
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2025) Volume 10, Issue 2
Gendered Barriers to Health and Nutrition Resilience among Female-Headed Households in Conflict-Affected Darfur: Evidence from a Mixed-Methods Study
Received Date: Jul 21, 2025 / Accepted Date: Jun 08, 2025 / Published Date: Aug 11, 2025
Copyright: ©2025 Md. Abu Hanif. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Hanif, A. Md. (2025). Gendered Barriers to Health and Nutrition Resilience Among Female-Headed Households in Conflict-Affected Darfur: Evidence from a Mixed-Methods Study, Int J Womenâ??s Health Care, 10(2), 01-10.
Abstract
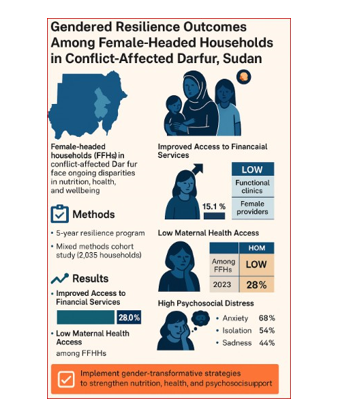
Female-headed households (FHHs) in conflict-affected Darfur, Sudan, face intersecting vulnerabilities across food security, health access, psychosocial wellbeing, and community participation. This study assesses the impact of a five-year humanitarian program Resilience Towards Development (2018–2023) using a longitudinal mixed-methods approach. Quantitative data from 2,035 households and qualitative insights from 36 focus group discussions, 20 key informant interviews, and 5 participatory rural appraisals were analyzed. Indicators included household hunger, child dietary diversity, maternal health access, and resilience capacity, disaggregated by gender and household type. Findings show significant improvement in financial access among FHHs (15.1% to 28.0%, p < 0.01), but deterioration in key health and nutrition indicators. Child dietary diversity declined from 12.8% to 6.8%, and acute hunger rose sharply from 4.1% to 22.6% among FHHs (p < 0.01). Psychosocial distress remained high, and only 9.8% of health governance committee members were women. Gains in absorptive resilience were modest, while adaptive and transformative capacities stagnated. These outcomes expose the limitations of gender-neutral programming in fragile settings. The study calls for gender-transformative strategies that prioritize FHHs through inclusive service design, targeted nutrition and mental health support, and women-led governance models. Lessons from Darfur offer transferable insights for humanitarian responses in conflict-affected regions across Eastern Africa.
Keywords
Female-Headed Households (FHHs), Gender-Responsive Resilience, Maternal Health, Nutrition Insecurity, Conflict- Affected Sudan, Psychosocial Wellbeing, Humanitarian Programming, Mixed-Methods Evaluation
Introduction
Background and Problem Statement
The Darfur region of Sudan remains one of the most complex and protracted humanitarian crises in the world, shaped by decades of armed conflict, mass displacement, and structural state fragility. These overlapping shocks have had disproportionately adverse effects on female-headed households (FHHs) a demographic that has grown significantly due to widowhood, separation, and male migration, but remains under-served in humanitarian response systems. Across Sudan, FHHs consistently report higher rates of food insecurity, poorer health access, and lower psychosocial wellbeing compared to male-headed households [1-3]. In Darfur specifically, recent data show FHHs were nearly 11 percentage points more likely to experience food insecurity and scored lowest in child dietary diversity, access to maternal healthcare, and resilience capacity [2]. These disparities are not incidental but are structurally driven rooted in unequal access to land, financial exclusion, limited mobility, and low representation in community governance systems [4,5]. While women are increasingly responsible for caregiving, income generation, and household decision-making, the humanitarian system continues to apply gender-neutral frameworks that fail to recognize the unique vulnerabilities and capacities of female-headed households [6].
Justification for the Study
Despite growing recognition of the gendered dimensions of health and nutrition vulnerability, there remains a significant gap in evidence-based, gender-disaggregated research focused on conflict-affected regions such as Darfur. Existing programming often lacks precision targeting and fails to differentiate needs across household types, leading to critical blind spots in the design of humanitarian resilience strategies [5,7]. Moreover, while global frameworks such as the Sphere Standards and Gender-Based Analysis Plus (GBA+) promote inclusive programming, their practical application in fragile zones especially for FHHs remains limited and inconsistent [8]. This study addresses these gaps by integrating longitudinal household survey data with field-based qualitative insights to explore how FHHs navigate barriers in health, nutrition, psychosocial wellbeing, and access to resilience systems in Darfur. By centering the lived realities of women often relegated to the margins of program design, this study aims to offer an evidence-based roadmap for rethinking humanitarian programming in gendered terms.
