
Archives of Infectious Diseases & Therapy(AIDT)
ISSN: 2577-8455 | DOI: 10.33140/AIDT
Impact Factor: 1.385


Research Article - (2024) Volume 8, Issue 2
Impact of the Introduction of Artesunate on the Management of Severe Malaria in Casamance (Senegal): A Comparative Analysis of Data From 2016 and 2020
2Department of Infectious Diseases, Peace Hospital in Ziguinchor, Senegal
3Department of Anaesthesia and Resuscitation, Peace Hospital in Ziguinchor, Senegal
4Department of Nephrology, Regional Hospital in Ziguinchor, Senegal
5Department of Parasitolgy and Mycology, Regional Hospital in Ziguinchor, Senegal
6Department of Hematology, Peace Hospital in Ziguinchor, Senegal
7Microbiology Department of the Peace Hospital in Ziguinchor, Senegal
8Department of Nutrition, Cheikh Anta Diop University, Senegal
9Department of Pneumology, Peace Hospital in Ziguinchor, Senegal
Received Date: Apr 28, 2024 / Accepted Date: May 15, 2024 / Published Date: May 23, 2024
Copyright: ©Â©2024 Kalilou Diallo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Diallo, K., Sambou, P., Dionou, J. C., Kane, Y., Diop, A., et al. (2024). Impact of the Introduction of Artesunate on the Management of Severe Malaria in Casamance (Senegal): A Comparative Analysis of Data From 2016 and 2020. Archives of Infect Diseases & Therapy, 8(2), 01-09.
Abstract
Background: the implementation of different control strategies, including the treatment of severe forms with injectable artesunate, has made it possible to significantly reduce malaria in Senegal. Despite everything, malaria remains a concern in Senegal, especially in the southern regions, hence the interest in studying these characteristics and their evolution over time.
Objectives: describe the epidemiological, clinical and evolving aspects of severe malaria before and after implementation of artesunate treatment.
Patients and methods: retrospective, cross-sectional, descriptive and analytical study focusing on cases of severe malaria admitted in two health structures in the Vélingara district in 2016 and 2020. The severity of diagnosis was made based on the current criteria of the WHO and confirmation made by thick blood smear and/or HRP2 rapid diagnostic test. The data was entered into Excel and analyzed with Epi-info version 7.2.6.
Results: In 2016, 357 cases of serious malaria were recorded from January 1st to December 31st, with 75.6% in October and December. The average age is 16.2 ± 12.9 years, with a predominance of the age group 6-15 years (38,94%). There was a male predominance and the sex ratio was 1.01. Coma (57%), convulsions (34%) and jaundice (14%) were the most common signs of severity. Under treatment with quinine salts (97%) and artemether (3%), the lethality was 5%. Factors significantly associated with death were rural origin (p:0.009), coma (p:0.000), hepatomegaly (p:0.03) and diffuse hemorrhages (p:0.03).
In 2020, 456 cases were collected from July 1st to December 31st, with 75.44% in October and November. The average age was 15.38±15.36 years (1 to 85 years) with a predominance of age group 6 to 15 years (46.49%). There was a male predominance and the sex ratio was 1.06. The signs of severity were dominated by prostration (52.63%), repeated convulsions (17.11%), coma (7.9%) and jaundice (7.2%). All patients were treated with injectable artesunate with a lethality of 3.5%. Death was significantly associated with coma (p:0.000) and the occurrence of respiratory failure (p:0.000).
Conclusion: severe malaria remained a childhood pathology with neurological manifestations predominating in Vellingara. A drop in lethality is observed with the generalization of artesunate-based treatment.
Keywords
Severe Malaria, Clinico-Biological Aspects, Casamance (Senegal)
Introduction
Malaria remains a major public health issue, especially in sub-Sa-haran Africa [1] despite the financial support from major interna¬tional initiatives such as the Global Fund, the American presiden¬tial initiative against malaria, the Roll Back Malaria program and the declaration of 'Abuja [2, 3], These investments made it possible to develop and implement controlling and preventive strategies, targeting pregnant women and children, which led to a significant reduction of the incidence of malaria [4].
