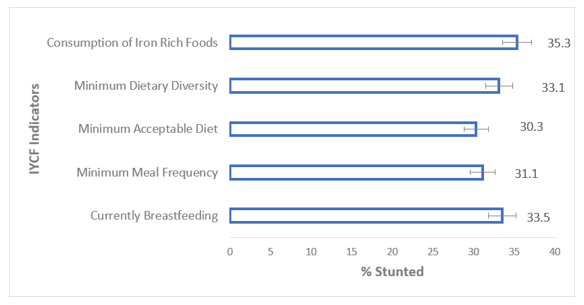
Figure 4: Prevalence of IYCF Practices and Stunting among Children age 6-23 months
Child Stunting by Infant and Young Child Feeding (IYCF) Practic¬es and Child, Maternal, and Household Characteristics.
Table 2 shows bivariate analysis of stunting among children ages 6-23 months and other covariates; IYCF practices, child, maternal and household characteristics. The results confirm that child stunt¬ing was significantly associated with sex of the child, child’s age, perceived size of child at birth, receipt of vitamin A supplement and child’s anaemia status. On the Maternal characteristics side, maternal education, women’s access to the internet, the number of antenatal visits attended and household wealth status are signifi¬cantly associated with child stunting (p<0.01).
Child and Maternal Characteristics on Stunting among children age 6-23 months
The sex and age of the child are important attributes in child nu¬tritional assessment. Table 2 indicates that both the sex and age of the child are significantly associated with stunting (p<0.01). The prevalence of stunting appears to increase with increasing age of the child with the highest prevalence among children age 18-23 months (46%) compared with 23% among children age 6-8 months. Childs perceived size at birth is significantly associated with child stunting.
Children with a perceived below average size at birth had a higher prevalence of stunting (47%) compared to those with a perceived above average size at birth. Similarly, maternal edu-cation, women’s access to the internet, the number of antenatal visits attended, household wealth status is significantly (p<0.01) associated with child stunting. Stunting among children age 6-23 months appears to decrease with increasing mother’s level of ed-ucation. Household Characteristics on Stunting among Children age 6-23 months.
Zambia’s stunting prevalence among children ages 6-23 months appears to vary significantly by region and residence. The high¬est prevalence is reported in Luapula (47%) and Northern (43%) provinces. Rural areas have a higher prevalence of child stunting compared to urban areas (38% versus 33%; p<0.01). Children from poorer households appear to have a higher prevalence of stunting at 45% compared with 25% among those from richer households (p<0.01).
Table 2: Prevalence of stunting among children age 6-23 months by child, maternal, Household and IYCF characteristics(n=2730)
|
Characteristic |
% |
CI |
P-Value |
|
Child’s Characteristics |
|||
|
Sex of the Child |
|||
|
Female |
29.2 |
[26.5, 32.1] |
|
|
Male |
43.1 |
[39.9, 46.3] |
<0.001 |
|
Age of Child (Months) |
|||
|
6-8 Months |
22.7 |
[18.6, 27.5] |
|
|
9-11 Months |
27.4 |
[22.2, 32.7] |
<0.001 |
|
12-17 Months |
37.0 |
[33.2, 41.1] |
|
|
18-23 Months |
46.4 |
[42.8, 49.9] |
|
|
Perceived Size of Child at Birth |
|||
|
Average and Above |
34.5 |
[32.2, 36.8] |
|
|
Below Average |
46.8 |
[42.1, 52.7] |
<0.001 |
|
Birth Order |
|||
|
1st Child |
36.2 |
[31.8, 40.9] |
|
|
2nd Child |
38.5 |
[33.5, 43.7] |
|
|
3rd Child |
32.6 |
[27.5, 38.1] |
0.466 |
|
4th and Above |
36.3 |
[33.2, 39.4] |
|
|
Vitamin A in the last 6 months |
