
International Journal of Diabetes & Metabolic Disorders(IJDMD)
ISSN: 2475-5451 | DOI: 10.33140/IJDMD
Impact Factor: 1.23


Research Article - (2024) Volume 9, Issue 1
Frequency of ABO/Rh Blood Groups Among Patients with Diabetes Mellitus in Luanda, Angola
2Instituto Nacional de Investigação em Saúde (INIS), Luanda, Angola
3Centro de Investigação em Saúde de Angola (CISA), Caxito, Angola
4Instituto Politécnico de Malanje da Universidade Rainha Njinga A Mbande (IPM/URNM), Malanje, Angola
5Centro de Estudos, Investigação Cientifica e Pós-graduação (CEIP) da Universidade Privada de, Angola
6Instituto de Educação Física e Desportos da Universidade Agostinho Neto (IEFD/UAN), Luanda, Angola
7Instituto Politécnico, Universidade Rainha Njinga A Mbande (IPM/URNM), Malanje, Angola
8Centro Nacional de Investigação Científica (CNIC) Luanda, Angola
Received Date: Dec 05, 2023 / Accepted Date: Jan 08, 2024 / Published Date: Jan 15, 2024
Copyright: ©Â©2024 Edson Kuatelela Cassinela, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Sacomboio, E. N. M., Pululo, S. A., Sebastião, C. S., Tchivango, A. T., Silveira, S. D. R, et al. (2024). Frequency of Abo/Rh Blood Groups Among Patients with Diabetes Mellitus in Luanda, Angola. Int J Diabetes Metab Disord, 9(1), 01-08.
Abstract
Background Diabetes is a chronic disease characterized by alterations in glucose, lipid, and protein metabolism, which can be identified by detecting high blood glucose levels. In this study we evaluated the frequency of ABO/Rh blood groups in patients with diabetes treated in Luanda, during the second half of 2020.
Methods This was an observational, analytical, prospective study with a quantitative approach conducted with 100 patients with diabetes.
Results The mean age of patients was 48,4±14 years old. Patients males (63%) with a mean age of 47.9±14.5 years old, secondary educational level (33%), and living in urbanized areas from Luanda (33%), which were the most prevalent in this studied population. About 57% did not exercise before the disease and did not have the disease in the family (51%). About 71% of the patients used insulin to treat diabetes. ORh+ and ARh+ blood groups were the most frequent. The majority of the patients were less than 4 years with diabetes.
Conclusion We concluded that the patients most affected by diabetes were the elderly, males, from urbanized areas, and with blood groups ORh+ or ARh+. Further studies assessing the relationship between ABO/Rh blood groups and diabetes among the Angolan population are needed.
Keywords
Diabetes, ABO/Rh blood groups, Angola
Introduction
Diabetes mellitus (DM) is a metabolic disorder of multiple etiologies, characterized by chronic hyperglycemia with disorders of carbohydrate, fat, and protein metabolism resulting from defects in insulin secretion, insulin action, or both [1]. Pathological processes are involved in the development of this disorder, ranging from the destruction of pancreatic β-cells with consequent insulin deficiency to abnormalities inducing resistance to insulin action [2].
Approximately 15 million premature deaths per year worldwide are attributable to noncommunicable diseases, including cardiovascular disease and DM, more than 85% of these deaths occur in low- and middle-income countries [3,4].
Diabetes mellitus is the most common metabolic disorder that affects people all over the world, both in developing and developed countries. In 2017 were estimated more than 451 million people living with DM worldwide. These numbers are expected to increase to 693 million by 2045 [5]. In the African region, the average prevalence was 4.9% in 2013 [6,7]. The main human blood group systems are ABO and Rh. The frequency distribution of these blood groups varies markedly across different races, ethnic and socioeconomic groups [8].
