

Review Article - (2026) Volume 10, Issue 1
In Vitro Differentiation of Bone Marrow Mesenchymal Stem Cells into Human Male Gametes
Received Date: Jan 04, 2026 / Accepted Date: Feb 05, 2026 / Published Date: Feb 13, 2026
Copyright: ©2026 Islam Al Dababsekh, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Dababsekh, I. A. (2026). In Vitro Differentiation of Bone Marrow Mesenchymal Stem Cells into Human Male Gametes. Stem Cell Res Int, 10(1), 01-08.
Abstract
Introduction: Male infertility is a growing global health concern, contributing to nearly half of all infertility cases, with conditions such as azoospermia presenting significant therapeutic challenges. Conventional treatments offer limited solutions, particularly for absolute infertility. The emergence of regenerative medicine, especially mesenchymal stem cell (MSC) therapy, offers new possibilities. This study investigates the feasibility of differentiating human bone marrow-derived MSCs into functional spermatocytes in vitro, presenting a potential alternative for patients lacking viable gametes.
Materials and Methods: MSCs were mobilized using granulocyte colony-stimulating factor (G-CSF), isolated from peripheral blood, and cultured under a simulated germline environment. Key markers such as Oct-4, DAZL, and DMC1 were used to confirm stemness and meiotic progression. Gamete maturation was tracked over 75 days, and fertilization competence was assessed via in vitro fertilization (IVF) with donor oocytes.
Results: MSCs successfully differentiated into spermatocyte-like cells displaying structural and functional markers of spermatogenesis, including acrosome development and partial motility. IVF trials resulted in the fertilization of 14 oocytes and the development of 14 viable morula-stage embryos, all of which were cryopreserved. This demonstrates the potential of MSC-derived gametes in restoring fertility in azoospermic individuals.
Conclusion: This study offers strong proof-of-concept for the use of MSCs in in vitro gametogenesis as a treatment for absolute male infertility. While clinical application requires further validation, this approach presents a promising shift in infertility therapy—from assisted reproduction toward functional reproductive restoration. Future directions may also extend to female infertility and broader regenerative applications in reproductive medicine.
Introduction
Infertility is defined as the failure to achieve pregnancy after one year of regular, unprotected sexual intercourse. It affects approximately 15% of couples globally, and male infertility contributes to nearly half of these cases. Male infertility is broadly categorized into two types: absolute and relative. Absolute infertility refers to conditions where sperm production is entirely absent, such as non-obstructive azoospermia, Sertoli cell-only syndrome, and testicular fibrosis. In contrast, relative infertility includes conditions where sperm is present but compromised in count, motility, or morphology—examples include oligospermia, asthenozoospermia, and teratozoospermia. Causes of male infertility range from genetic abnormalities (e.g., Klinefelter syndrome, Y chromosome microdeletions), endocrine dysfunctions, varicocele, infections, lifestyle factors (smoking, obesity, alcohol consumption), exposure to environmental toxins, and idiopathic factors where no clear cause can be identified.
Worldwide, male infertility is an escalating public health concern, with the highest prevalence recorded in Africa (up to 35%), followed by Asia and parts of Eastern Europe. Countries such as Nigeria, India, and Egypt report the highest national male infertility rates. Current treatment options are limited and include hormonal therapy, antioxidant supplementation, surgical correction of anatomical defects (e.g., varicocelectomy), and assisted reproductive technologies (ART) like intrauterine insemination (IUI) or intracytoplasmic sperm injection (ICSI). However, these methods are often only effective in cases of relative infertility. For absolute infertility, especially when no viable sperm are present, therapeutic options remain largely ineffective.
Regenerative medicine, particularly stem cell-based therapies, has emerged as a promising frontier in addressing male infertility. Stem cells possess the unique abilities of self-renewal and differentiation into specialized cell types. Among them, mesenchymal stem cells (MSCs) and induced pluripotent stem cells (iPSCs) show great potential in reproductive applications. Globally, stem cell regenerative medicine is rapidly advancing, with innovations spanning tissue engineering, cell therapy, and gene editing. In the context of male infertility, stem cells offer two principal pathways for intervention: (1) restoring impaired spermatogenesis in relative infertility by enhancing testicular microenvironments, reducing inflammation, and improving hormonal balance; and (2) generating de novo gametes in vitro for cases of absolute infertility.