|||
|
Not Received/Not Known |
30.2 |
[26.2, 34.6] |
|
|
Received |
37.9 |
[35.4, 40.4] |
0.003 |
|
Child Anemia (<11g/dl) |
|||
|
No |
30.4 |
[26.2, 34.8] |
|
|
Yes |
38.3 |
[35.7, 40.6] |
0.003 |
|
Diarrhoea in the last 2 weeks |
|||
|
No |
37.0 |
[34.5, 39.6] |
|
|
Yes |
33.9 |
[30.3, 37.6] |
0.154 |
|
Maternal Characteristics |
|||
|
Age of Mother |
|||
|
Under 20 |
39.4 |
[33.7, 45.4] |
|
|
20-29 |
35.9 |
[32.9, 39.2] |
|
|
30-39 |
35.1 |
[30.9, 39.4] |
0.702 |
|
40-49 |
36.0 |
[28.4, 44.4] |
|
|
Mother’s Level of Education |
|||
|
No Education |
41.2 |
[34.8, 47.9] |
|
|
Primary |
38.6 |
[36.0, 41.3] |
<0.001 |
|
Secondary |
34.0 |
[30.4, 37.9] |
|
|
Higher |
10.9 |
[5.8, 19.7] |
|
|
Mother’s Employment Status |
|||
|
Not Working |
36.5 |
[33.6, 39.6] |
|
|
Working |
35.7 |
[32.7, 38.7] |
0.685 |
|
Number of ANC Visits |
|||
|
None |
35.6 |
[20.4. 54.3] |
|
|
1-3 |
36.6 |
[32.8, 40.6] |
0.003 |
|
4+ |
34.9 |
[45.2, 65.6] |
|
|
Maternal Anaemia (<11g/dl) |
|||
|
Yes |
34.5 |
[31.9, 37.1] |
|
|
No |
41.2 |
[36.8, 53.1] |
0.020 |
|
Birth Interval Group |
|
|
|
|
>= 24 Months |
39.4 |
[31.5, 47.9] |
|
|
<24 Months |
35.3 |
[32.2, 41.3] |
0.581 |
|
Household Characteristics |
|||
|
Wealth Index |
|||
|
Poor |
39.6 |
[36.9, 42.4] |
|
|
Middle |
36.5 |
[32.9, 40.2] |
<0.001 |
|
Rich |
24.5 |
[19.3, 30.7] |
|
|
Residence |
|||
|
Rural |
37.9 |
[35.6, 40.3] |
|
|
Urban |
32.7 |
[28.6. 37.1] |
0.039 |
|
Region |
|||
|
Central |
41.5 |
[35.4, 47.9] |
|
|
Copperbelt |
34.2 |
[26.4, 43.0] |
|
|
Eastern |
35.4 |
[30.5, 40.8] |
|
|
Luapula |
47.2 |
[41.6, 52.9] |
|
|
Lusaka |
32.3 |
[26.1, 39.2] |
0.003 |
|
Muchinga |
25.9 |
[19.8, 33.3] |
|
|
Northern |
43.4 |
[37.3, 49.6] |
|
|
North Western |
32.9 |
[26.3, 40.3] |
|
|
Southern |
34.7 |
[29.3, 40.6] |
|
|
Western |
32.1 |
[26.2, 38.7] |
|
|
Use of the Internet |
|||
|
Never Used or more than 12 months |
37.6 |
[35.5, 39.8] |
|
|
Yes, Last 12 Months |
18.3 |
[12.3. 26.2] |
<0.001 |
|
Infant Young Children Feeding (IYCF) Practices |
|||
|
Minimum Meal Frequency |
|
|
|
|
No |
35.9 |
[32.7, 39.2] |
|
|
Yes |
31.1 |
[27.8, 34.6] |
<0.001 |
|
Minimum Acceptable Diet |
|||
|
No |
36.9 |
[34.8, 39.1] |
|
|
Yes |
30.3 |
[24.2, 37.1] |
0.058 |
|
Minimum Dietary Diversity |
|||
|
No |
37.3 |
[34.9, 39.7] |
|
|
Yes |
33.1 |
[28.7, 37.8] |
0.110 |
|
Consumption of Iron-Rich Foods |
|||
|
No |
37.0 |
[34.1, 40.1] |
|
|
Yes |
35.3 |
[32.3, 38.5] |
0.449 |
Infant and Young Child Feeding (IYCF) Practices on Stunting among Children age 6-23 Months.
To measure the magnitude of association between IYCF and stunt¬ing of children age 6-23 months, we ran an adjusted multiple re¬gression logistic model. Table 3 shows the results of the adjusted multiple regression model of stunting among children age 6-23 months. The odds of stunting among currently breastfed children age 6-23 months were 38% lower than for children who were not breastfed (AOR 0.62; 95% CI 0.48, 0.79). Among children who received a minimum dietary diversity, the odds of stunting were 33% lower than children age 6-23 who did not receive a minimum dietary diversity 24 hours prior the interview (AOR 0.67; 95% CI 0.470, 0.951).