Blood group antigens are believed to be among the hereditary determinants and play a vital role in understanding the genetics and susceptibility to DM [9]. Since the discovery of blood groups, there has been a great deal of interest in discovering a possible correlation between ABO/Rh blood groups and different pathological conditions [10]. The clinical significance of the ABO and Rh blood group system goes beyond transfusion medicine, several studies suggest an important involvement of ABO and Rh blood group antigens in the development of different diseases [11,12,13]. Including different types of tumors such as gastric cancer, salivary gland tumors, duodenal ulcer, colorectal cancer, thyroid disorders, ovarian tumors, coronary heart disease, and DM, especially type 2 DM [14,15,16,17,18].
The pathophysiological mechanisms of the association between ABO blood group phenotypes with type 2 DM and associated factors are not well understood. However, there are a few possible hypotheses: the first is that ABO blood groups are linked to specific molecules related to type 2 DM. Genome-wide association studies have shown that variants at the ABO gene loci, especially the A and B antigens, are associated with increased levels of plasma lipids and inflammatory markers such as intercellular adhesion molecule 1 (ICAM-1), E-selectin, P-selectin, and tumor necrosis factor-2 (TNF-2), These molecules are known as mediators of inflammation that affect insulin and its receptors and have contributed to the development of DM [19,20].
ABO blood group phenotypes are significantly associated with type 2 DM. In this study, blood group B had a positive association with type 2 DM, while blood group O had a negative association with type 2 DM. However, blood groups A, AB, and Rh were not associated with type 2 DM, this study also sought to determine the relationship between the phenotypes of ABO and Rh blood groups with factors associated with DM, and it was found that blood group A is associated with increased systolic blood pressure, and blood group B was significantly associated with decreased total cholesterol levels [21]. Another study also showed that people of blood group B have a greater susceptibility to DM [22] and women with blood group AB have a low risk of developing gestational diabetes [23].
Our previous studies have shown a strong correlation between ABO blood groups and different diseases, one of the studies published in 2021 showed a correlation between ABO blood groups and High Blood Pressure, blood group B and O patients were more likely to develop High Blood Pressure respectively [24]. To date, no study has been carried out to understand the relationship between ABO blood groups and DM in the Angolan population, so in this study, we evaluated the frequency of ABO and Rh blood groups in patients with diabetes treated in Luanda, the capital city of Angola.
Methodology
Study Design and Setting
This was an analytical, prospective study, with a quantitative approach, where the blood group (ABO System) and Rhesus factor were determined in patients with Diabetes Mellitus treated at Hospital do Prenda, located in Luanda, the capital city of Angola, in the second half of 2020. The studied population consisted of 150 patients, from which a sample of 100 patients with Diabetes Mellitus was extracted, regardless of gender and age among those who agree to participate in the study after being informed about the objectives and nature of the study. The study was reviewed and approved by the Ethics Committee for Research on Human Beings of the Instituto Superior de Ciências da Saúde, Agostinho Neto University (nr.198/GD/ISCISA/UAN/2020) and by the Pedagogical and Scientific Department of Hospital do Prenda (nr.43/DCP/HP/2020). All patients gave oral and in writing their informed consent before being included in the study.
Data Collection and Laboratory Procedure
A questionary was used to collect demographic data (such as age, gender, educational level, and area of residence) and clinical data (such as treatment used and complications related to diabetes). A whole blood sample estimated at 2 mL was collected for each patient by the venipuncture technique and the samples were placed in test tubes containing ethylenediaminetetraacetic acid (EDTA). The samples were placed in three wells and the latter was associated with anti-A, Anti-B, and Anti-D reagents (Immucor, Portugal). Blood group determination was performed using the microplate technique according to the manufacturer's instructions, which is an agglutination test between the patient's serum and the anti-A, Anti-B, and Anti-D reagents from each well for phenotypic identification of the blood groups (ABO and Rh).
Statistical Analysis
The data obtained in this study were analyzed using SPSS v20 (IBM SPSS Statistics, USA). Absolute and relative frequencies were determined in the descriptive analysis. Normally data distribution was expressed as mean and standard deviation (SD).