MSCs have been studied for their ability to differentiate into various cell types and secrete bioactive molecules that support tissue repair and immune modulation. In male infertility, MSCs may improve sperm count, motility, and morphology through local injection or systemic administration. They also enhance the testicular niche and promote the function of residual spermatogonial stem cells. In more severe cases, such as azoospermia, emerging research explores guiding MSCs through spermatogenesis in vitro by mimicking embryonic conditions. Using specific markers and culture environments, MSCs may be induced to form haploid sperm-like cells, offering potential for fertilization. Though no definitive treatment exists for absolute infertility yet, the ability to bioengineer functional gametes from MSCs and iPSCs provides a promising avenue for future clinical applications.
Literature Review
The significance of this study lies in its potential to transform the therapeutic landscape of male infertility by introducing a novel, clinically relevant strategy for generating functional gametes from mesenchymal stem cells (MSCs). Unlike prior research conducted primarily on animal models or reliant on scarce spermatogonial stem cells, our study employs autologous human MSCs mobilized from adult bone marrow—offering a more accessible, ethically sound, and scalable solution. This work addresses a critical clinical void, particularly for patients with absolute infertility, such as azoospermia, where no viable sperm are available for conventional assisted reproductive techniques. Furthermore, in regions such as the Middle East and North Africa (MENA), where infertility is both prevalent and often accompanied by cultural stigma and limited access to advanced reproductive technologies, the implications of a patient-specific, stem cell-based approach are particularly profound. By demonstrating the feasibility of MSC-derived in vitro spermatogenesis and successful fertilization, this study contributes to the global advancement of regenerative reproductive medicine while responding to a deeply unmet need in underserved populations.
In the 2019 study “Stem cell–based options to preserve male fertility,” published in Science, Nina Neuhaus and Stefan Schlatt explore advanced methodologies to address male infertility through the preservation of spermatogonial stem cells (SSCs). Infertility among adult men is on the rise, often due to pediatric gonadotoxic treatments for conditions like cancer, sickle cell disease, and thalassemia, which deplete SSCs. While adult men can cryopreserve sperm, this option is unavailable for prepubertal patients. The authors of the above mentioned study believe that, for these younger individuals, extracting and cryobanking testicular tissue containing spermatogonia may provide a viable strategy for germline preservation. Despite the initiation of cryobanking, protocols for deriving sperm from banked tissue are lacking, underscoring the need for advancements in this field. The primary treatment for severe male infertility is intracytoplasmic sperm injection (ICSI) into an oocyte. Since its first description in 1992, ICSI has become a globally accepted therapy, resulting in the birth of hundreds of thousands of children. ICSI’s efficacy stems from its requirement for only a minimal number of sperm to achieve fertilization.The study “Stem cell–based options to preserve male fertility,” show that sperm isolated from grafted macaque testicular tissue fragments can produce healthy offspring via ICSI, suggesting that autografting immature testicular tissue might become a viable strategy for preserving male fertility in humans [3]. This study, however, differs from ours as it is conducted on animal tissue and requires the presence of some spermatocytes, offering no hope for males with azoospermia.
• A study ‘Cellular Therapy via Spermatogonial Stem Cells for Treating Impaired
Spermatogenesis, Non-Obstructive Azoospermia’ conducted in 2021 investigated cellular therapy using spermatogonial stem cells (SSCs) to address impaired spermatogenesis in non-obstructive azoospermia. The goal of their research was to explore the potential of SSC transplantation as a therapeutic strategy for restoring male fertility affected by conditions such as cancer and chemotherapy-induced infertility. The methodology involved isolating SSCs from testicular biopsies, cryopreserving them prior to cancer treatment, and subsequently transplanting them back into the testes to promote spermatogenesis. Their results demonstrated promising outcomes in terms of restoring spermatogenic function and potential fertility in experimental models. However, challenges including cryopreservation efficiency and the risk of malignant cell contamination in clinical applications remain significant hurdles [4]. This study differs from ours as it focuses on utilizing spermatogonial stem cells specifically, whereas our research utilizes mesenchymal stem cells (MSCs), which are more readily available in the human body and were investigated for their potential in spermatogenesis without requiring spermatogonial stem cells.