Child’s characteristics, sex and perceived weight of the child at birth by the mother are significantly associated with stunting among children age 6-23 months. Female children were 55% less likely to be stunted than male children (AOR 0.45; 95% CI 0.359, 0.552). Among children with a perceived birth size of less than average, the odds of stunting were 88% higher than those whose mothers said the birth size was more than average (AOR 1.88; 95% CI 1.381, 2.557). aternal characteristics such as the interval between the births, mother’s employment status and maternal education were sig-nificantly associated with stunting however, the odds of stunting among children 6-23 months appear to reduce with increasing lev¬el of education. Children born from mothers with anaemia (<11g/ dl) had 36% higher odds of being stunted than children born from mothers with no anemia (AOR 1.36; 95% 0.061, 1.744).
Among children from rich households, the odds of stunting were 43% lower than children from poor households (AOR 0.57; 95% CI 0.365, 0.889). The use of the internet by mothers at the house¬hold level was significantly associated with child stunting. The odds of stunting among children whose mothers reported the use of the internet within 12 months prior to the 2018 ZDHS were 54% lower than those who have never used or used more than 12 months ago (AOR 0.47; 95% CI 0.190, 1.135). Some coefficients on the IYCF practices variables (minimum acceptable diet and consumption of iron-rich foods) failed to reach statistical signifi¬cance at the 95% level and the variable minimum meal frequency failed collinearity test with other IYCF practices variables hence, and thus was not included in the final model.
Table 3: An Association between IYCF Practices and Stunting among children age 6-23 months adjusted for other variables (Child, Maternal and Household characteristics)
|
Characteristic |
AOR |
95% CI |
|
IYCF Variables |
||
|
Currently Breastfed |
||
|
No |
1 |
|
|
Yes |
0.616*** |
[0.477, 0.796] |
|
Minimum Acceptable Diet |
||
|
No |
1 |
|
|
Yes |
1.373 |
[0.894, 2.107] |
|
Minimum Dietary Diversity |
||
|
No |
1 |
|
|
Yes |
0.669** |
[0.470, 0.951] |
|
Consumption of Iron-Rich Foods |
||
|
No |
1 |
|
|
Yes |
1.207 |
[0.945, 1.543] |
|
Childs Characteristics |
||
|
Sex of the Child |
||
|
Male |
1 |
|
|
Female |
0.446*** |
[0.359, 0.552] |
|
Perceived Size of Child at Birth (Average and above) |
||
|
Average and Above |
1 |
|
|
Below Average |
1.879*** |
[1.381, 2.557] |
|
Maternal Characteristics |
||
|
Birth Interval Group |
||
|
>=24 Months |
1 |
|
|
< 24 Months |
0.895 |
[0.605, 1.324] |
|
Mother’s Level of Education |
||
|
No Education |
1 |
|
|
Primary |
0.953 |
[0.665, 1.365] |
|
Secondary |
0.987 |
[0.656, 1.484] |
|
Higher |
0.587 |
[0.185, 1.862] |
|
Mother’s Employment Status |
||
|
Not Working |
1 |
|
|
Working |
1.003 |
[0.804, 1.252] |
|
Maternal Anaemia (<11g/dl) |
||
|
No Anaemia |
|
|
|
Yes |
1 |
|
|
Household Characteristics |
1.361** |
[1.061, 1.744] |
|
Wealth Index |
||
|
Poor |
|
|
|
Middle |
1 |
|
|
Rich |
0.942 |
0.190, 1.135] |
|
Use of the Internet |
0.569** |
[0.365, 0.889] |
|
Never or more than 12 months |
||
|
Yes, Last 12 Months |
1 |
|
|
|
0.465* |
[0.190, 1.135] |
|
***p<0.01, ** p<0.05, *p<0.1; AOR= Adjusted odds Ratio |
||
Discussion
This study investigated the influence of IYCF practices on stunting in children age 6 – 23 months in Zambia using the 2018 ZDHS data. Specifically, the study sought to determine the influence that breastfeeding, Minimum Acceptable Diet, Minimum Dietary Diversity , Minimum Meal Frequency and consumption of Iron rich-foods have on child stunting in Zambia and to determine the child, maternal and household characteristics associated with child stunting in Zambia. The study, based on a sufficiently large sample of nationally representative women in Zambia found that, the level of under-five child stunting is at 35% and is the highest in Sub-Saharan Africa, it is only 4 percentage points short of the developing world average (39%) and 5 percentage points short of the sub-Saharan regional average of 40% [2]. Despite the reduc- tion in Stunting levels from 53% in 2001-02 to 35% in 2018, stunt¬ing remains a public health challenge. More so, stunting among children age 6-23 months, a critical period for child growth and development, is even higher at 36%. The importance of age range 6-23 months for the growth and development of children as it af¬fects both the physical and mental growth of a child cannot be over-emphasized. Zambia’s Ministry of Health recognizes that ad¬equate nutrition is critical to children’s growth and development and that the period from birth to age two is especially important for optimal physical and cognitive growth and development [17]. Stunting is the devastating result of poor nutrition in early child¬hood. Children suffering from stunting may never grow to their full height and their cognitive ability may never develop to their full potential [9].