The transition from quinine to artesunate represents an important step in improving the management of severe cases of malaria. In¬deed, the WHO recommends artesunate as first-line treatment for severe Plamodium falciparum malaria in adults and children after the publication of results of comparative clinical trials which il¬lustrated not only the superior effectiveness of artesunate, but also its better safety profile, in comparison with quinine which was the reference treatment for decades [5, 6].
In Senegal, malaria is mainly caused by P. falciparum, represent-ing 98% of cases, followed by P. malariae and P. ovalae [7]. The WHO reported in 2020 that 0.7% of deaths worldwide due to ma¬laria were recorded in Senegal [4].
The implementation by the national malaria control program (PNLP) of interventions with proven effectiveness as recommend-ed by the WHO resulted at the operational level in an improvement in the access and the quality of treatment through access to the RDT rapid diagnostic test (HRP2), the dispensation of antimalarial drugs such as injectable artesunate for severe forms, acceptance of the use of insecticide-treated mosquito nets as a useful means of prevention, just like the use of intermittent preventive treat-ment (IPT) in pregnant women and chemo-prevention of seasonal malaria (CPS) in children aged 3 to 120 months. Despite the im¬plementation of these different prevention strategies, malaria re¬mains endemic throughout the national territory, particularly in the south-eastern regions of Senegal [8]. We conducted this study in that region to describe the epidemiological, clinical and evolving aspects of severe malaria before and after the implementation of artesunate treatment.
Materials and Methods
Type and framework of the study: The study took place in two health structures in the department of Velingara located in the region of Kolda, southeast of Senegal.
This is a cross-sectional, descriptive and analytical study covering 813 patients' files admitted to the two health centers in the Velingara department, including 357 collected from January 1st to December 31st, 2016 in the Velingara health center and 456 from July 1st, 2020 to December 31st, 2020) in the Medina Gounass health center.
In 2016, injectable quinine was the first-line treatment for severe malaria. Quinine base: 25 mg/kg/day divided into 3 infusions of 4 hours in 10% glucose serum to be repeated every 8 hours for 5 to 7 days then followed by quinine or ACTs as soon as the oral route is possible. Artemether: 3.2 mg/kg of body weight at admission then 1.6 mg/kg per day.
In 2020, the first-line treatment for severe malaria is injectable artesunate. Artesunate: 2.4 mg/kg body weight administered intravenously (IV) or intramuscularly (IM) at admission (t = 0), then 12 and 24 hours later and, thereafter, once daily until the patient is able to take their medication orally
Study population
Inclusion criteria: all patients included were cases of severe malar¬ia. The diagnosis of severity was made based on the current WHO criteria [9], namely: the presence of asexual forms of Plasmodium falciparum in the thick film and in the blood smear associated with one or more of the severity criteria of the WHO. In the absence of a thick film or smear, the diagnosis of severe malaria was made based on the positivity of the HRP2 rapid diagnostic test, and treat¬ment for severe malaria was administered.
Non-Inclusion Criteria
We did not include suspected severe malaria not confirmed by par-asitological examination or RDT, pregnant women, and all other patients whose medical records were incomplete or did not meet the diagnostic criteria for severe malaria. Data collection: Data were collected from patients' medical re-cords, hospitalization and treatment records. Survey forms were completed based on information collected from patients' medical records and hospitalization records. For each patient, a form was established including socio-demographic aspects (age, sex, geographical origin), clinical aspects (date of consultation, clinical signs of severity of malaria, associated clinical signs), Para clinical aspects (biological signs of severity, other associated biological signs), therapeutic aspects (antimalarial treatment) and outcome aspects (duration of hospitalization, progressive modalities).
Statistical Analyses
Data were calculated using Excel 97-2003 and analyzed using Sta-ta/Special 16 software (Stata Corporation, Texas and USA). Re-sults were expressed as mean ± standard deviation for continuous variables and as proportion for categorical variables. Student's t test was used for mean comparisons and Pearson's chi-square test for comparison of categorical variables. P values <0.05 were con¬sidered significant for all analyses.