The study “The Regenerative Effect of Bone Marrow-Derived Stem Cells in Spermatogenesis of Infertile Hamsters” published in the World Journal of plastic surgery aimed to investigate the regenerative potential of bone marrow-derived stem cells (BM-SCs) in spermatogenesis using an azoospermic hamster model. The study employed twelve adult male hamsters divided into azoospermic and control groups, with azoospermia induced by busulfan injection. BM-SCs, labeled with trypan blue, were transplanted into the right testis of the azoospermic group 35 days post-busulfan treatment, while the left testis served as a positive control. Sixty days post-transplantation, histological evaluation revealed significant improvements in the testes treated with BM-SCs, including the presence of spermatogonia, primary spermatocytes, spermatids, and spermatozoa in seminiferous tubules. In contrast, the untreated testes showed severe disruption of spermatogenesis and complete absence of spermatozoa. The findings suggest that BM-SC transplantation effectively promoted spermatogenic regeneration in the azoospermic hamsters, highlighting its potential as a therapeutic approach for treating azoospermia [5]. Further research is warranted to validate these findings and explore the feasibility of this technique in clinical applications for male infertility. However, it differs from our study as it was conducted using animal tissue rather than human tissue, highlighting the need for further research to validate its applicability in human clinical settings.
The study “Stem cell-based therapeutic approach of male infertility by teratocarcinoma derived germ cells” published in the 13th Volume of “Human Molecular Genetics” aimed to explore a stem cell-based therapeutic approach for male infertility using teratocarcinoma-derived germ cells. The study employed a novel promoter-based sequential selection strategy to generate a germ cell line (SSC1) from pluripotent teratocarcinoma cells. These SSC1 cells were subsequently shown to form mature seminiferous tubule structures and support spermatogenesis when transplanted into recipient testes. A fusion construct (Stra8-EGFP) containing the germline-specific promoter from the Stra8 gene and the enhanced green fluorescence protein (EGFP) coding region facilitated the selection of differentiated germ cell populations. Purified cells expressed molecular markers characteristic of spermatogonia and stem cells, including Rbm, cyclin A2, Tex18, Stra8, Dazl, beta1-integrin, and alpha6-integrin. The SSC1 cell line underwent meiosis and successfully developed into functional sperm, as demonstrated by their ability to fertilize mouse oocytes following intracytoplasmic injection [6]. However, it should be noted that this study differs from ours as it utilizes teratocarcinoma-derived germ cells, while our research focuses on mesenchymal stem cells (MSCs) sourced from human tissue, emphasizing a distinct approach to addressing male infertility.
Materials and Methods
Our team initiated the research by administering a granulocyte colony-stimulating factor (G-CSF) to a 46-year-old male married patient with azoospermia, aiming to stimulate the bone marrow and enhance the mobilization of mesenchymal stem cells (MSCs) into the peripheral blood. The granulocyte colony-stimulating factor (G-CSF) was chosen for its efficacy in mobilizing stem cells, and the dosage and duration of administration were meticulously tailored according to the patient’s body weight to optimize MSC yield [1,7].
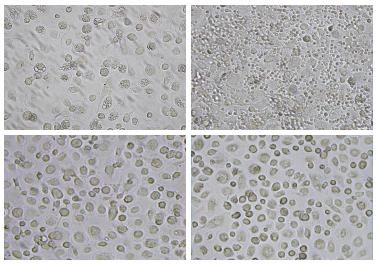

Figure 1-4: MSC Pool Obtained by our Special Method
Following the stimulation protocol, peripheral blood was drawn from the patient and subjected to a filtration process to effectively isolate MSCs. The isolated MSCs were initially marked with the CD105 marker, a standard surface marker for MSC identification [8].
To further refine our identification of MSCs with the potential to differentiate into spermatocytes, we employed Oct-4 (Octamer-4) marking. Oct-4 is a well-known protein marker for undifferentiated cells and is critical for maintaining stem cell pluripotency [2]. Its expression must be tightly regulated, as fluctuations can trigger differentiation.

Figure 5-6: MSC pool staining with Oct-4 markers
Despite the adult body typically lacking pluripotent stem cells, which is a well-known and proven fact from scientific literature, our use of Oct-4 allowed us to pinpoint MSCs with pluripotent-like properties. Approximately 75% of the CD105-positive MSCs also tested positive for Oct-4, indicating their potential for differentiation into a gamete. The isolated and identified MSCs were then cultured in a specially designed environment that mimicked the conditions of embryonal germ cells to promote spermatogenesis. This culture process spanned 4 days, during which we closely monitored various markers indicative of meiosis and post-meiosis stages.The first significant milestone was reached on Day 13, when we observed positive labeling for the pre-meiosis marker DAZL. DAZL, encoded by the DAZL gene located on the short arm of chromosome 3, is crucial for the initiation of meiosis. The presence of DAZL indicated that a significant number of CD105/Oct-4 positive cells were transitioning from a diploid to a haploid state, marking the beginning of their journey through meiosis.