Results
Sociodemographic Characteristics The results in table 1 reveal that the age group most affected by diabetes was between 51-60 years of age, representing 26% (26/100) with a mean age of 55.8±2.6 years, followed by patients aged over 60 years (24%, n=24/100) with a mean age of 66.7±3.9 years, the general mean age of these patients was 48.4±14.9 years. Regarding blood groups, it was observed that the majority were from group O (44%, n=44/100), followed by groups A (27%, n=27/100) and B (23%, n=23/100), the negative Rh factor accounted for only 2%. It was found that most patients with diabetes were male, representing 63% (n=63/100), and females representing 37% (n=37/100). As for the frequency of blood groups, male patients in group O represented about 49.2% (n=31/63), followed by group A (26.9%, n=17/63), group B and AB represented 17.4% (n=11/63) and 6.3% (n=4/63), respectively, no Rh negative factor was identified in this studied population. In females, group O represented 35.1% (n=13/37) and 5.4% (n=2/37) were Rh negative factors, groups A and B, represented 27% (n= 10/37) and 32.4% (n=12/37) respectively, and no female patient was identified with group AB, and the mean age of both sexes was 48.4.
According to the origin of the patients, we observed that the majority of the patients were from the municipality of Luanda, an urbanized area, and the majority of the ORh+ (51.5%, n=17/33), and two patients of the ORh- (6%, n=2/33), followed by groups B, A, and AB represented 21.2% (n=7/33), 18.8% (n=6/33), and 3% (n =1/33), respectively. In the municipality of Kilamba Kiaxi likewis, group O was the most frequent with 60% (n=12/20), followed by groups A and B with 25% (n=5/20), 15% (n=3/20). As for patients from the city of Viana, group O represented about 50% (n=6/12), followed by groups B, A, and AB representing 25% (n=3/12), 16.6% (n=2 /12), and 8.3% (n=1/12), respectively.
The data from the same table clarified that most patients had completed secondary educational level, representing 33% (n=33/100), with a mean age of 40.8±15.9 years, followed by primary education (27%, n=27/100), the mean age of 52.2±12.5 years, the illiterates represented 22% (n=22/100), with a mean age of 55.9± 11.0 years and only 18% (n=18/100) had completed higher education and the average age in this group was 47.6±14.6 years. Regarding blood groups, patients with completed secondary education were mostly from group O representing 39.3% (n=13/33), and 6% (n=2/33) were Rh (-), followed by group A with 30% (n=10/33), groups B and AB represented 18.1% (n=6/33), and 6% (n=2/33) respectively. Primary school patients were mostly from group O with 48.1% (n=13/27), patients from groups A, B, and AB represented 25.9% (n=7/27), 22.2 % (n=6/27), and 3.7% (n=1/27), respectively. We also observed that 51% (n=51/100) of patients with diabetes have no family history, and 49% (n=49/100) reported cases of diabetes in the family with an overall mean age of 48.4 years. As for the blood groups of those who said they did not have the disease in the family, 47% (24/51) were from group O, followed by B, A, and AB representing 27.4% (n=14/51), 23.5% (n=12/51) and 1.9% (n=1/51) respectively, on the other hand, patients with a case report of the disease in the family, the groups with the highest frequency were O, A, B, and AB with 40% (n=20/49), 30% (n=15/49), 18.3% (n=9/49) and 6.1% (n=3/49) respectively.