Results
Of the 813 cases of severe malaria included in this study, 459 cases observed in 2020 were treated with artesunate and 357 cases in 2016 were treated with quinine (97.20%) or artemether (2.80%). The average age of the patients did not differ significantly between the two groups (15.38±15.36 versus 14.86±16.72, p=0.643) and the age group of 6-15 years was predominant in the two groups (46.49% vs 38.94; p=0.031) (Table1). The number of cases was higher in the months of October (30.81% vs 27.41%), November (48.02% vs 31.37%) and December (9.42% vs 13.44%) with a peak of cases in November (Figure1).
The predominant signs of severity in 2016 and 2020 were repre-sented by disturbances of consciousness (57% versus 32.5%, P= 0.029), repeated convulsions (34% versus 19.8%, P<0.001), and jaundice (14% versus 76.4%, P = 0.017). In addition to these se-rious signs, fever was noted in 350 cases (98%), vomiting in 134 cases (37.5%) and diarrhea (6.4%) (Figure2) . The average length of hospitalization was significantly lower in patients treated with artesunate (1.59 ± 0.78 vs 3.22 ± 1.99 days; (P < 0.0000) (Table 3).
Rapid diagnostic tests for malaria were performed in 100% of cas-es. The thick smear was performed in 240 patients or 67% in 2016 compared to 96 (21.05%) in 2020.
The average parasite density before starting treatment was significantly lower in patients diagnosed in 2020 (11833.88±22432.99 vs 34967.97± 62955.38; (p=0.0005) however, a significantly greater proportion of hyperparasitemia was observed in 2020 (78.51 % vs 48.18%; p =0.000).
The average hemoglobin level was similar in the two groups (8.93 ± 2.75 versus 8.93 ± 2.75, p = 0.9902). The proportion of cases of severe anemia with a hemoglobin level <7 g/dl was greater among patients in 2016 compared to 2020 but the difference was not significant (11.20% versus 7.46%; p: 0.065) (Figure 2).
The average blood sugar level was 1.09±0.42 g/l in 2016 with a proportion of 5% cases of hypoglycemia < 0.5 mg/l compared to 1.27±0.47 in 2020 with a proportion 1.97% of cases of hypoglycemia < 0.5 mg/l.
All cases collected in 2020 were treated with artesunate while the majority of cases included in 2016 were on injectable quinine and (2.80%) were on arthemeter (Table 3). The fatality rate was slightly lower in patients treated with artesunate in 2020 compared to those treated with quinine or artemether in 2016. Factors significantly associated with death in 2016 were coma (p:0.000) (Table5). In 2020, death was significantly associated with coma (p: 0.000) and the occurrence of respiratory failure (p: 0.000).
Discussion
This retrospective descriptive and analytical study aimed to describe the epidemiological, clinical and evolving aspects of severe malaria before and after the implementation of artesunate treatment.
In terms of frequency, our results are higher than those of Diop in 2010, who reported 181 cases over 4 years [10] and Wade, who reported 87 cases over a period of 2 years [11] in Dakar, Senegal. This reflects the geographic disparities in terms of transmission and incidence of malaria in Senegal, like many African countries. Indeed, the southeastern regions of Senegal are characterized by a Sudanian-type climate with longer and more intense rainy seasons favoring the reproduction of mosquito vectors. Our results are also superior to those of a study carried out in Ivory Coast which identified 274 cases over 14 years [12]. On the other hand, our results are similar to those of a study carried out in Congo by Ntabi et al. [13] who found 241 cases over one year or 31.2%.
The number of cases was higher in the months of October, November and December corresponding to the rainy season. This observation is found in several studies carried out on severe malaria in Africa [10, 12, 14,15]. Senegal is classified as a sub-Saharan African country where malaria is endemic, with seasonal transmission mainly during the rainy season, according to the National Malaria Control Program [8].
