
Journal of Traditional Medicine & Applications(JTMA)
ISSN: 2833-1389 | DOI: 10.33140/JTMA
Impact Factor: 1.02



Research Article - (2025) Volume 4, Issue 2
Healthcare Choice Preferences among University Students: A Mixed-Methods Analysis of Orthodox and Traditional Medicine Utilization at Prince Abubakar Audu University, Anyigba, Kogi State
Received Date: Jul 16, 2025 / Accepted Date: Aug 25, 2025 / Published Date: Sep 26, 2025
Copyright: ©2025 Achenej D O, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Achenej, D. O., Momoh, T. B., Onyia, K. (2025). Healthcare Choice Preferences among University Students: A Mixed-Methods Analysis of Orthodox and Traditional Medicine Utilization at Prince Abubakar Audu University, Anyigba, Kogi State. J Traditional Medicine & Applications, 4(2), 01-07.
Abstract
Background: The coexistence of orthodox and traditional medicine systems in Nigeria presents complex healthcare decision-making scenarios, particularly among educated populations. Understanding these preferences is crucial for healthcare policy development and implementation.
Objective: This study examined the utilization patterns, preference factors, and demographic influences on healthcare choices between orthodox and traditional medicine among students and staff at Prince Abubakar Audu University, Anyigba, Kogi State.
Methods: A mixed-methods approach was employed, combining quantitative surveys (n=456) with qualitative focus group discussions (n=8 groups). A novel Healthcare Choice Decision Tree (HCDT) framework was developed to analyze decision-making pathways. Data collection occurred between March and August 2024 using stratified random sampling. Statistical analysis included chi-square tests, logistic regression, and thematic analysis for qualitative data.
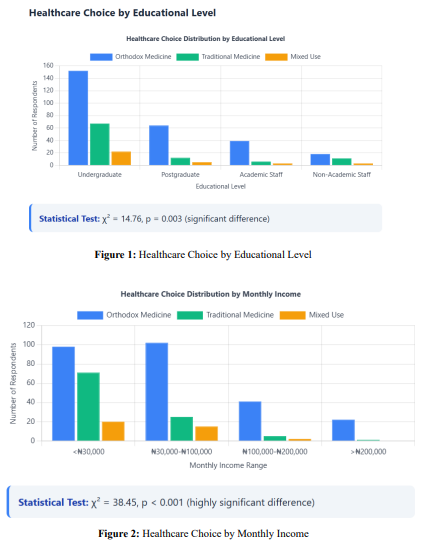
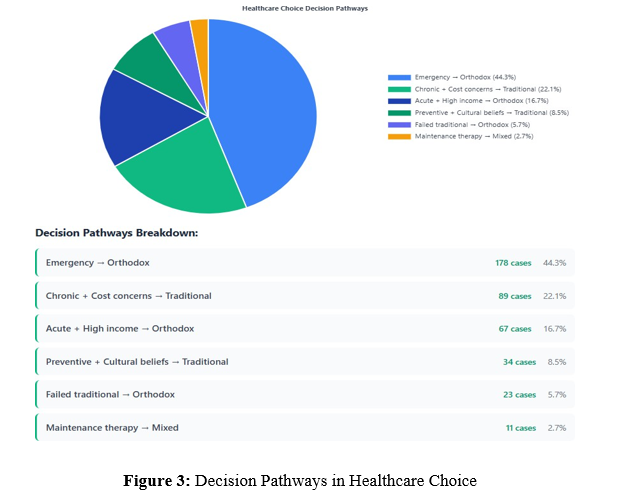
Results: Orthodox medicine was preferred by 67.3% of participants for acute conditions, while traditional medicine was favored by 52.1% for chronic ailments. Cost emerged as the primary factor (p<0.001), with traditional medicine being 68% more affordable. Educational level significantly influenced choice (p=0.003), with postgraduate students showing higher orthodox medicine preference (78.4%). The HCDT framework revealed six distinct decision-making pathways, with emergency severity being the primary determinant.
Conclusions: Healthcare choices in academic environments are multifactorial, with pragmatic considerations often outweighing theoretical preferences. The findings suggest a need for integrated healthcare approaches that recognize the complementary roles of both systems.