While the findings show interesting associations, the fact that DHS data are cross-sectional is an inherent limitation in this study, as causal relationships cannot be established. Besides, despite the large sample size to enable the identification of the factors associ¬ated with stunting, sub-analysis to assess the relationship between the many co-variates was not possible due to the few cases of the sample in each sub-group. For instance, we would have liked to in¬vestigate the likelihood of stunting for children without minimum acceptable diet and consumption of iron-rich foods but these co¬efficients could not reach statistical significance at 95% level and minimum meal frequency failed collinearity test with other IYCF practices variables. This however, does not negate the importance of findings at sub-population level that give substantial insight in the possible determinants of nutrition deficiencies in young chil¬dren.
We identified IYFC practices that influence stunting in Zambia. Our findings suggest that children who are breastfed and have min-imum dietary diversity are less likely to be stunted compared to children who were not. Children age 6-23 months who were still breastfeeding had lower odds (38%) (AOR 0.62; 99% CI 0.48, 0.79) of being stunted. The findings also show lower odds of stunt-ing ((AOR 0.67; 95% CI 0.47, 0.95) among children who had min-imum dietary diversity. This shows that breastfeeding plays a sig-nificant role in averting stunting in children 6-23 months. These findings suggest that breastfeeding up to the recommended dura-tion of 24 months or beyond especially in low resource settings like Zambia can significantly reduce stunting. Dietary diversity as complementary feeding is introduced together with gradual wean¬ing can avert the stunting levels in Zambia [18] . Evidence from other studies suggest that interventions that promote and support optimal breastfeeding practices and enable increased consumption of nutritious local foods have potential to contribute to reducing stunting [22]. Further, nutrition-specific interventions targeted at improving IYCF practices, dietary diversification and intake of nutrient-rich meals, should be adopted and scaled up to address undernutrition23.
This study identified several children, maternal and household characteristics associated with stunting among children 6-23 months in Zambia. The findings suggest that sex of the child, child’s age, perceived size of child at birth, receipt of vitamin A supplementation and child’s anaemia are significantly associated with stunting, the results are consistent with other studies on stunt-ing among children age 6-23 months [19-21].
Further, male children, older children (18-23 months), children with a perceived low birth size and children who did not receive Vitamin A supplementation are more likely to be stunted. UNICEF indicates that painful and debilitating cycles of illness, depressed appetite, insufficient food and inadequate care contribute to stunt¬ing. Many children do not survive such detriment while many of those who do survive carry long-term defects in mental capacity along with losses in stature [2]. Analysis of maternal characteristics showed that children 6-23 months from rich households had the lowest odds of being stunted. Other maternal characteristics sig¬nificantly associated with stunting are education, access to the in¬ternet and the number of antenatal visits attended. Children whose mothers had more education, access to the internet, attended ANC, belonged to the rich wealth index category were less likely to be stunted. These findings are consistent with the findings from oth¬er studies in sub-Saharan Africa [20-22]. These associations come as no surprise because women who are educated, mostly live in urban areas where there is internet access and are more likely to know how to use the internet, have better health-seeking behaviour and access to health facilities to attend ANC and can afford to buy foods that are dietary diverse as well as know how to prepare them. A high maternal education translates into greater health care uti¬lization, adoption of modern medical practices and greater female autonomy, which in turn influences health-related decisions that improve child nutritional outcomes [22].