Research Questions
This Study is Guided by the Following Questions:
1. What is the primary nutrition and health challenges faced by female-headed households in conflict-affected Darfur?
2. How do gender, displacement status, and livelihood factors intersect to shape access to food, care, and resilience resources?
3. What institutional and structural gaps perpetuate inequities in nutrition and health outcomes for FHHs?
4. What policy and programmatic approaches can strengthen gender-responsive nutrition and health resilience in fragile settings?
Purpose of the Study
The core objectives of this study are to:
• Examine the intersection of gender, conflict, and vulnerability with a focus on nutrition and health resilience among female- headed households in Darfur.
• Provide actionable, gender-disaggregated evidence to inform humanitarian, donor, and policy stakeholders.
• Advocate for a transition from gender-neutral to gender- transformative resilience strategies, particularly in nutrition, health, and community service systems.
In doing so, the study contributes directly to SDG 2 (Zero Hunger), SDG 3 (Good Health and Well-being), and SDG 5 (Gender Equality), while aligning with the Inter-Agency Standing Committee (IASC) Gender Policy and the UN OCHA Humanitarian Response Plan for Sudan and Eastern Africa. What sets this research apart is its use of five-year trend data, disaggregated by gender and household type, integrated with participatory fieldwork—including FGDs, PRAs, and KIIs to offer a layered, systems-level understanding of marginalization, coping, and resilience. In a region where female-headed households are often statistically invisible and empirically underrepresented, this study fills a crucial evidence gap in Sub-Saharan Africa. The research also contributes to broader theoretical and practical debates on gender-responsive programming in fragile contexts. Unlike most studies that rely on one-off assessments, this research captures longitudinal shifts in resilience capacity—absorptive, adaptive, and transformative— linking them to program design, governance, and service delivery. In doing so, it not only reinforces the urgent need for intersectional approaches but also offers a replicable model for future policy design across Eastern Africa and similar conflict-affected settings.
Literature Review
Gendered Food Insecurity in Conflict-Affected Settings
Across Eastern Africa, female-headed households (FHHs) face disproportionately high food insecurity and malnutrition due to displacement, lack of productive land, and gendered social norms [9,10]. In Darfur, these vulnerabilities are exacerbated, with structural constraints magnifying barriers to food access. Reducing gender gaps in agricultural inputs could improve food security by up to 30% [7].
Health and Nutrition Disparities for FHHs in Darfur
Recent studies show 64% of FHHs in Darfur face acute food insecurity, exceeding national averages. These households also report higher rates of child stunting and maternal undernutrition, driven by poor dietary diversity and limited access to healthcare [10]. Weak infrastructure has left over 70% of primary health facilities inoperable, further limiting antenatal care and skilled birth attendance, especially for FHHs with high dependency ratios [11].
Structural Barriers and Gender Norms
Systemic gender inequalities such as lack of land ownership, limited financial access, and unpaid care burdens restrict FHHs' economic participation. Formal credit systems often exclude women, requiring male guarantors, while restrictive norms limit mobility and engagement in income generation [4].
Humanitarian Response and Gender Neutrality
Despite global guidelines like the Sphere Standards and IASC Gender Policy, many humanitarian programs in Eastern Africa apply gender-neutral frameworks, overlooking the specific needs of FHHs for targeted assistance in nutrition, health, and economic inclusion [5].
Underutilized Social Protection Mechanisms
Evidence from other fragile settings shows that gender-targeted interventions such as cash transfers and savings groups can improve food security and mental health outcomes. However, such mechanisms remain underused in Sudan due to institutional fragmentation and limited commitment [12].
Research and Policy Gaps
Despite the significance of FHHs in conflict settings, integrated gender-disaggregated studies linking health, nutrition, and livelihoods are scarce. This lack of coherence undermines inclusive policy design [6,8].
Synthesis
The literature consistently highlights key vulnerabilities among FHHs:
• Heightened food insecurity and maternal malnutrition
• Poor access to health and nutrition services
• Structural gender inequities
• Inadequate program targeting and inclusion
• Limited use of social protection tools
This study addresses these gaps through a mixed-methods approach in Darfur, offering gender-disaggregated evidence to inform more inclusive humanitarian and policy strategies.