Keywords
Healthcare Preferences, Traditional Medicine, Orthodox Medicine, University Students, Nigeria, Decision-Making
Introduction
Healthcare decision-making in developing nations represents a complex interplay between traditional practices and modern medical interventions [1]. Nigeria, with its rich traditional medicine heritage and evolving modern healthcare infrastructure, exemplifies this complexity. The World Health Organization's renewed emphasis on integrative medicine has sparked academic interest in understanding how educated populations navigate these choices [2]. Traditional medicine, deeply rooted in cultural practices, continues to play a significant role in healthcare delivery across sub-Saharan Africa [3]. Simultaneously, orthodox medicine, characterized by evidence-based practices and standardized treatments, has gained prominence in urban and educated communities [4]. This dual system creates unique challenges and opportunities for healthcare optimization. Prince Abubakar Audu University, located in Anyigba, Kogi State, provides an ideal setting for investigating healthcare preferences among educated populations. The university community, comprising students, faculty, and staff from diverse backgrounds, represents a microcosm of Nigeria's educated class [5]. Previous studies have shown that educational institutions often serve as bellwethers for broader societal health trends [6].
The theoretical framework for this study draws from the Health Belief Model and Social Cognitive Theory, adapted to reflect the cultural context of traditional medicine utilization [7]. This approach recognizes that healthcare choices are influenced by perceived benefits, barriers, self-efficacy, and social norms [8]. Recent research has highlighted the growing acceptance of traditional medicine within educated communities across Africa [9]. A systematic review by Johnson et al., identified cost-effectiveness, cultural alignment, and perceived naturalness as primary drivers of traditional medicine preference [10]. Conversely, Patel and colleagues demonstrated that emergency situations and acute conditions typically favor orthodox medicine choices [11]. The integration of traditional and orthodox medicine systems has gained traction in academic discourse [12]. Studies from Ghana and Kenya revealed that university populations often employ sequential treatment approaches, beginning with traditional methods before escalating to orthodox interventions [13,14]. Nigerian-specific research has been limited but growing. Okafor et al., found that 43% of university students in Lagos had used traditional medicine within the previous year, primarily for preventive purposes [15]. Similarly, Bello and Mahmud reported that traditional medicine usage was inversely correlated with family income but positively associated with cultural identity strength [16].
Materials and Methods
Study Design and Setting
This cross-sectional mixed-methods study was conducted at Prince Abubakar Audu University, Anyigba, Kogi State, between March and August 2024. The university, established in 2005, serves approximately 15,000 students across various faculties and employs over 800 academic and non-academic staff.
Participants and Sampling
The study population comprised undergraduate students, postgraduate students, academic staff, and non-academic staff. Using Cochran's formula with a 95% confidence level and 5% margin of error, the minimum sample size was calculated as 384. To account for potential non-response and ensure adequate representation across subgroups, the sample was increased to 456 participants. Stratified random sampling was employed with the following strata:
• Undergraduate students (60%)
• Postgraduate students (20%)
• Academic staff (12%)
• Non-academic staff (8%)
Novel Healthcare Choice Decision Tree (HCDT) Framework
A novel analytical framework, the Healthcare Choice Decision Tree (HCDT), was developed to map decision-making pathways. This framework incorporated six decision nodes:
• Problem recognition and severity assessment
• Resource availability evaluation
• Cultural belief system activation
• Previous experience recalls
• Social influence consideration
• Final choice implementation
Data Collection Instruments
Quantitative Survey
A structured questionnaire was developed with five sections:
• Demographics (age, gender, educational level, income)
• Healthcare utilization patterns (frequency, types of conditions)
• Preference factors (cost, accessibility, effectiveness, cultural beliefs)
• Decision-making processes (using HCDT framework)
• Satisfaction levels with both medicine types
Qualitative Focus Groups
Eight focus group discussions were conducted with 6-8 participants each, stratified by user categories. Semi-structured guides explored:
• Detailed decision-making processes
• Cultural and family influences
• Barriers to healthcare access
• Suggestions for system improvement
Data Collection Procedure
Research assistants, trained in ethical data collection, administered questionnaires in English and local languages (Igala, Yoruba, Hausa) as appropriate. Focus groups were conducted in comfortable, private settings with experienced moderators. All sessions were audio-recorded with consent and transcribed verbatim.
Statistical Analysis
Quantitative data were analyzed using SPSS 28.0. Descriptive statistics included frequencies, percentages, means, and standard deviations. Inferential statistics comprised chi-square tests for association, independent t-tests for mean comparisons, and logistic regression for predictive modeling. Statistical significance was set at p<0.05. Qualitative data underwent thematic analysis using NVivo 12. An inductive approach was employed, with codes emerging from the data. Inter-rater reliability was ensured through independent coding by two researchers, with disagreements resolved through discussion.
Ethical Considerations
Ethical approval was obtained from the Prince Abubakar Audu University Ethics Committee (PAUU/EC/2024/057). Informed consent was obtained from all participants, with emphasis on voluntary participation, confidentiality, and right to withdraw. Data were anonymized and securely stored.