The age profile for the onset of serious malaria in our region remains young with a male predominance. These profiles are comparable with those obtained in other regions across our country and in sub-Saharan Africa [13,16]. Indeed, children in particular age groups 6-15 years and those under 5 years are more vulnerable to severe malaria due to their still developing immune systems, as well as increased exposure and susceptibility to higher parasite loads. The male predominance could be explained by the fact that boys are inclined to carry out activities with a greater risk of exposure to mosquitoes.
In our study, the reasons for consultation were dominated by fever, vomiting and headache. Regarding fever, it remains the most common reason for consultation in most studies [2,17].
The predominant signs of severity in 2016 and 2020 were repre-sented by disturbances of consciousness (57% versus 32.5%, P= 0.029), repeated convulsions (34% versus 19.8%, P<0.001), and jaundice (14% versus 76.4%, P = 0.017). The predominance of cerebral malaria, especially in children over six months and under five years of age, has been noted by several authors [18,19]. Jaundice is often linked to liver damage, which is very common in adults, as highlighted by other authors [20,21]. These results could be influenced by traditional herbal medicine, which lengthens con-sultation times [20,21].
The rate of severe anemia was higher in 2016 compared to 2020. Our results are lower than those found by several authors in the sub-region [10,23, 24]. Anemia is linked to the lysis of parasitized red blood cells but also to the release of plasma toxins [25]. In addition, there is said to be deficiency anemia in sub-Saharan Africa among children under five years of age, to which malaria is linked [26]. It is considered as a poor prognostic factor [27].
Cases of respiratory distress represented only 4% in 2016 and 0.8% in 2020 in our series. Respiratory distress during malaria can result mainly from metabolic acidosis which is probably underes-timated because the measurement of respiratory gases blood was not systematically available in our public services, which could constitute a bias. This result is much lower than the result of Wade [11] [9] who obtained 38% in a study of 87 patients. Respiratory distress is aggravated by severe anemia and disseminated intra-vascular coagulation, linked to hyperparasitemia and Plasmodium falciparum infection.
The average parasite density before starting treatment was significantly lower in patients diagnosed in 2020 (11833.88±22432.99 p/ µL vs 34967.97± 62955.38 p/µL; (p=0.0005) (Table 2) however there was a proportion of cases of significantly greater hyperparasitemia in 2020 (78.51% vs 48.18%; p = 0.000). In several studies carried out in Senegal, the parasite density remains high [28,29]. A study conducted by Kotepui .M and al [30] and Rodriguez. P and al [31] showed an increase in parasite density with correlation to signs of severity.
The average length of hospitalization was significantly lower in patients treated with artesunate (1.59 ± 0.78 vs 3.22 ± 1.99 days). This reduction in the duration of hospitalization under artesunate was observed in the study of Cisse VPM et al. in Dakar. Clinical trials had already established that the use of injectable artesunate results in reduced mortality and shortened hospital stays, as this leads to faster elimination of parasites [32,33].
The case fatality rate was slightly lower in patients taking artesunate in 2020 compared to those treated with quinine or artemether in 2016. This rate of 5% in 2020 is lower than the results of other previous studies carried out in Senegal by Diop [10], Lawson [34] and Cisse [17] who found 17.1% and 18% and 10.9% respectively. This trend observed in our study is clearly in line with current WHO data, which shows a reduction in case fatality in recent years, from 896,000 cases in 2000 to 558,000 cases in 2019 [4].
In Senegal, the number of deaths fell from 526 to 260, a reduction of 51% over the period from 2016 to 2019 [8]. In addition, injectable artesunate, the currently first-line treatment for severe malaria, was the only antimalarial used in all patients included in 2020. Clinical trials had already established that the use of injectable artesunate reduced mortality and shortened hospital stays, as it led to faster elimination of parasites [32,33].
We also looked for risk factors for death: in 2016, the factors significantly associated with death were coma (p: 0.000), hepatomegaly (p: 0.03) and diffuse hemorrhage (p: 0.03). In 2020. Death was significantly associated with coma (p: 0.000) and the occurrence of respiratory failure (p: 0.000).
Disorders of consciousness, particularly coma, have been found as a factor independently associated with death in several studies [17, 35,36]. In Brunel's study [20], 21% of surviving patients had impaired consciousness, compared to 62% of deceased patients, with a statistically significant difference. The severity of cerebral malaria is linked to the sequestration of red blood cells, leading to vital dysfunction, which is mainly the prerogative of Plasmodium falciparum.