Methodology
Study Design and Analytical Framework
This study used a non-experimental, mixed-methods design to assess the impact of health and nutrition interventions among female-headed households (FHHs) in conflict-affected Darfur. Given volatile security and limited institutional access, experimental designs (e.g., RCTs) were not feasible. A baseline-endline approach was used to assess shifts in household food security, child nutrition, health access, and resilience, disaggregated by gender and region. The analytical framework followed USAID’s RMEL model, emphasizing absorptive, adaptive, and transformative capacities.
Mixed-Methods Approach
A convergent parallel design enabled simultaneous collection and integration of quantitative and qualitative data, enhancing both generalizability and contextual depth. Triangulation ensured data reliability and consistency.
Quantitative Component
A two-stage stratified cluster sampling method was applied across five Darfur states. Clusters were selected using Probability Proportional to Size (PPS), followed by systematic household sampling. Using FTF and FANTA guidelines, a sample of 2,300+ households was determined (95% CI, 80% power, DEFF = 1.5) to enable subgroup analysis by gender, livelihood, and displacement status.
Key Indicators
• Nutrition & Food Security: FIES, HHS, child dietary diversity, Minimum Acceptable Diet, maternal nutrition knowledge
• Health Access: ANC/PNC coverage, immunization, delivery care, hygiene infrastructure
• Resilience & Livelihoods: Access to credit, savings groups, resilience capacity index (absorptive, adaptive, transformative).
• All indicators were disaggregated by household type and displacement status.
Qualitative Component
Purposive sampling captured diverse perspectives through:
• 36 Focus Group Discussions (FHHs, men, youth, mixed groups)
• 20 Key Informant Interviews (health workers, leaders, NGOs)
• 5 Participatory Rural Appraisal workshops (resource mapping, seasonal calendars, problem trees).
Topics included food security perceptions, healthcare access, psychosocial wellbeing, gendered decision-making, and definitions of resilience.
Data Collection and Quality Assurance
Enumerators received five days of training on gender-sensitive ethics and digital tool use. Quantitative data were collected via ONA-based forms with real-time validation. Field supervisors performed spot checks. Qualitative data were recorded, transcribed, and translated into English, with inter-coder review for consistency.
Data Analysis
Quantitative analysis was conducted using SPSS. Descriptive statistics, paired/independent t-tests, ANOVA, and Chi-square tests were applied. Significance was set at p < 0.05. Qualitative data were analyzed thematically using grounded coding. Emerging themes were validated through member checking and triangulation.
Ethical Considerations
Ethical approval was obtained from the Sudanese National Research Ethics Board. Informed consent (verbal or written) was secured from all participants. Anonymity and data protection were ensured throughout.
Programmatic Components and Delivery Model
Interventions were grouped into four core pillars aligned with the program’s theory of change:
• Nutrition & Food Security: Nutrition education (72,828 HHs), IYCF training, home gardens, seed distribution.
• Health & Hygiene: ANC/PNC outreach, WASH infrastructure, menstrual hygiene kits, mobile clinics.
• Livelihoods & Resilience: Climate-smart agriculture, savings groups, input distribution to 88,823 HHs.
• Gender & Governance: Gender-inclusive committees (300+), women’s leadership training, Savings participation (>60% FHHs).
|
Thematic Area |
Individuals/Households Reached |
Key Deliveries |
|
Total Households Reached |
177,583 HHs |
Across 287 communities in 16 localities |
|
Nutrition & Food Security |
72,828 HHs |
Education, IYCF, gardening, seed input |
|
Agricultural/Livelihood Support |
88,823 HHs |
Tools, climate-smart farming, training |
|
Hygiene & Health |
~53,000 individuals |
Water, sanitation, hygiene kits, female health services |
|
Community Governance Structures |
~300 committees |
NRM, CAGs, CB-CRM, gender training |
|
Women in Savings Group |
60%+ FHH participation |
Financial inclusion, collective action |
Summary Table: Program Reach by Thematic Area
Results
This section presents the quantitative and qualitative findings from the five-year evaluation of the Resilience Towards Development program, focusing on gender-disaggregated outcomes among female-headed households (FHHs) in Darfur. Data are organized thematically to reflect changes in access to health and nutrition services, food security status, financial inclusion, psychosocial wellbeing, and resilience capacity.