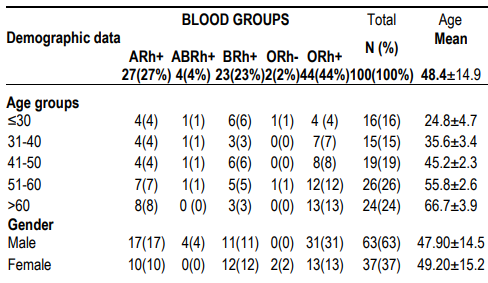
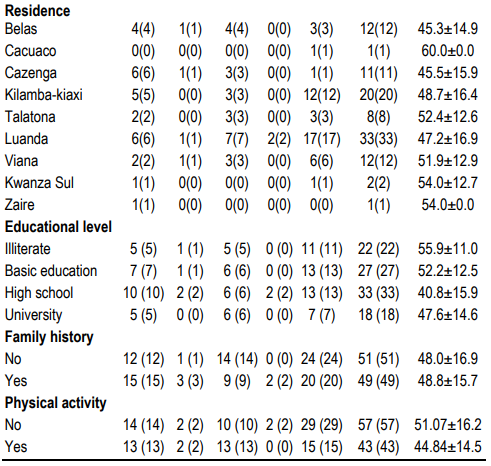
Table 1. ABO/Rh Blood groups distribution according to demographic data
ABO/Rh Blood Groups and Clinical Conditions
The data show that 67% (n=67/100) of the patients had a time of diagnosis of the disease fewer than 4 years with a mean age of 46.3±14.9 years, and the minority of patients (3%, n=3/100) had lived with the disease more than 17 years, with an average age of 56.3±22.0 years. Regarding blood groups, most patients with a time of diagnosis of the disease less than 4 years were from group O, followed by groups B, A, and AB, with 38.8% (n=26/67), 28.3% (n=19/67), 23.8% (n=16/67), and 5.9% (n=4/67), respectively. As for the minority who had a disease diagnosis time of more than 16 years, they were in groups O and A with 66.6% (n=2/3), and 33.3% (n=1/3), respectively.
Regarding treatment, we observed that most patients used insulin, representing 71% (n=71/100), with a mean age of 47.9 years, followed by metformin 25% (n=25/100), with a mean age of 48.7. The use of the glibenclamide 2% (n=2/100) means age 56.0 years and insulin/metformin (2%, n=2/100) mean age 54.5 years were the less frequent. Regarding blood groups, most of those who used insulin were from group O representing 42.2% (n=30/71), while in group O 1.4% (n=1/71) were Rh factor (-) groups A and B had the same frequency of 25.5% (n=18/71), group AB represented 5.6% (n=4/71), and patients using metformin, 48% (n=12 /25) were from group O, followed by group A, B with 32% (n=8/25) and 12% (n=4/25) respectively. Most patients had visual complications representing 52% (n=52/100) with a mean age of 50.2 years, and 32% (n=32/100) had no complications, with a mean age of 42.6 years, patients with renal and visual complications represented 9% (n=9/100) with a mean age of 51.6 years, and those with only renal complications represented 5% (n=5/100) with a mean age of 57 years. Only 2% (n=2/100) had lower limb amputations due to poor glycemic control and late diagnosis and all were from the ORh+ blood group. The data also show visual complications mostly in patients in group O, followed by groups A, B, and AB with 40.3% (n=21/52), 26.9% (n=14/52), 23% (n=12/52), 7.8% (n=4/52), and only 1.9% (n=1/52) group ORh-, respectively. Patients who did not present any complications were also mostly from group O with 43.7% (n=14/32), followed by groups A and B with 34.4% (n=11/32), 18.7% (n=6/32), and only 3.1% (n=1/32) of the group O factor Rh-. Patients with renal complications were mostly in group O with 60% (n=3/5), followed by group B with 40% (n=2/5). Patients with renal and visual complications were mostly from group O with 44.4% (n=4/9), followed by groups B and A with 33.3% (n=3/9), and 22.2% ( n=2/9), respectively. Patients with more severe complications and amputees were of group O.