Children with a birth interval of fewer than 24 months have lower odds of being stunted. Due to the lower birth interval, one would expect that breastfeeding duration is less than 24 months and care may be inadequate and therefore stunting could be more prevalent but the results showed otherwise. We did not, however, explore the household or maternal characteristics of these children to de¬termine whether this unexpected finding is due to the latter factors. We can, however, speculate that these children may have received adequate care and were well-nourished despite having a less than 24 months birth interval.
Stunting among children age 6-23 months differs by rural-urban and regional areas. Stunting was more prevalent in rural areas than in urban areas. Children in rural areas have higher odds of being stunted compared with counterparts in urban areas. Our findings differ from a study conducted in Cambodia which showed lower odds for children in rural areas [23]. The difference in findings could be explained by many socio-economic differences which this study did not seek to explore.
Conclusion and Policy Implications
With 36% of children age 6-23 months stunted, this child nutrition is still a public health challenge in Zambia. The study identified sex of child, perceived size of child at birth, household wealth and mother’s internet access as strong determinants of stunting. Male children and children with perceived low birth size were more likely to be stunted whereas children from rich households have the lowest odds of stunting. Children with mothers who have in¬ternet access also have lower odds of being stunted. Maternal ed¬ucation and antenatal attendance are significantly associated with stunting. Stunting levels reduce with increase in mother’s educa¬tion and an increase in wealth status. Breast feeding and Minimum Dietary Diversity are two important IYCF practices that influence stunting. Children who are breastfed and have minimum dietary diversity are less likely to be stunted. We, therefore, recommend that programmes on Infant and Young Child Feeding should em-phasise breastfeeding especially in low-resource settings like Zambia and promote dietary diversity in order to reduce stunting. Further, IYCF practices such as breastfeeding and dietary diver-sity should be emphasized during mothers ANC and PNC visits. ANC and PNC attendance should be encouraged for all mothers to promote good nutrition during pregnancy; monitor growth of children and health of mothers; as well as provide information on IYCF best practices and prevent illnesses that may lead to stunt¬ing. Accelerated investment in nutrition programs and health ed¬ucation on IYCF are essential to reduce child stunting in Zambia. Further, to yield a sustainable improvement in child nutrition in Zambia, a holistic multi-sectoral approach is needed that targets the IYCF practices and socio-economic factors associated with stunting, thereby setting the country on the path to achieving the WHO global nutrition target by 2025 and achieving the SDG’s target to end preventable deaths of newborns and children under 5 years of age, with the aim to reduce neonatal mortality to at least as low as 12 per 1,000 live births and under-5 mortality to at least as low as 25 per 1,000 live births by 2030.
Declarations
Acknowledgements
Not Applicable
Authors’ contributions
AB contributed to the conception and design of the study; AB and ETN did the literature search; AB performed the statistical anal¬ysis; AB wrote the first draft of the manuscript. AB, ETN, CCM, BBB and NM contributed to manuscript revision, read, and ap¬proved the submitted version.
Funding
None.
Availability of data and materials
Data used in this article are available to bona fide researchers on request from the DHS program
Ethics approval and consent to participate
Not Applicable
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interest.
References
- W. H. O. Antonio and S. Weise, “WHO Global Nutrition Target : Stunting Policy Brief,” Who, 2010.
- UNICEF, World Health Organization [WHO], and World Bank, “Levels and trends in child malnutrition: Key Findings of the 2020 Edition of the Joint Child Manutrition Estimates,”2020. doi: 10.18356/6ef1e09a-en.
- B. Omilola and N. A. Sanogo, “Health, nutrition, and economic development in Africa,” Public Heal. Open J, vol. 5, no. 1,pp. 14–16, 2020, doi: 10.17140/PHOJ-5-140.
- ZDHS, “Zambia Demographic and Health Survey 2018; Zambia Statistical Agency, Ministry of Health & ICF,” 2018.
- World Health Organization [WHO], “Global Nutrition Targets 2025: Stunting Policy Brief,” 2014. doi: 10.1057/9781137477699_6.
- World Health Organization [WHO], “Indicators for assessing infant and young child feeding practices,” 2010. doi: ISBN 978 92 4 159975 7.
- M. K. I. & U.-G. Gerdtham, “Moving towards universal coverage-about the series,” 2006. Accessed: Apr. 09, 2020. [Online]. Available: www.who.int/reproductive-health/mtuc.