Conclusion
Serious malaria remains a public health problem in Senegal, especially in the South-Eastern regions, which are characterized by a persistence of serious forms of malaria, especially in children, with a predominance of neurological signs of severity. Access to RDT has improved early diagnosis and the use of injectable artesunate has helped reduce mortality. Optimizing early diagnosis of signs of malaria severity and strengthening the technical platform in intensive care units, as well as increasing preventive efforts, can improve outcomes for patients.
Table 1: Socio-demographic characteristics of severe malaria among patients Velingara's two health centers in 2016 and 2020.
|
Variables |
Année 2016 (N=357) |
Année 2020 (N=456) |
P-value |
|
Gender |
|
|
|
|
Female |
178 (49.86) |
221 (48.46) |
0.693 |
|
Male |
179 (50.14) |
235 (51.54) |
|
|
Age (years) |
|
|
|
|
0 - 5 |
121 (33.89) |
107 (23.46) |
0.001 |
|
6 - 15 |
139 (38.94) |
212 (46.49) |
0.031 |
|
16 - 50 |
77 (38.94) |
115 (38.94) |
0.224 |
|
>50 |
69 (21.57) |
93 (25.22) |
0.619 |
|
Mean age |
14.86±16.72 |
15.38±15.36 |
0.643 |
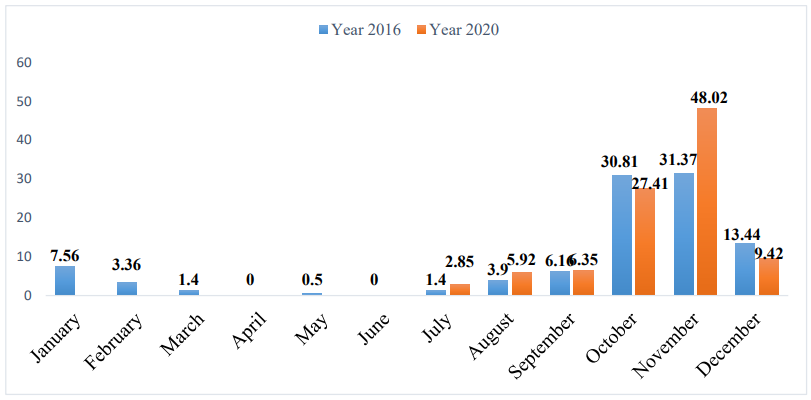
Figure 1: Patients’ received for severe malaria based on different months in Velingara’s two health centers in 2016 and 2020.
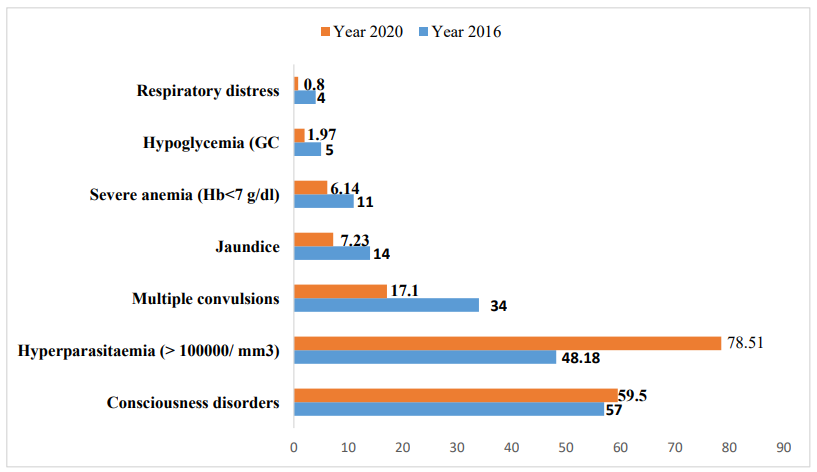
Figure 2: Table 2. Clinical and biological manifestations of severe malaria Vélingara’s two health centers in 2016 and 2020.