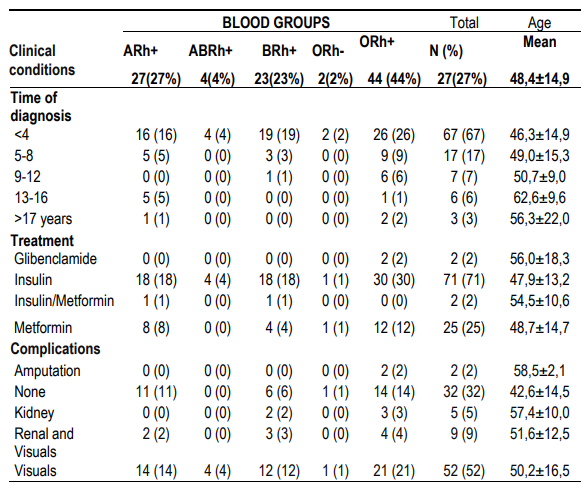
Table 2: ABO Blood groups according to clinical conditions
Discussion
Different study has demonstrated an association between ABO/Rh blood groups with different pathological states, including gastric ulcers, hepatitis B, vascular diseases, Arterial Hypertension, abdominal aortic aneurysms, and cancer [24]. Some epidemiological studies have demonstrated the relationship between the "ABO" blood group and the risk of type 2 DM [25]. Our results demonstrated that diabetes has a high prevalence in patients over 50 years of age, these results corroborate a recent study that analyzed 579 diabetic patients and showed that the highest prevalence was between 40 - 60 years of age [26]. The same study revealed that blood group B has the highest frequency (42%), followed by blood group AB (23%), O (21%), and A (11.4%), respectively, while in our study the highest frequency was observed in blood group O (44%), followed by groups A (27%) and B (23%) respectively [26]. Researchers from different countries found a diverse association between ABO blood groups and DM, this can be explained by the different distribution of blood groups in the population of these countries and varies according to the population [27,28]. The results of our study are in line with different studies, some of them carried out in Pakistan [28], Algeria [29], and Iraq [30] where it was observed that blood group O has the highest prevalence among diabetics patients. Some studies in the literature have shown an increase in the association of blood group O with DM [31,32,33] but others have not [33,34]. On other hand, our study has only two patients with Rh factor (-) and they are both in group O, thus disagreeing with the study on the Rhesus factor. Some studies recently published by some of our research team members in Angola showed a great predominance of blood group B 36.4% (36/99) in patients with Arterial Hypertension, blood group O 56.4% (79/99) 140) in patients with chronic kidney disease and O blood groups, followed by patients in the ABR group in patients with Nephrotic Syndrome and Sickle Cell Anemia [24,43,44,45].
As for sociodemographic factors, in the later stages of the epidemiological transition, low socioeconomic status may be associated with an increased risk of non-communicable diseases such as diabetes mellitus, cancer, and cardiovascular disease [35]. Poverty and food insecurity may contribute to the increase in DM prevalence in some rural African settings where DM prevalence exceeds that in urban areas [38]. In addition to the fact that poverty can contribute to the onset of diabetes potentially through fetal and infant malnutrition or obesity in adulthood (39). In our study, most patients were from the city of Luanda (33%) and Kilamba-Kiaxi (22%). Most patients had completed secondary school education (33%), and different studies have shown that low socioeconomic status, assessed mainly based on income, occupation, and educational level, is an independent risk factor for DM [40,41, 42]. A systematic review and meta-analysis data have shown that an increased incidence of DM is associated with low socioeconomic status in high-, middle-, and low-income countries [42].
Family history is another associated risk factor, in our study we observed that 49% of patients with diabetes have a family history and regarding a healthy lifestyle with physical activity, we found that only 43% practiced some type of physical activity of low intensity. Our findings suggest that subjects with a family history of DM should adopt periodic screening in order to ensure early identification and medical assistance. A family history of type 2 DM is recognized as a crucial non-modifiable risk factor, constituting an easily assessed marker of the genetic predisposition underlying DM [41]. On the other hand, unhealthy eating habits, a sedentary lifestyle, and decreased physical activity are closely associated with an increased risk of type 2 DM, both directly and indirectly, through the promotion of obesity and various components of the metabolic syndrome [42]. The time of diagnosis of DM in 67% was less than 4 years, insulin was the main treatment and, in most cases, the patients had visual complications, a study with the elderly showed an average of fewer than 10 years of DM and the majority reported visual changes, data that corroborate our results [43]. One of the main limitations of our study is the small sample size, which limits the clinical importance of our findings. Our results present a picture of the distribution of ABO/Rh blood groups among patients with diabetes. However, further studies assessing biological and non-biological features related to predisposition to diabetes should be carried out in the population of different settings in Angola.