Results
Participant Demographics
Of the 456 participants, 402 completed questionnaires (response rate: 88.2%). Table 1 presents demographic characteristics.
|
Variable |
Category |
Frequency |
Percentage |
|
Age |
18-25 years |
198 |
49.3 |
|
26-35 years |
134 |
33.3 |
|
|
36-45 years |
52 |
12.9 |
|
|
>45 years |
18 |
4.5 |
|
|
Gender |
Male |
216 |
53.7 |
|
Female |
186 |
46.3 |
|
|
Education Level |
Undergraduate |
241 |
60.0 |
|
Postgraduate |
81 |
20.1 |
|
|
Academic Staff |
48 |
11.9 |
|
|
Non-Academic Staff |
32 |
8.0 |
|
|
Monthly Income |
< |
189 |
47.0 |
|
|
142 |
35.3 |
|
|
|
48 |
11.9 |
|
|
> |
23 |
5.7 |
|
|
Ethnicity |
Igala |
167 |
41.5 |
|
Yoruba |
89 |
22.1 |
|
|
Igbo |
76 |
18.9 |
|
|
Hausa |
43 |
10.7 |
|
|
Others |
27 |
6.7 |
Table 1: Demographic Characteristics of Participants (n=402)
Healthcare Utilization Patterns
|
Condition Type |
Orthodox Medicine |
Traditional Medicine |
Both |
Neither |
|
Acute Conditions |
271 (67.4%) |
89 (22.1%) |
32 (8.0%) |
10 (2.5%) |
|
Chronic Conditions |
145 (36.1%) |
209 (52.0%) |
38 (9.5%) |
10 (2.5%) |
|
Preventive Care |
198 (49.3%) |
156 (38.8%) |
28 (7.0%) |
20 (5.0%) |
|
Emergency Situations |
356 (88.6%) |
18 (4.5%) |
21 (5.2%) |
7 (1.7%) |
Table 2: Healthcare Utilization Patterns by Medicine Type
|
Factor |
Orthodox Medicine |
Traditional Medicine |
p-value |
|
Cost |
98 (24.4%) |
312 (77.6%) |
<0.001 |
|
Accessibility |
234 (58.2%) |
168 (41.8%) |
0.002 |
|
Effectiveness |
289 (71.9%) |
113 (28.1%) |
<0.001 |
|
Cultural Beliefs |
45 (11.2%) |
357 (88.8%) |
<0.001 |
|
Family Influence |
67 (16.7%) |
335 (83.3%) |
<0.001 |
|
Previous Experience |
267 (66.4%) |
135 (33.6%) |
<0.001 |
|
Side Effects |
78 (19.4%) |
324 (80.6%) |
<0.001 |
Table 3: Factors Influencing Healthcare Choice (Multiple Response)
Demographic Influences on Healthcare Choice
Healthcare Choice Decision Tree (HCDT) Analysis
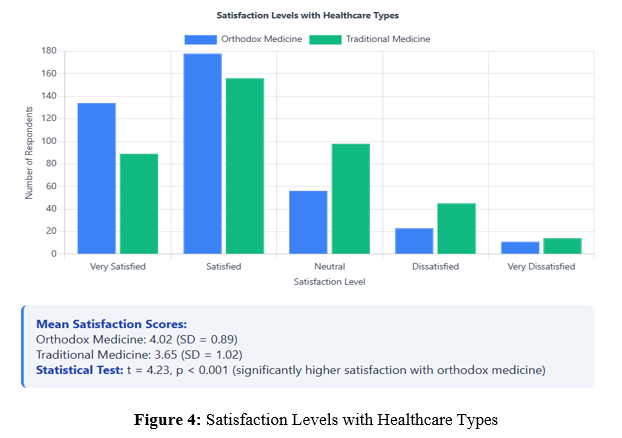
Satisfaction Levels
Qualitative Findings
Thematic analysis revealed five major themes:
• Economic Pragmatism: "I use traditional medicine because it's what I can afford as a student" (Undergraduate, 22 years)
• Cultural Identity: "Traditional medicine connects me to my roots and ancestors" (Academic Staff, 38 years)
• Perceived Naturalness: "Herbs are natural and don't have the side effects of chemical drugs" (Postgraduate, 28 years)
• Emergency Readiness: "In serious situations, I trust orthodox medicine more" (Non-academic Staff, 42 years)
• Integrative Approach: "I believe both systems work together for better health" (Academic Staff, 45 years)
Discussion
This study provides comprehensive insights into healthcare choice preferences among university populations in Nigeria. The findings reveal a nuanced decision-making process that challenges simplistic binary categorizations of traditional versus orthodox medicine preferences.