Table 2: Clinical manifestations of severe malaria Vélingara’s two health centers in 2016 and 2020.
|
Signes cliniques |
Year 2016 |
Year 2020 |
|
Fever |
351 (98.32) |
393 (86,18) |
|
Vomiting |
131(36.69) |
213 (46,71) |
|
Headach |
13 (3.64) |
107 (23,46) |
|
Algie diffuse |
16 (4.48) |
56 (12,28) |
|
Diarrhée |
17 (4,76) |
37 (8,11) |
|
Saignement anormal |
8 (2,2) |
0 (0,00) |
Table 3: Repartion of patients based on therapeutic and evolving aspects in Vélingara’s two health centers in 2016 and 2020.
|
Aspects thérapeutiques |
Year 2016 |
Year 2020 |
p-value |
|
Artesunate inj |
0 (0,00) |
456 (100) |
|
|
Quinine inj |
347 (97.20) |
0 (0,00) |
|
|
Artheméter in |
10 (2.80) |
0 (0,00) |
|
|
Hospitalization length (days) |
|
|
|
|
Mean |
3.22 ± 1.99 |
1.59 ± 0.78 |
0.0000 |
|
< 4 |
257 (72.19) |
445 (97.59) |
|
|
4- 7 |
85 (23.88) |
11 (2.41) |
|
|
> 7 |
14 (3.93 ) |
0 (0,00) |
|
|
Evolution |
|
|
|
|
Healing |
324 (91) |
433 (95) |
|
|
Deaths |
19 (05) |
16 (3,5) |
|
|
Transfert |
14 (04) |
07 (1,54) |
|
Table 4: Repartition of death cases due to severe malaria based on age, sex, severity signs.
|
Variables |
Death |
|
|
Year |
2016 |
2020 |
|
Sex |
|
|
|
Male |
6 (3.35) |
13 (5.53) |
|
Female |
13 (7.30) |
10 (4.52) |
|
Age range (years) |
|
|
|
0-5 |
9 (7.44) |
9 (8.41) |
|
6-15 |
7 (5.04) |
13 (6.13) |
|
15-50 |
2 (2.60) |
0 (0,00) |
|
> 50 |
1 (5.00) |
1 (4.55) |
|
|
19 (5.32) |
23 (5.04) |
|
Gravity symptoms |
|
|
|
Coma |
9/189 (4,76) |
5/14 (35,71) |
|
Multiples convulsions |
8/128 (6.25) |
8/78 (10.26) |
|
Jaundice |
4/54 (7.41) |
1/38 (2.56) |
|
Hyperparasitaemia (> 100000/ mm3 |
13/172 (7.56) |
20/358 (5.59) |
Table 5: Risk factors for death of severe malaria Vélingara’s two health centers in 2016 and 2020.
|
Année |
Variables |
OR |
p-value |
IC 95% |
|
2016 |
Consciousness disorders |
15,35 |
0,000 |
[3,74 –62,89 |
|
|
Respiratory distress |
15,10 |
0,031 |
[1,27 - 179] |
|
2020 |
Consciousness disorders |
13,5 |
0,00 |
[5,6 – 35] |
References
- National Agency for Statistics and Demography (ANSD) [Senegal], and ICF. 2021. Survey on malaria indicators in Senegal, 2020-2021: 155.
- Barry, M. (2012). L’efficacité des nouvelles innovations insti-tutionnelles: la coordination impulsée par Roll Back Malaria (RBM). Le cas du Sénégal. Journal de gestion et d’économie médicales, 30(3), 151-174.
- Republic of Senegal, Ministry of Health and Social Action. (2016). National malaria control program. NATIONAL GUIDE to the biological diagnosis of Malaria.
- World Health Organization .(2021). World Malaria Report.
- Dondorp, A. (2005). South East Asian Quinine Artesunate Malaria Trial (SEAQUAMAT) group: Artesunate versus quinine for treatment of severe falciparum malaria: A randomized trial. Lancet, 366, 717-725.