Conclusion
Our results showed that the blood group O+ was the one with the highest frequency among patients with diabetes. The age group of 51-60 years old, male, low educational level, and area of residence were the most frequent demographic features observed in this studied population. Moreover, most patients were diagnosed in less than 4 years, and almost half of them have a family history of the disease. Further studies should be carried out to deepen the impact of ABO/Rh blood groups on DM predisposition, as well as the molecular aspects that might be associated with the disease in the Angolan population.
Abbreviations
DM: Diabetes mellitus
ICAM-1: intercellular adhesion molecule 1
TNF-2: Tumor necrosis factor-2
SD: standard deviation
EDTA: ethylenediaminetetraacetic acid
Acknowledgment
The authors thank all study participants for agreeing to participate in the research and providing all the information necessary for this study. We thank the clinical and research staff of Hospital do Prenda, ICISA, CEIP/UPRA, CISA/INIS, CNIC, and CFS for their scientific, technical, logistic, and institutional support.
Interest Conflicts
The authors declare that there are no conflicts of interest.
Funding
The authors received no specific funding for this work.
Authors' Contributions
Conceptualization: SAP, ENMS. Data curation: ENMS, EKC, SRS, MC, CAPS, CSS, EEV, ATT. Formal analysis: ENMS, EKC, and CSS. Investigation: ENMS, SAP. Project administration: ENMS, EKC, SRS, MC, CAPS, CSS, EEV. Supervision: ENMS. Validation: ENMS, EKC, and CSS. Writing – original draft: ENMS, EKC, and CSS. Writing – review & editing: ENMS, EKC, SRS, MC, CAPS, EEV, SAP, ATT, and CSS. All authors approved the submitted version of this manuscript.
References
- Kerner W, and Brückel J.“Definition, classification and diag-nosis of diabetes mellitus,”Experimental and Clinical Endocri-nology & Diabetes, vol. 122, no. 7, pp. 384–386, 2014.[2] G. Roglic,“WHO Global report on diabetes: a summary,”International Journal of Noncommunicable Diseases, vol. 1,no. 1, p. 3, 2016
- American Diabetes Association,“Diagnosis and classificationof diabetes mellitus,”Diabetes care, vol. 36, Supplement 1,pp. S67–S74, 2012
- Noncommunicable diseases fact sheet [article online]. 2021. Available from https://www.who.int/news-room/fact-sheets/ detail/noncommunicable-diseases
- Ogurtsova K, Da Rocha Fernandes JD, Huang Y, Linnenkamp U, Guariguata L, Cho NH, et al. IDF Diabetes Atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40–50. pmid:28437734
- Cho NH, Shaw JE, Karuranga S, et al.,“IDF Diabetes Atlas:global estimates of diabetes prevalence for 2017 and projec-tions for 2045,”Diabetes research and clinical practice,vol. 138, pp. 271–281, 2018
- GuariguataL,WhitingDR,HambletonI,BeagleyJ,Linnenkamp U, and Shaw JE.“Global estimates of diabetesprevalence for 2013 and projections for 2035,”Diabetes researchand clinical practice,vol.103,no.2,pp.137–149, 2014
- Aynalem SB and Zeleke AJ.“Prevalence of diabetes mellitusand its risk factors among individuals aged 15 years and abovein Mizan-Aman town, Southwest Ethiopia, 2016: a cross sec-tional study,”International journal of endocrinology, vol. 1,no. 1, pp. 1–7, 2018
- Fagherazzi G, Gusto G, Clavel-Chapelon F, Balkau B, and Bonnet F. “ABO and Rhesus blood groups and risk of type 2diabetes: evidence from the large E3N cohort study,”Diabeto-logia, vol. 58, no. 3, pp. 519–522, 2015.
- Dodiya D, Patel A, and Jadeja J. “Association of ABO blood group with diabetes mellitus,”International Journal of Basicand Applied Physiology, vol. 5, no. 1, pp. 63–66, 2016.