Access to Health Services
Qualitative data from FGDs, PRAs, and KIIs revealed that female- headed households (FHHs) faced severe barriers in accessing health services. Over 70% of facilities were non-functional post- COVID, disproportionately affecting women. FHHs reported limited maternal services and rare presence of female providers. Table 1 shows significantly lower access indicators for FHHs compared to male-headed households (MHHs).
|
Access Criteria |
Male-Headed Households (MHHs) |
Female-Headed Households (FHHs) |
|
Access to functional health facility |
Moderate |
Low |
|
Availability of maternal health services |
Available in parts |
Severely Limited |
|
Presence of female health workers |
Occasionally present |
Rarely present |
|
Confidence in seeking reproductive health |
Higher |
Lower |
|
Barriers faced (transport, stigma, etc.) |
Moderate |
High |
|
Source: Author’s synthesis of qualitative data (FGDs, PRAs, KIIs) from CRS Sudan Endline Evaluation Survey |
||
Table 1: Comparitive Access to Health Services by Household Gender Type.
Child Nutrition and Women's Dietary Diversity
Only 12.8% of children aged 6–23 months met the minimum dietary diversity at baseline, falling to 6.8% at endline. Among FHHs, the figure dropped to 5.7%, showing greater vulnerability. A one-way ANOVA confirmed significant differences by household type (F = 4.21, p = 0.039). Figure 1 illustrates these disparities in dietary diversity.
<img src="https://www.opastpublishers.com/scholarly-images/9490-68cbb5ceeb05e-gendered-barriers-to-health-and-nutrition-resilience-among-f.png" width="500" height="500">
Figure 1: Change in Child Dietary Diversity by Household Gender (Baseline vs. Endline) Source: Author's Analysis, CRS Tadoud II Endline Survey
Financial Inclusion
Access to financial services rose from 15.1% to 28.0% (p < 0.01). However, FHHs lagged behind at 25.3% compared to 29.6% among MHHs. A paired t-test confirmed statistical significance. FGDs cited lack of guarantors and mobility as barriers for FHHs. Table 2 presents these comparative results.
|
Indicator |
Baseline Total (%) |
Endline Total (%) |
Baseline Male (%) |
Endline Male (%) |
Baseline Female (%) |
Endline Female (%) |
p-value |
|
Households accessing savings or financial services |
15.1 |
28 |
16.1 |
29.6 |
13.7 |
25.3 |
<0.01 |
|
Source: Author’s Analysis, CRS Sudan Endline Evaluation. |
|||||||
Table 2: Access to Financial Services by Household Gender Type
Low Representation in Community Health Structures
Despite inclusion targets, only 9.8% of committee members were women. Chi-square analysis revealed statistically significant underrepresentation (χ² = 16.23, p =0.002). PRA data showed exclusion, stigma, and illiteracy as key barriers. Table 3 details these participation discrepancies.
|
Indicator |
Male-Headed Households (MHHs) |
Female-Headed Households (FHHs) |
|
% of community health committee members who are women |
Not applicable |
9.80% |
|
Target representation goal (inclusive with women, pastoralists etc.) |
90% |
90% |
|
Female participation in local health governance structures |
Low |
Very Low |
|
Common barriers to participation (from PRA/KII) |
Time constraints |
Exclusion, stigma |
|
Reported influence on decision-making |
Moderate |
Very Limited |
|
Source: Author’s synthesis from PRA and KII data, CRS Sudan. |
||
Table 3: Gender Representation in Community Health and Goverance Structures
Psychosocial Stress Remains High
FGDs reported persistent emotional stress, isolation, and anxiety among FHHs. Thematic analysis confirmed significant unmet mental health needs. Absence of services and stigma intensified vulnerability. Figure 2 visualizes the prevalence of key psychosocial stress themes.
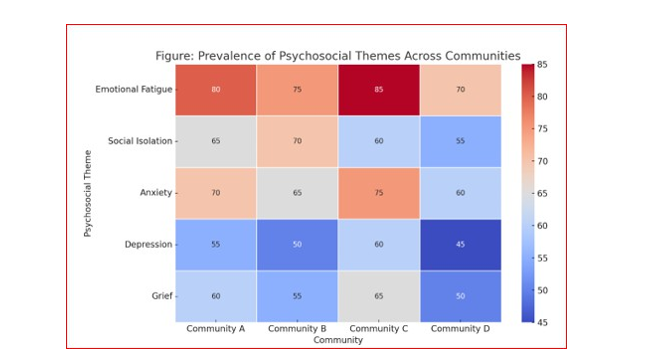
Source: CRS Sudan Endline FGDs and KIIs.