- B. Mzumara, P. Bwembya, H. Halwiindi, R. Mugode, and J. Banda, “Factors associated with stunting among children below five years of age in Zambia: evidence from the 2014 Zambia demographic and health survey,” BMC Nutr., vol. 4, no. 1,pp. 1–8, 2018, doi: 10.1186/s40795-018-0260-9.
- NFNCZ, “The first most critical days: Three year programme 2013-2015,” no. December 2012, pp. 2011–2015, 2012, [On-line]. Available: http://scalingupnutrition.org/wp-content/up-loads/2013/04/Zambia_First-1000-Most-Critical-Days-Pro-gramme_2013-2015.pdf.
- UNICEF, “First 1000 Days; The Critical window to ensure that Children survive and thrive,” 2017.
- M. Katepa-Bwalya, V. Mukonka, C. Kankasa, F. Masaninga,O. Babaniyi, and S. Siziya, “Infants and young children feeding practices and nutritional status in two districts of Zambia,” Int. Breastfeed. J., vol. 10, no. 1, 2015, doi: 10.1186/s13006-015-0033-x.
- United Nations Children’s Fund, “Programming guide infant and young child feeding,” Nutr. Sect. UNICEF, no. May, p. 173, 2011, doi: http://www.unicef.org/nutrition/files/Final_ IYCF_programming_guide_2011.pdf.
- C. P. Stewart, L. Iannotti, K. G. Dewey, K. F. Michaelsen, and A. W. Onyango, “Contextualising complementary feeding in a broader framework for stunting prevention,” Matern. Child Nutr., vol. 9, no. S2, pp. 27–45, Sep. 2013, doi: 10.1111/ mcn.12088.
- Kyaw Swa Mya, Aung Tin Kyaw, and Thandar Tun, “Feeding Practice and Nutritional Status of Children Age 6-23 Months in Myanmar: Further Analysis of the 2015-16 Demographic and Health Survey,” PLoS One, no. June No. 136, pp. 1–13, 2018.
- G. A. Ettyang and C. J. Sawe, “Factors Associated with Stunting in Children under Age 2 in the Cambodia and Kenya 2014 Demographic and Health Surveys,” 2016.
- UNICEF, “Programming guide infant and young child feed-ing,” 2011. doi: http://www.unicef.org/nutrition/files/Final_ IYCF_programming_guide_2011.pdf.
- MOH, “Zambia National Health Strategic Plan 2017-2021,” 2017.
- J. Krasevec, X. An, R. Kumapley, F. Bégin, and E. A. Fron-gillo, “Diet quality and risk of stunting among infants and young children in low- and middle-income countries,” Matern. Child Nutr., vol. 13, no. November 2016, pp. 1–11, 2017, doi: 10.1111/mcn.12430.
- E. Agedew and T. Chane, “Prevalence of Stunting among Children Aged 6–23 Months in Kemba Woreda, Southern Ethiopia: A Community Based Cross-Sectional Study,” Adv. Public Heal., vol. 2015, pp. 1–6, 2015, doi: 10.1155/2015/164670.
- S. Nkurunziza, B. Meessen, J. P. Van geertruyden, and C. Kor-achais, “Determinants of stunting and severe stunting among Burundian children aged 6-23 months: Evidence from a na-tional cross-sectional household survey, 2014,” BMC Pediatr., vol. 17, no. 1, pp. 1–14, 2017, doi: 10.1186/s12887-017-0929-2.
- B. B. Bwalya, M. Lemba, C. C. Mapoma, and N. Mutombo, “Factors Associated with Stunting among Children Aged 6-23 Months in Zambian: Evidence from the 2007 Zambia Demographic and Health Survey,” Int. J. Adv. Nutr. Heal. Sci., vol. 3, no. 1, pp. 116–131, 2015, doi: 10.23953/cloud.ijanhs.146.
- B. J. Akombi, K. E. Agho, D. Merom, A. M. Renzaho, and J. J. Hall, “Child malnutrition in sub-Saharan Africa: A meta-anal-ysis of demographic and health surveys (2006-2016),” PLoS One, vol. 12, no. 5, p. e0177338, May 2017, doi: 10.1371/ journal.pone.0177338.
Appendix
Childhood Stunting Framework Adapted from the WHO Framework for Childhood Stunting