- Waseem AG, Iqbal M, Khan O, and Tahir M. “Associationof diabetes mellitus with ABO and Rh blood groups,”TheAnnals of Pakistan Institute of Medical Sciences, vol. 8, no. 2,pp. 134–136, 2012
- Liumbruno GM and Franchini M. “Beyond immunohaema-tology: the role of the ABO blood group in human diseases,”Blood Transfusion, vol. 11, no. 4, pp. 491–499,2013
- Franchini M, Favaloro EJ, Targher G, and Lippi G. “ABOblood group, hypercoagulability, and cardiovascular and can-cer risk,”Critical Reviews in Clinical Laboratory Sciences,vol. 49, no. 4, pp. 137–149, 2012
- Abegaz SB. "Human ABO Blood Groups and Their Associations with Different Diseases", BioMed Research International, vol. 2021, Article ID 6629060, 9 pages, 2021. https://doi.org/10.1155/2021/6629060
- Wazirali H, Ashfaque R A, and Herzig JW. ABO bloodgroup frequency in Ischemic heart disease patients in Pakistanipopulation,”Pakistan Journal of Medical Sciences, vol. 30,no. 3, pp. 1–3, 1969
- Edgren G, Hjalgrim H, Rostgaard K et al.“Risk of gastriccancer and peptic ulcers in relation to ABO blood type: acohort study,”American Journal of Epidemiology, vol. 172,no. 11,pp. 1280–1285, 2010
- Klechova L and Gosheva-Antonova T. “ABO and Rh bloodgroup factors in thyroid gland diseases,”Vutreshni bolesti,vol. 19, no. 4, pp. 75–79, 1980
- Zhang BL, He N, Huang HB, Song FJ, and Chen KX. “ABO blood groups and risk of cancer: a systematic reviewand meta-analysis,”Asian Pacific Journal of Cancer Prevention, vol. 15, no. 11, pp. 4643–4650, 2014
- Montavon Sartorius C, Schoetzau A, Kettelhack H et al.,“ABO blood groups as a prognostic factor for recurrence inovarian and vulvar cancer,”PLoS One, vol. 13, no. 3, articlee0195213, 2018
- Jankowski JA. Inflammation and Gastrointestinal Cancers:Springer Science & Business Media, Springer, Berlin, Heidel-berg, 2011
- Bahar A, Asadian L, Abediankenai S, Namazi SS, and KashiZ. “Coronary heart disease and ABO blood group indiabetic women: a case-control study,”Scientific Reports,vol. 9, no. 1,pp. 1–6, 2019
- Legese B, Abebe M, Fasil A. "Association of ABO and Rh Blood Group Phenotypes with Type 2 Diabetes Mellitus at Felege Hiwot Comprehensive Referral Hospital Bahir Dar, Northwest Ethiopia", International Journal of Chronic Diseases, vol. 2020, Article ID 2535843, 9 pages, 2020. https://doi.org/10.1155/2020/2535843
- Ghafar M, Khwaja S, Zahid M, Hussain SI, Karim A, & Akram A. (2022). Association of blood groups/Rh and diabetes mellitus in Karachi city, Pakistan. Brazilian Journal of Biology, 84.
- Rom E, Yogev M, Sela N, Jehassi A, Romano S, & Salim R. (2021). The association between ABO blood groups and gestational diabetes mellitus: a retrospective population-based cohort study. The Journal of Maternal-Fetal & Neonatal Medicine, 1-5.
- Sacomboio ENM, Sassoke JL, Hungulo OFS, Ekundi-Valentim E, Cassinela EK, et al. (2021) Frequency of ABO/ Rh Blood Groups and Social Condition of Hypertensive Patients in Luanda. J Blood Disord Med 4(1): dx.doi. org/10.16966/2471-5026.125
- Aggarwal T, Singh D, Sharma B, Siddiqui SS, Agarwal S.Association of ABO and Rh blood groups with type 2 diabetes mellitus in Muzaffarnagar city. National Journal of Physiology, Pharmacy and Pharmacology.2018; 8(2): 167-170.