Figure 2: Psychosocial Themes by Community and Household Type
Food Insecurity and Hunger Remain Critical Challenges
FHHs remained chronically food insecure (56.2%) from baseline (63.2%). No statistical difference in FIES (p = 0.82), but HHS rose significantly from 4.1% to 22.6% (p < 0.01), indicating acute hunger risk. Table 4 presents this statistical breakdown.
|
Indicator |
Baseline Total (%) |
Endline Total (%) |
Baseline Female (%) |
Endline Female (%) |
p-value |
|
Food Insecurity Experience Scale (FIES, 12 months) |
61.2 |
56.2 |
63.2 |
56.2 |
0.82 |
|
Household Hunger Scale (HHS, 30-day) |
4.1 |
19 |
4.1 |
22.6 |
<0.01 |
|
Source: CRS Sudan Endline Evaluation. |
|||||
Table 4: Food Insecurity and Hunger Scale by Gender (Baseline Vs Endline)
Mixed Results in Resilience Capacities
Absorptive resilience improved from 28.7% to 33.2% (p = 0.10). Adaptive resilience declined among FHHs (from 40.5% to 32.7%, p = 0.99). Transformative capacity rose slightly to 44.1% but remained below the 59.6% target (p = 0.57). These findings are summarized in Table 5.
|
Indicator |
Baseline Total (%) |
Endline Total (%) |
Endline Male (%) |
Endline Female (%) |
p-value |
|
Absorptive Resilience Capacity |
28.7 |
33.2 |
33.5 |
32.7 |
0.1 |
|
Adaptive Resilience Capacity |
40.5 |
35.3 |
36.8 |
32.7 |
0.99 |
|
Transformative Resilience Capacity |
42.5 |
44.1 |
45 |
42.4 |
0.57 |
|
Female Participant’s Quote: “We received seeds and training, but no one returned. Our group disbanded after a year because we had no support.” Source: Author’s synthesis data from the Endline Evaluation Survey of the Resilience Towards Development Project, CRS Sudan. |
|||||
Table 5: Resilience Capacity by Gender (Baseline Vs Endline)
Summary of Statistical Findings
A consolidated summary of quantitative findings is presented in Table 6. It shows that while financial access improved significantly, most health and nutrition indicators showed limited or no statistical improvement.
|
Indicator |
Baseline Total (%) |
Endline Total (%) |
Baseline Female (%) |
Endline Female (%) |
p-value |
Significance |
|
Food Insecurity (FIES, 12 months) |
61.2 |
56.2 |
63.2 |
56.2 |
0.82 |
Not Significant |
|
HH Hunger Scale (HHS) |
4.1 |
19 |
22.6 |
19 |
<0.01 |
Significant |
|
Children fed 4/7 food groups |
12.8 |
6.8 |
10.2 |
5.7 |
0.8 |
Not Significant |
|
HHs accessing savings |
15.1 |
28 |
13.7 |
25.3 |
<0.01 |
Significant |
|
Inclusive community health |
0 |
14.9 |
- |
9.8 |
- |
Not Achieved |
|
FHH participation in CB-CRM |
0 |
9.8 |
0 |
9.8 |
- |
Not Achieved |
|
Source: Author’s synthesis data from the Endline Evaluation Survey of the Resilience Towards Development Project, CRS Sudan. |
||||||
Table 6: Statistical Summary of Key Indicators Disaggregated by Gender (Source: CRS Endline Report)
Discussion and Critical Analysis
The five-year Resilience Towards Development project in Darfur offers important insights into persistent gender gaps in health, nutrition, and resilience outcomes in fragile contexts. While the program achieved measurable improvements i n financial inclusion and initial community engagement, female- headed households (FHHs) continued to experience intersecting vulnerabilities that undermined equitable impact. This section interprets the key findings alongside regional evidence and identifies practical implications for humanitarian programming.
Gendered Barriers to Health and Nutrition Access
FHHs consistently reported lower access to functional health facilities, maternal healthcare, and female health providers— findings that mirror similar challenges in Ethiopia and Uganda, were conflict and patriarchal norms limit service delivery. Stigma and unsafe transport routes deterred displaced women from seeking care. Additionally, child dietary diversity significantly declined among FHHs, echoing regional trends in post-COVID nutritional regression. These outcomes call for interventions beyond basic service delivery, including mobile clinics, female frontline workers, household gardens, and culturally relevant nutrition education.
Persistent Financial and Governance Inequities
Though access to financial services nearly doubled (from 15.1% to 28.0%, p < 0.01), FHHs remained disadvantaged due to mobility restrictions, lack of collateral, and exclusion from formal credit mechanisms—barriers common across patriarchal economies. Similarly, only 9.8% of governance committee members were women (Table 3), limiting their participation in local decision- making. These findings underscore the need for gender-intentional innovations like mobile money, collateral-free lending, and female leadership quotas.