- Dondorp, A. M., Fanello, C. I., Hendriksen, I. C., Gomes, E.,Seni, A., Chhaganlal, K. D., ... & White, N. J. (2010). Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial. The Lancet, 376(9753), 1647-1657.
- Global Fund. Senegal Funding Request 2020–22
- National Malaria Control Program (NLP), National Malaria Control Strategic Plan in Senegal 2021-2025
- World Health Organization. (2015). Guidelines for the treatment of malaria. World Health Organization.
- Diop, S. A., Ndour, C. T., SOW, P., DIA, N., MANGA, N., &FORTES, L. (2010). Aspects actuels du paludisme grave de l'adulte à la clinipue des maladies infectieuses du CHNU de Fann de Dakar (Sénégal). Médecine d'Afrique noire, 57(4), 193-197.
- Wade, K. A., Sene, B. E. J., Niang, E. M., Diallo, A., & Di-atta, B. (2012). Epidemiology and prognostic value of organ failure during severe malaria in the Principal Military Teaching Hospital of Dakar, Senegal. Médecine et Santé Tropicales, 22(4), 422-424.
- Eholie, S. P., Ehui, E., Adou-Bryn, K., Kouame, K. E., Tanon, A., Kakou, A., ... & Kadio, A. (2004). Severe malaria in native adults in Abidjan (Côte d'Ivoire). Bulletin de la Societe de Pathologie Exotique (1990), 97(5), 340-344.
- Mbama Ntabi, J. D., Lissom, A., Djontu, J. C., Diafouka-Ki-etela, S., Vouvoungui, C., Boumpoutou, R. K., ... & Ntoumi,F. (2022). Prevalence of non-Plasmodium falciparum species in southern districts of Brazzaville in The Republic of the Congo. Parasites & vectors, 15(1), 209.
- Soumare, M., Seydi, M., Diop, S. A., Ba, T. A., Ndour, C. T., Dieng, Y., ... & Sow, P. S. (2008). The place of malaria in an infectious disease department in Dakar, Senegal. Medecine Tropicale: Revue du Corps de Sante Colonial, 68(5), 485-490.
- Appawu, M., Owusu-Agyei, S., Dadzie, S., Asoala, V., Anto, F., Koram, K., ... & Fryauff, D. J. (2004). Malaria transmission dynamics at a site in northern Ghana proposed for testing malaria vaccines. Tropical Medicine & International Health, 9(1), 164-170.
- Traoré, Y. (2022). Etude épidémiologique clinique et bi-ologique du paludisme grave et compliqué chez les enfants de 0 à 14 ans après la mise à échelle de la chimio-prévention du paludisme saisonnier dans le district sanitaire de la commune I de Bamako (Doctoral dissertation, USTTB).
- Cisse, V. M. P., Mbaye, K. D., Badiane, A. S., Diallo, M., Diop, M., Lakhe, N. A., ... & Seydi, M. (2023). Severe Malaria and Risk Factors for Death in the Infectious Diseases Department of the University Hospital of Fann in Dakar, Senegal. Asian Journal of Research in Infectious Diseases, 14(4), 86-93.
- Agbeille, M. F., Adedemy, J. D., Noudamadjo, A., Kpanidja, Mbanga-Ngoume J. J., J. Agossou. (2019). Neuropaludisme de l’enfant au Centre Hospitalier Universitaire Départemental du Borgou, Bénin. Médecine d'Afrique Noire 6603, 131-138
- Moyen, G., Mbika Cardorelle, A., Kambourou, J., Oko, A., & Mouko, A. (2010). Paludisme grave de l'enfant à Brazzaville. Médecine d'Afrique noire, 57(2), 113-116.
- SYLLA, K., MBAYE, K. D., JABER, C., MASSALY, A., DI-ALLO, V. M. P. C., Daye, K. A., ... & Moussa, S. E. Y. D.(2018). Current Aspect of Severe Malaria at the Infectious and Tropical Disease Service in Fann (Dakar). Archives of Infectious Diseases & Therapy, 2(2), 1-7.
- Cook, G., & Zumla, A. (2003). Manson’s Tropical Diseases, 21s1 Edition. Saunders, London, 995-1036.