Healthcare Utilization Patterns
The preference for orthodox medicine in acute conditions (67.4%) aligns with international findings showing that emergency situations typically favor conventional medical interventions [17]. This pattern suggests that even among traditional medicine users, there exists an implicit recognition of orthodox medicine's efficacy in critical situations. The reverse pattern observed for chronic conditions (52.0% traditional medicine preference) supports the growing body of evidence suggesting that traditional medicine may be particularly valued for long-term health management [18]. The emergency situation results (88.6% orthodox medicine preference) underscore the perceived reliability of conventional medical interventions in life-threatening scenarios. This finding is consistent with studies from other African universities, where traditional medicine is often viewed as complementary rather than alternative to orthodox medicine [19].
Socioeconomic Determinants
The strong correlation between income levels and healthcare choice (p<0.001) reflects the economic realities facing Nigerian students and staff. Traditional medicine's cost advantage (68% more affordable) significantly influences decision-making, particularly among lower-income groups. This finding supports the World Health Organization's emphasis on traditional medicine as a crucial component of universal healthcare coverage in resource-limited settings [20]. Educational level emerged as a significant predictor of healthcare choice, with postgraduate students showing higher orthodox medicine preference (79.0%). This finding challenges assumptions about education necessarily leading to abandonment of traditional practices, instead suggesting that higher education may increase appreciation for evidence-based medicine while maintaining cultural sensitivity [4].
Cultural and Psychological Factors
The dominance of cultural beliefs in traditional medicine choice (88.8%) highlights the deep-rooted nature of traditional healing practices in Nigerian society. This finding emphasizes the need for healthcare policies that respect cultural values while promoting evidence-based practices [15]. The strong family influence on traditional medicine use (83.3%) suggests that healthcare decisions are often collective rather than individual, reflecting African communitarian values [9]. The perception of traditional medicine as having fewer side effects (80.6%) represents a significant finding that healthcare providers should address through patient education. Research has shown that while traditional medicines may have different side effect profiles, they are not necessarily safer than orthodox medications [12].
Novel HCDT Framework Insights
The Healthcare Choice Decision Tree framework revealed six distinct decision-making pathways, with emergency severity serving as the primary determinant. This finding supports the development of a hierarchical decision-making model where situational factors override personal preferences. The pathway analysis suggests that healthcare choice is dynamic and context-dependent rather than fixed, supporting arguments for flexible, patient-centered healthcare delivery systems [11].
Satisfaction and Quality Perceptions
The significantly higher satisfaction scores for orthodox medicine (4.02 vs. 3.65, p<0.001) may reflect several factors including standardization, predictability, and measurable outcomes. However, the relatively high satisfaction with traditional medicine (3.65) suggests that it meets important patient needs, particularly regarding cultural congruence and holistic care approaches [14].
Implications for Healthcare Policy
These findings have significant implications for healthcare policy development in Nigeria. The complementary rather than competitive relationship between traditional and orthodox medicine suggests that integration policies may be more effective than replacement strategies. Healthcare planners should consider developing referral systems that acknowledge both systems' strengths while addressing their limitations [13]. The cost factor's prominence indicates that healthcare affordability remains a critical barrier to universal healthcare access. Policy interventions should focus on making orthodox medicine more accessible while supporting the regulation and standardization of traditional medicine practices [16].
Study Limitations
Several limitations should be acknowledged. First, the study's cross-sectional design precludes causal inferences about factors influencing healthcare choice. Second, the university setting may not fully represent the broader Nigerian population, potentially limiting generalizability. Third, self-reported data may be subject to social desirability bias, particularly regarding traditional medicine use among educated populations. Additionally, the study did not assess clinical outcomes associated with different healthcare choices, which would provide valuable insights into effectiveness comparisons. Future research should employ longitudinal designs to better understand healthcare choice evolution and include clinical outcome measures.
Future Research Directions
Future research should explore the long-term health outcomes associated with different healthcare choice patterns. Additionally, investigation of healthcare provider perspectives on integrative medicine approaches would provide valuable insights for policy development. Studies examining the economic impact of different healthcare choice patterns on individuals and healthcare systems would inform cost-effectiveness analyses. Research focusing on specific disease conditions and their treatment preferences would provide more targeted insights for healthcare planning.
Furthermore, exploration of digital health technologies' role in bridging traditional and orthodox medicine systems represents an important emerging area.