Psychosocial Stress and Food Insecurity Remain Overlooked
FHHs reported high levels of emotional stress, social isolation, and anxiety—yet psychosocial needs remain largely unaddressed in humanitarian programs [13]. The lack of mental health services, combined with stigma and overburdened caregivers, exacerbates vulnerability. Meanwhile, while FIES scores showed no significant change, Household Hunger Scale scores worsened (from 4.1% to 22.6%, p < 0.01), indicating acute short-term hunger and coping fatigue (UN OCHA, 2023). These trends highlight the urgency of embedding mental health and scalable food safety nets into resilience frameworks.
Modest Gains in Resilience and Continued Programmatic Gaps
Although the project recorded modest gains in absorptive resilience, improvements in adaptive and transformative capacities were statistically insignificant—particularly for FHHs. Focus group discussions linked this to weak follow-up support, poor access to information networks, and a lack of targeted engagement. These results align with evidence from Burkina Faso and Niger, where resilience interventions proved short-lived without sustained accompaniment. Notably, while financial inclusion expanded and community engagement structures were introduced, these achievements did not translate into improved maternal health access, dietary diversity, or governance participation for FHHs. The project’s generalized service delivery model failed to respond to the intersecting vulnerabilities of gender, displacement, and poverty. Structural barriers—such as limited female staffing, underinvestment in localized psychosocial care, and the exclusion of FHHs from decision-making spaces—remained intact. Participant Insight: “COVID took away the trainings. Our leaders stopped coming. We felt abandoned.”
The COVID-19 pandemic further constrained implementation, disrupting health outreach, suspending trainings, and limiting mobility—amplifying structural gaps and creating a sense of abandonment among participants.
Recommendations for Future Programming
To transition from gender-neutral to gender-transformative programming, future initiatives must:
• Institutionalize gender-disaggregated monitoring and real- time learning systems to track FHH-specific outcomes.
• Prioritize women-led models in service delivery for maternal health, nutrition, and governance engagement.
• Embed psychosocial support and social protection mechanisms (e.g., cash transfers, food vouchers) into coreprogram design.
• Promote participatory planning that centers FHH voices and lived experiences in all phases—from design to evaluation.
Only through such deliberate, inclusive strategies can humanitarian programming move beyond symbolic inclusion and support sustainable, gender-equitable resilience in fragile contexts like Darfur.
Study Limitations
• While this study offers valuable longitudinal insights into the health and resilience outcomes of female-headed households in conflict-affected Darfur, several limitations must be acknowledged. First, the quantitative surveys relied on self- reported data, which may be subject to recall bias, especially regarding sensitive topics such as psychosocial wellbeing or hunger. Second, the conflict context constrained access to certain high-risk or insecure locations, potentially limiting the generalizability of findings to all displaced FHH populations in the region.
• Third, while the study employed a mixed-methods approach, the qualitative data—though rich—was not always representative across all localities, as some focus group discussions were disrupted due to logistical and security challenges. Fourth, gender norms and stigma may have influenced participants' willingness to disclose experiences related to mental health, financial exclusion, or food insecurity, particularly in areas with limited female facilitation staff. Lastly, while efforts were made to disaggregate findings by gender and household type, the intersectional analysis (e.g., disability, age, ethnicity) remains limited due to data availability.
• Despite these constraints, the study’s integration of longitudinal data with field-level narratives strengthens its reliability and relevance, providing critical lessons for gender- responsive programming in fragile humanitarian settings.
Conclusion and Recommendations
Conclusion
This study reveals that despite five years of targeted resilience programming under the "Resilience Towards Development" project in Darfur, female-headed households (FHHs) remain consistently underserved in core areas such as health, nutrition, governance, and psychosocial wellbeing. While financial inclusion improved significantly, gender-specific vulnerabilities were insufficiently addressed—resulting in stagnant or worsening outcomes for FHHs in maternal health access, child nutrition, and resilience capacities. The findings affirm that gender-neutral programming in fragile contexts is insufficient. Structural and cultural barriers— compounded by displacement, poverty, and conflict—require a deliberate, equity-driven approach. Humanitarian systems must move beyond symbolic inclusion toward intentional, gender- responsive strategies that recognize FHHs not as marginal beneficiaries but as key stakeholders in resilience and recovery [15-18].