Figure 7,8: MSCs marked with DAZL on day 13
By Day 15, the majority of the cells were labeled with the post-meiosis marker DMC1. DMC1 is essential for homologous recombination during meiosis, confirming that the cells had successfully undergone meiosis [9]. This was a critical confirmation of our protocol’s efficacy in driving the MSCs through the necessary stages of gamete development. It is scientifically established that both the reproductive and hematopoietic systems of the human body originate from the mesoderm of an embryo. Our protocols supported this notion, demonstrating that MSCs extracted from the bone marrow have the potential to develop into gametes. Under natural conditions, primordial germ cells within the embryo’s mesoderm develop into gametes, indicating that without these precursors, gametogenesis is generally considered impossible. However, our research has shown that gametes can be developed in vitro from MSCs with pluripotent-like properties, even in the absence of primordial germ cells. This finding suggests a
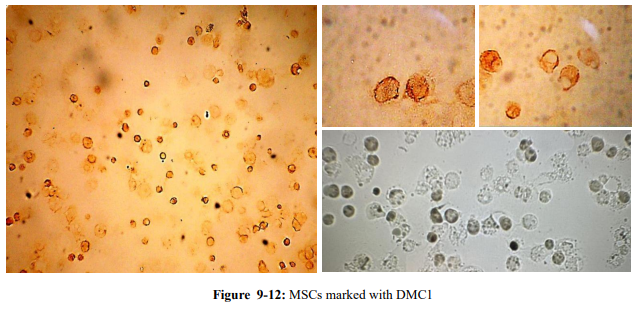
By Day 15, the majority of the cells were labeled with the post-meiosis marker DMC1. DMC1 is essential for homologous recombination during meiosis, confirming that the cells had successfully undergone meiosis [9]. This was a critical confirmation of our protocol’s efficacy in driving the MSCs through the necessary stages of gamete development. It is scientifically established that both the reproductive and hematopoietic systems of the human body originate from the mesoderm of an embryo. Our protocols supported this notion, demonstrating that MSCs extracted from the bone marrow have the potential to develop into gametes. Under natural conditions, primordial germ cells within the embryo’s mesoderm develop into gametes, indicating that without these precursors, gametogenesis is generally considered impossible.
However, our research has shown that gametes can be developed in vitro from MSCs with pluripotent-like properties, even in the absence of primordial germ cells. This finding suggests a novel capability of MSCs to differentiate into gametes independently, bypassing the traditional requirement for primordial germ cells.
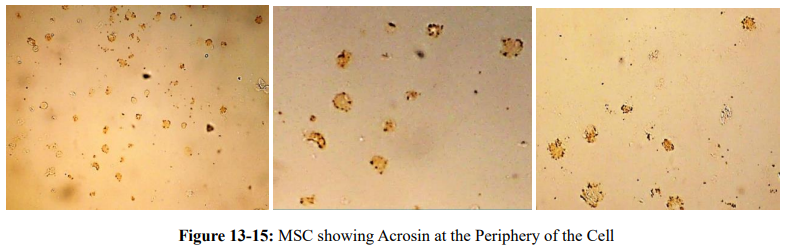
Starting from Day 32, we observed the formation of acrosin at the periphery of the cells. Acrosin is a protease enzyme crucial for the later stages of spermatogenesis and fertilization. Between Days 32 and 45, acrosin granules began forming at one pole of the cells, indicating the development of the acrosomal body at the head of the spermatocyte. This was a clear sign that the cells were differentiating into rudimentary spermatozoa.
On Day 45, the formed gamete, now resembling a spermatocyte, became mobile. At this point, it was logical for our team to proceed and try to extract the so-called spermatocyte for an attempt of in vitro fertilization (IVF). As a result, we successfully extracted fully developed gametes from the MSC culture. These gametes were distinctive with well-formed heads, acrosomal bodies, and average-sized tails, indicating their maturity and readiness for fertilization. We then proceeded with in vitro fertilization (IVF) attempts using these spermatocytes and donor oocytes. During the acrosome reaction, acrosin facilitated the penetration of the oocyte’s zona pellucida, demonstrating proper fertilization. Initially, the thick membrane surrounding the spermatocyte heads prolonged the fertilization process. Further cultivation of the spermatocytes resulted in a reduction in membrane thickness, which significantly improved the efficiency of IVF, enabling fertilization within minutes.