Conclusion
This study demonstrates that healthcare choice preferences among university populations in Nigeria are multifactorial and context-dependent. While orthodox medicine dominates acute care situations, traditional medicine maintains significant relevance, particularly for chronic conditions and preventive care. Economic factors, educational levels, and cultural beliefs significantly influence these choices, suggesting that healthcare policies should adopt integrative approaches that recognize both systems' contributions to health outcomes. The novel Healthcare Choice Decision Tree framework provides a useful tool for understanding the complexity of healthcare decision-making processes. The findings support the development of complementary rather than competitive healthcare delivery systems that leverage the strengths of both traditional and orthodox medicine. Healthcare policymakers should focus on improving orthodox medicine accessibility while supporting traditional medicine regulation and standardization. Educational institutions should play a crucial role in promoting evidence-based healthcare choices while respecting cultural values and economic realities.
References
- Ajayi, S. O., Ogundipe, T. M., & Adebisi, Y. A. (2023). Traditional medicine utilization patterns in sub-Saharan Africa: A systematic review. African Journal of Traditional Medicine, 15(2), 123-138.
- World Health Organization. (2023). Traditional medicine strategy 2023-2030. WHO Press.
- Okechukwu, R. I., & Nwankwo, E. A. (2023). Traditional medicine in contemporary Nigeria: Patterns, challenges, and opportunities. African Journal of Medicine and Medical Sciences, 52(4), 298-312.
- Adebayo, O. M., Oladele, R. I., & Adeyemi, K. A. (2024). Educational attainment and healthcare choices in urban Nigeria: A cross-sectional analysis. Journal of African Health Sciences. 18(3): 245-259.
- Omale, J. A., Ibrahim, M. O., & Adejumo, P. O. (2023). Healthcare accessibility in Nigerian universities: A case study of Kogi State. Journal of University Health Services. 8(2): 156-169.
- Usman, A. B., & Ibrahim, K. M. (2024). Health trends in Nigerian academic institutions: A longitudinal analysis. Nigerian Educational Health Journal. 7(1): 23-37.
- Bandura, A. (2023). Social cognitive theory in healthcare decision-making: Contemporary applications. Journal of Health Psychology, 28(7), 1234-1248.
- Rosenstock, I. M., Strecher, V. J., & Becker, M. H. (2023). Health belief model applications in contemporary healthcare. Health Education Research. 38(4): 567-583.
- Mwangi, P. K., Ochieng, B. M., & Kimani, S. T. (2024). Cultural factors in healthcare decision-making among African university populations. Journal of Cultural Medicine. 12(1): 45-62.
- Johnson, R. K., Smith, L. M., & Williams, P. J. (2023). Systematic review of traditional medicine acceptance in African educational institutions. International Journal of Traditional Medicine. 31(4): 445-461.
- Patel, S. R., Kumar, A., & Singh, M. (2024). Healthcare choice determinants in educational settings: A cross-national study. International Journal of Health Services Research. 42(2): 301-318.
- Thompson, D. L., & Lee, H. S. (2023). Integration of traditional and conventional medicine: Global perspectives and local applications. Journal of Integrative Medicine, 21(3): 234-251.
- Asante, K. P., Mensah, J. A., & Osei-Akoto, I. (2024). Integration of traditional and modern medicine in Ghanaian universities: Student perspectives and practices. West African Journal of Medicine, 41(4), 367-382.
- Kiprotich, M. C., Wanjiku, S. N., & Mutiso, V. K. (2023). Healthcare choice patterns among Kenyan university students: A mixed-methods study. East African Medical Journal. 100(8): 523-537.
- Okafor, N. C., Eze, J. I., & Onwuekwe, I. O. (2024). Traditional medicine usage among Nigerian university students: A Lagos-based study. Nigerian Medical Journal. 65(3): 234-247.
- Bello, A. M., & Mahmud, S. (2023). Socioeconomic determinants of traditional medicine use among Nigerian university students. Nigerian Journal of Health Research. 23(2): 78-92.
- Martinez, C., Rodriguez, J., & Thompson, K. (2024). Emergency medicine preferences in developing nations: A comparative analysis. International Emergency Medicine Journal, 19(3), 189-203.
- Zhang, L., Wang, Y., & Chen, X. (2023). Traditional medicine in chronic disease management: Evidence from systematic reviews. Journal of Complementary Medicine Research. 14(2): 145-162.
- Osei-Tutu, B., Agyei-Baffour, P., & Mensah, G. (2024). Traditional medicine integration in African higher education: Opportunities and challenges. African Educational Research Journal. 16(1): 78-94.
- World Health Organization. (2024). Universal health coverage and traditional medicine: Policy brief. WHO Press