- Shukia, M. M., Singh, N., Singh, M. P., Tejwani, B. M., Srivastava, D. K., & Sharma, V. P. (1995). Cerebral malaria in Jabalpur. Ind J Malarialogy, 32, 70-5.
- Soumare, M., Seydi, M., Diop, S. A., Diop, B. M., & Sow, P.S. (2008). Cerebral malaria in adults at the Infectious Diseases Clinic in the Fann Hospital in Dakar, Senegal. Bulletin de la Societe de Pathologie Exotique (1990), 101(1), 20-21.
- Moyen, G., Mbika Cardorelle, A., Kambourou, J., Oko, A., & Mouko, A. (2010). Paludisme grave de l'enfant à Brazzaville. Médecine d'Afrique noire, 57(2), 113-116.
- Camara, B., Diagne, N. R., Faye, P. M., Fall, M. L., Ndiaye, J. L., Ba, M., & Sow, H. D. (2011). Critères de gravité et facteurs pronostiques du paludisme chez l’enfant à Dakar. Médecine et maladies infectieuses, 41(2), 63-67.
- Berger, J., & Dillon, J. C. (2002). Stratégies de contrôle de la carence en fer dans les pays en développement. Sante, 12(1), 22-30.
- Rustin L. (2021). Criteria predictive of recourse to surrogacy treatmentsrgane in intensive care in severe forms of malaria. Life Sciences.
- Camara, B., Diagne, N. R., Faye, P. M., Fall, M. L., Ndiaye, J. L., Ba, M., & Sow, H. D. (2011). Critères de gravité et facteurs pronostiques du paludisme chez l’enfant à Dakar. Médecine et maladies infectieuses, 41(2), 63-67.
- CAMARA, E., BARRY, I. K., DIALLO, M. L., DIOP, M.,ONDIMA, H. M., & DIALLO, B. (2019). Corrélation entre densité parasitaire et taux d’hémoglobine au cours du paludisme grave chez les enfants de 0-5 ans à) Conakry en 2018/ Correlation between Parasitic Density and Hemoglobin levels during severe Malaria in Children aged 0-5 years old in Conakry In 2018.
- Kotepui, M., Piwkham, D., PhunPhuech, B., Phiwklam, N.,Chupeerach, C., & Duangmano, S. (2015). Effects of malaria parasite density on blood cell parameters. PloS one, 10(3), e0121057.
- Padilla-Rodríguez, J. C., Olivera, M. J., & Guevara-García,B. D. (2020). Parasite density in severe malaria in Colombia.PLoS One, 15(6), e0235119.
- Artemether-Quinine Meta-analysis Study Group. (2001). A meta-analysis using individual patient data of trials comparing artemether with quinine in the treatment of severe falciparum malaria. Transactions of the Royal Society of Tropical Medicine and Hygiene, 95(6), 637-650.
- Phu, N. H., Tuan, P. Q., Day, N., Mai, N. T., Chau, T. T.,Chuong, L. V., ... & Hien, T. T. (2010). Randomized controlled trial of artesunate or artemether in Vietnamese adults with severe falciparum malaria. Malaria journal, 9, 1-10.
- Déla-dem Lawson, A. T., Diop, M. M., Cisse, V. M. P., Akan-ni, S., Berthe, A., Toure, P. S., ... & Ka, M. M. (2018). The Epidemiological, Clinical, Paraclinical and Prognostic Aspects of Severe Malaria at the Regional Hospital of Thies. Advances in Infectious Diseases, 8(03), 162.
- Bruneel, F., Tubach, F., Corne, P., Megarbane, B., Mira, J. P., Peytel, E., ... & Severe Imported Malaria in Adults (SIMA) Study Group. (2010). Severe imported falciparum malaria: a cohort study in 400 critically ill adults. PloS one, 5(10), e13236.
- Mengistu, G., & Diro, E. (2006). Treatment outcome of severe malaria in adults with emphasis on neurological manifestations at Gondar University Hospital, north west Ethiopia. Ethiopian Journal of health development, 20(2), 106-111.