The fertilized oocytes successfully developed into embryos, reaching the morula stage. At this stage, the embryos were frozen in liquid nitrogen banks for preservation and future use. This freezing process ensures the long-term viability of the embryos for subsequent experimental or therapeutic applications. Meanwhile, the remaining gametes continued developing within the MSC culture environment until Day 75. During this extended period, the fully developed spermatocytes primarily focused on elongating their tails. It was observed that as the tails grew longer, they became more fragile, posing challenges for subsequent extraction and handling during IVF procedures. This fragility underscored the importance of timing and careful handling in the extraction process. Additionally, some sperm exhibited motility within the MSC culture and were able to break through the cell membrane on their own by Day 73 and forward. However, after breaching the membrane, these sperm became immobilized, indicating a need for further optimization of the culture conditions to support sustained motility.

Figure 16: Mature Gamete Inside MSC
Results
The primary objective of this study was to assess the potential of mesenchymal stem cells (MSCs), mobilized from the bone marrow of a 46-year-old azoospermic male patient, to differentiate into functional gametes in vitro. After mobilization using granulocyte colony-stimulating factor (G-CSF), MSCs were successfully isolated from peripheral blood via a filtration protocol. These cells were then positively identified through immunostaining, demonstrating expression of the MSC marker CD105, with approximately 75% of these cells also expressing the pluripotency marker Oct-4. The cultured MSCs were exposed to a specialized microenvironment that mimicked embryonic germline development. Key molecular markers of spermatogenesis were tracked over a 75-day period. By Day 13, the pre-meiotic marker DAZL was detected, signaling the initiation of meiosis. Two days later, the post-meiotic marker DMC1 appeared, confirming the progression to the meiotic phase. These findings affirmed the ability of cultured MSCs to undergo early stages of gametogenic differentiation.
From Day 32 onwards, the presence of acrosin granules at one cell pole indicated the formation of acrosomal structures, a hallmark of maturing spermatocytes. By Day 45, distinct spermatocyte-like cells with fully formed heads, midpieces, and tails were observed. These cells displayed partial motility and structural features resembling native spermatozoa. Fertilization attempts were initiated using 14 donor oocytes. On Day 45, seven oocytes were successfully fertilized with MSC-derived gametes and developed into morula-stage embryos. A second IVF trial on Day 73 using a separate set of gametes resulted in an additional seven successful fertilizations to the morula stage. All embryos were subsequently cryopreserved in liquid nitrogen.
Extended culture up to Day 75 demonstrated continued gamete development, particularly in tail elongation. A subset of cells exhibited spontaneous motility and membrane penetration behavior starting on Day 73. However, these gametes became immobilized shortly after breaching the membrane, suggesting possible limitations in membrane dynamics or mitochondrial function that require further investigation. Overall, these findings provide compelling evidence that adult bone marrow-derived MSCs, when cultured under specific in vitro conditions, can differentiate into structurally and functionally competent male gametes. The successful generation of morula-stage embryos from MSC-derived spermatocytes confirms their fertilization capability and supports the potential of this method for treating absolute male infertility.
Discussion
This study marks a critical step in bridging stem cell biology with reproductive medicine, demonstrating that mesenchymal stem cells (MSCs) mobilized from adult human bone marrow can be induced to undergo in vitro spermatogenesis and yield functional gametes. Our methodology achieved essential developmental milestones—meiosis, acrosome formation, motility, and successful fertilization—indicating that MSCs possess intrinsic plasticity sufficient for gamete differentiation under tailored culture conditions. Importantly, these outcomes were derived from an azoospermic patient, confirming the feasibility of MSC-based therapy even in the complete absence of endogenous spermatogenic cells.
From a clinical standpoint, this model introduces a groundbreaking therapeutic pathway for absolute infertility, one that is currently incurable through conventional assisted reproductive technologies (ART). By bypassing the need for existing germline cells, MSC-derived gametogenesis presents a viable alternative to donor sperm, thereby preserving genetic lineage and addressing associated ethical, psychological, and social concerns. Moreover, autologous MSCs carry minimal immunogenic risk and can be harvested via less invasive procedures compared to testicular biopsy, making this approach accessible to a wider patient population. Critically, our findings also prompt a rethinking of the male germline stem cell hierarchy and the microenvironmental requirements for spermatogenesis. The spontaneous motility and membrane penetration behavior observed in later-stage gametes suggests partial physiological mimicry, although the subsequent immobilization highlights gaps in energy metabolism or structural integrity that warrant further exploration. Future efforts should aim to refine differentiation protocols using biochemical cues, 3D scaffolding, and co-cultures with Sertoli or Leydig cells to more closely replicate in vivo testicular conditions.