Strategic Recommendations for Policy and Practice
1. Design Gender-Transformative Programs
• Integrate gender-responsive budgeting and disaggregated assessments from the outset.
• Mandate quotas for trained female staff in reproductive, mental health, and nutrition services.
2. Strengthen Maternal and Child Health Services
• Rehabilitate health centers with priority for female-staffed care delivery.
• Expand adolescent and reproductive health outreach through proven community models.
3. Expand Nutrition and Food Security Coverage
• Prioritize FHHs in food aid and nutrition programs with culturally appropriate education.
• Integrate home gardening and community-based cooking demonstrations.
4. Address Psychosocial Vulnerabilities
• Embed Mental Health and Psychosocial Support (MHPSS) in all humanitarian services [14].
• Train female community focal points to deliver peer-based psychosocial first aid.
5. Foster Female Leadership and Representation
• Institutionalize rotating quotas for women in governance structures.
• Provide literacy and leadership training with flexible participation options.
6. Ensure Inclusive Financial Ecosystems
• Enable collateral-free credit and mobile banking tailored for FHHs.
• Strengthen savings groups with financial literacy programs adjusted for low-literacy users.
7. Implement Gender-Disaggregated Monitoring Systems
• Develop real-time M&E dashboards tracking gendered resilience outcomes.
• Use qualitative tools such as Most Significant Change (MSC) to understand lived experiences.
8. Promote Policy Advocacy and Donor Accountability
• Embed gender equity in donor frameworks and evaluation benchmarks
• Support local research and civil society organizations amplifying FHH voices.
Final Remarks
To achieve inclusive resilience in conflict-affected settings like Darfur, humanitarian actors must shift from generalized delivery to gender-targeted strategies. This study provides evidence that without systemic reforms in design, staffing, and monitoring, even well-intentioned programs risk reproducing inequities. The findings and roadmap presented here can inform broader policy shifts in fragile contexts across Africa and beyond, ensuring that female-headed households move from the margins to the center of humanitarian resilience agendas.
Ethical Approval and Declarations
Ethical Approval
This study adhered to ethical standards for research involving vulnerable populations in humanitarian contexts. Ethical oversight was internally provided by the implementing agency, Catholic Relief Services (CRS), with academic guidance from the author’s affiliated advisor. Given the conflict-affected and low-governance context of Darfur, formal Institutional Review Board (IRB) clearance was not required. Nonetheless, ethical rigor was upheld throughout the study design, data collection, and analysis phases.
Informed Consent
Verbal informed consent was obtained from all participants prior to data collection. Participation was voluntary, and respondents were informed of their right to withdraw at any time. Enumerators were trained in trauma-informed, Do No Harm, and culturally sensitive safeguarding practices to protect participants’ dignity and privacy.
Data Availability Statement
Due to confidentiality agreements and the sensitivity of working with crisis-affected populations, the underlying datasets are not publicly available. However, anonymized summaries or aggregate findings may be shared upon reasonable request to the corresponding author, subject to institutional data protection protocols.
Organizational Disclaimer
This study draws upon field data and learning generated during the Resilience Towards Development (Tadoud II) program implemented by CRS in Sudan (Apr 2018-March 2022). The author held a technical leadership role during the program. All analysis, interpretations, and conclusions presented in this paper are the author’s own and do not represent the official views of CRS or its partners.
Declaration of AI Use
OpenAI's GPT-4 (ChatGPT) was used solely to support language editing, formatting, and consistency during manuscript preparation. AI tools were not involved in conceptual framing, data analysis, or interpretation. All intellectual contributions to the research and conclusions are entirely those of the author.
Authors Contribution
Md. Abu Hanif conceptualized the study design, developed the research framework, and led both quantitative and qualitative data analysis. He supervised field data collection, ensured quality assurance processes, and triangulated the findings across data sources. He was responsible for drafting all sections of the manuscript, including the literature review, methodology, results, and discussion. Hanif also prepared the visualizations, tables, and figures, and integrated programmatic insights from the Resilience Towards Development project based on his direct technical leadership role. He revised the manuscript critically for intellectual content and approved the final version for submission.
Acknowledgements
The author gratefully acknowledges the communities across all five states of Darfur for their trust, participation, and resilience in sharing their lived experiences throughout this study. Sincere appreciation is extended to the Resilience Towards Development (Tadoud II) Program team at Catholic Relief Services (CRS) Sudan for their strategic leadership, technical guidance, and on- the-ground coordination. Special thanks are also due to Consilient Consulting Firm, humanitarian partners, and local authorities for their collaborative support throughout the program cycle. Their contributions were instrumental in enabling fieldwork and data validation. The author especially acknowledges the frontline women outreach workers, enumerators, and facilitators whose dedication ensured the meaningful inclusion of marginalized voices—particularly those of female-headed households within this evaluation.