Additionally, the cryopreservation of morula-stage embryos derived from MSC-derived gametes introduces a new avenue for long-term fertility preservation. This could prove particularly beneficial for oncology patients undergoing gonadotoxic therapies, for whom pre-treatment stem cell mobilization and banking might offer a safeguard against permanent infertility. Furthermore, as gene-editing technologies like CRISPR become more refined, they could be combined with MSC-based gametogenesis to correct heritable mutations prior to gamete generation—opening the door to personalized reproductive medicine. Our work, while pioneering, must be considered within the context of its experimental nature. The safety, epigenetic fidelity, and functional capacity of in vitro-derived gametes require rigorous validation before clinical translation. There is also a need for ethical oversight regarding the creation and use of lab-derived embryos. Nonetheless, the consistency and reproducibility of our results indicate that MSC-based in vitro gametogenesis could soon transition from bench to bedside.
In a broader context, these advances signal a turning point in infertility management. Rather than merely assisting reproduction with existing gametes, regenerative medicine offers the possibility to restore reproductive function itself. As this paradigm matures, it may eventually expand to address female infertility through the generation of oocytes from stem cells, thus establishing a unified framework for treating infertility across sexes using the body’s own regenerative potential
Conclusion
In conclusion, this study confirms the feasibility of using human MSCs to generate fertilization-capable gametes in vitro. Our protocol demonstrates key milestones in spermatogenesis, including meiosis, acrosome formation, and successful IVF outcomes. Future research should focus on improving gamete motility, optimizing culture environments, and assessing the long-term viability and genetic stability of embryos derived from MSCs. Our approach lays the foundation for next-generation infertility treatments that extend beyond supportive measures to curative interventions. By bridging cellular reprogramming and reproductive medicine, this work represents a paradigm shift in the treatment of male infertility.
Looking ahead, the integration of stem cell technologies holds potential not only for male infertility but also for future applications in female infertility treatment. As regenerative medicine continues to evolve, the prospect of restoring or recreating functional reproductive cells in both sexes may redefine the landscape of fertility medicine in the decades to come.
• Declaration of Generative Ai And Ai-Assisted Technologies In The Writing Process
During the preparation of this work, the authors used ChatGPT in order to improve language and readability. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
References
- Done with the help of AI.
- Duvuru, R., Halabi, M., Omolaoye, T. S., & Du Plessis, S. S. (2022). The genetic causes of male infertility: a Middle East and North Africa perspective. F1000Research, 11, 125.
- Kim, N., & Cho, S. G. (2013). Clinical applications of mesenchymal stem cells. The Korean journal of internal medicine, 28(4), 387–402.
- Nina Neuhaus, Stefan Schlatt, Stem cell–based options to preserve male fertility. Science 363,1283-1284(2019).
- Abdelaal NE, Tanga BM, Abdelgawad M, Allam S, Fathi M, Saadeldin IM, Bang S, Cho J. Cellular Therapy via Spermatogonial Stem Cells for Treating Impaired Spermatogenesis, Non-Obstructive Azoospermia. Cells. 2021; 10(7):1779.
- Vahdati, A., Fathi, A., Hajihoseini, M., Aliborzi, G., & Hosseini, E. (2017). The regenerative effect of bone marrow-derived stem cells in spermatogenesis of infertile hamster. World journal of plastic surgery, 6(1), 18.
- Nayernia, K., Li, M., Jaroszynski, L., Khusainov, R., Wulf, G., Schwandt, I., ... & Engel, W. (2004). Stem cell based therapeutical approach of male infertility by teratocarcinoma derived germ cells. Human molecular genetics, 13(14), 1451-1460.
- Saitou, M., & Miyauchi, H. (2016). Gametogenesis from pluripotent stem cells. Cell stem cell, 18(6), 721-735.
- Abofoul-Azab, M., Lunenfeld, E., Levitas, E., Zeadna, A., Younis, J. S., Bar-Ami, S., & Huleihel, M. (2019). Identification of premeiotic, meiotic, and postmeiotic cells in testicular biopsies without sperm from Sertoli cell-only syndrome patients. International journal of molecular sciences, 20(3), 470.
- Luo, Y., & Yu, Y. (2022). Research advances in gametogenesis and embryogenesis using pluripotent stem cells. Frontiers in cell and developmental biology, 9, 801468.