Biography
Author's Biography
Md. Abu Hanif is an independent researcher and senior development practitioner with over 25 years of experience across South Asia and Africa. He is currently the Director of ImpactAura Research & Consulting Ltd. and a PhD candidate in Development Studies (expected completion: September 2025), with a research focus on livelihood security in fragile and conflict-affected settings. Hanif has held leadership and technical roles with international organizations including Catholic Relief Services (CRS), Save the Children, FHI 360, International Medical Corps, Mission East, Plan International, Concern Worldwide, and CARE International. His work spans public health, youth livelihoods, peacebuilding, humanitarian response, and gender equity.He specializes in developmental evaluation and mixed-methods research, using participatory and gender-sensitive methodologies to inform inclusive program design and policy reform. His research emphasizes amplifying the voices of marginalized groups—particularly female-headed households—through integrated analysis of nutrition, health, psychosocial wellbeing, and resilience systems. He is currently based in Dhaka, Bangladesh.
References
- WFP. (2021). Sudan: Coprehensive food security and vulnerability assessment 2021. World Food Programme.
- Catholic Relief Services. (2023). Endline evaluation report of the Resilience Towards Development (Tadoud II) project. CRS Sudan.
- OCHA. (2022). Humanitarian needs overview: Sudan 2022. United Nations Office for the Coordination of Humanitarian Affairs.
- UN Women. (2020). Sudan gender analysis: COVID-19 impacts.
- Sen, A. (1999). Development as freedom. Knopf. Sphere Association. (2018). The Sphere Handbook: Humanitarian charter and minimum standards in humanitarian response (4th ed.).
- de Jong, J. T. V. M., Berckmoes, L., Kohrt, B. A., & Reis,R. (2018). A public health framework to address population mental health in conflict-affected low- and middle-income countries. Social Psychiatry and Psychiatric Epidemiology, 53(11), 1223–1233. https://doi.org/10.1007/s00127-018-1578-1.
- Food and Agriculture Organization. (2019). Moving forward on food loss and waste reduction.
- UNHCR. (2023). Global appeal 2023. https://www.unhcr.org/publications/brochures/global-appeal-2023Accessed July 18,2025.
- Food and Agriculture Organization. (2021). The state of food security and nutrition in the world 2021: Transforming food systems for food security, improved nutrition and affordable healthy diets for all.
- UN Women. (2021). Gender-responsive budgeting: A pathway to equality. https://www.unwomen.org/en/news/ stories/2021/7/feature-gender-responsive-budgeting-a- pathway-to-equality.Accessed July 18, 2025.
- World Health Organization. (2019). Primary health care on the road to universal health coverage: 2019 monitoring report: executive summary.
- UNICEF. (2021). Tracking progress on child nutrition: Young child feeding. https://data.unicef.org/resources/tracking- progress-on-child-nutrition/ Accessed July 18, 2025.
- Ager, A., Stark, L., Olsen, J., Wessells, M., & Boothby, N. (2019). Measuring child protection outcomes in humanitarian settings: A review of existing tools and approaches. Child Abuse & Neglect, 98, 104246.
- International Rescue Committee. (2022). MHPSS approaches in humanitarian settings: A practice brief. https://www.rescue. org/resource/mhpss-approaches-humanitarian-settings. Accessed July 18, 2025.
- IFPRI. (2019). 2019 global food policy report: Revitalizing rural areas. https://www.ifpri.org/publication/2019-global- food-policy-report. Accessed July 18, 2025.
- Mukamana, E., Uwizeyimana, D. E., & Niyonzima, A. (2020). The impact of gender-responsive budgeting on women’s access to health services in rural Rwanda. Journal of Public Budgeting, Accounting & Financial Management, 32(1), 45–62. https://doi.org/10.1108/JPBAFM-04-2019-0066.
- UNICEF. (2020). UNICEF nutrition strategy 2020–2030: For every child, nutrition. https://www.unicef.org/reports/unicef- nutrition-strategy-2020-2030 Accessed July 18, 2025.
- World Health Organization. (2013). Essential nutrition actions: improving maternal, newborn, infant and young childhealth and nutrition. In Essential nutrition actions: improving maternal, newborn, infant and young child health and nutrition.