- Prakash, Satyam, et al. Exemplification of ABO Blood Groups in Patients with Diabetes Mellitus. MedS Alliance Journal of Medicine and Medical Sciences, 2022, vol. 2, no 3, p. 70-75.
- Daniels G. Human blood groups. 2nd ed. USA: Blackwell scientific. 2002.
- Waseem AG, Iqbal M, Khan OA, Tahir M. Association of Diabetes Mellitus with ABO and Rh Blood Groups. Ann Pak Inst Med Sci. 2012;8:134-136.
- Dali SM, Belmokhtar F, Boazza F. The relationship between ABO/ rhesus blood groups and type 2 diabetes mellitus in Maghnia, western Algeria. S AfrFamPract. 2011; 53(6).
- Jassim WE. Association of ABO blood group in Iraqis with hypercholesterolaemia, hypertension and diabetes mellitus. East Mediterr Health J. 2012; 18:888-91.
- Aggarwal T, Singh D, Sharma B, Siddiqui SS, Agarwal S.Association of ABO and Rh blood groups with type 2 diabetes mellitus in Muzaffarnagar city. National Journal of Physiology, Pharmacy and Pharmacology.2018; 8(2): 167-170
- Wolpin BM, Chan AT, Hartge P, Chanock SJ, Kraft P, Hunter DJ, et al. ABO blood group and incidence of epithelial ovarian cancer. Int J Cancer. 2011;128(2):482-486.
- Kamil M, Al-Jamal HA, Yusoff NM. Association of ABO blood groups with diabetes mellitus. Libyan J Med. 2010; 5: 4847.
- Bener A, Yousafzai MT.The distribution of the ABO blood groups among the diabetes mellitus patients in Qatar. Nigerian Journal of Clinical Practice.2014; 17(5): 565- 568.
- 35- Sommer I, Griebler U, Mahlknecht P, Thaler K, Bouskill K, Gartlehner G, et al. Socioeconomic inequalities in noncommunicable diseases and their risk factors: an overview of systematic reviews. BMC Public Health. 2015;15:914
- Chiwanga, FS., et al. Urban and rural prevalence of diabetes and pre-diabetes and risk factors associated with diabetes in Tanzania and Uganda. Global health action, 2016, vol. 9, no 1, p. 31440.
- Hsu CC, Lee CH, Wahlqvist ML, Huang HL, Chang HY, Chen L, et al. Poverty increases type 2 diabetes incidence and inequality of care despite universal health coverage. Diabetes Care. 2012;35:2286–92.
- Kyrou I, Tsigos C, Mavrogianni C. et al. Sociodemographic and lifestyle-related risk factors for identifying vulnerable groups for type 2 diabetes: a narrative review with emphasis on data from Europe. BMC Endocr Disord 20 (Suppl 1), 134 (2020). https://doi.org/10.1186/s12902-019-0463-3
- Weisman A, Fazli GS, Johns A, Booth GL. Evolving Trends in the Epidemiology, Risk Factors, and Prevention of Type 2 Diabetes: A Review. Can J Cardiol. 2018 May;34(5):552-564. doi: 10.1016/j.cjca.2018.03.002. Epub 2018 Mar 13. PMID: 29731019.
- Agardh E, et al. Type 2 diabetes incidence and socio-economic position: a systematic review and meta-analysis. International journal of epidemiology, 2011, vol. 40, no 3, p. 804-818.
- Zheng Y, Ley Sylvia H, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nature reviews endocrinology, 2018, vol. 14, no 2, p. 88-98.
- Lima LR. de, et al. Quality of life and time since diagnosis of diabetes mellitus among the elderly. Revista Brasileira de Geriatria e Gerontologia, 2018, vol. 21, p. 176-185.
- Sacomboio ENM. ABO/Rh Blood Groups and Chronic Diseases in Angolan Patients. Am J Biomed Sci & Res. 2021 - 13(1). AJBSR.MS.ID.001834. doi: 10.34297/ AJBSR.2021.13.001834.
- Sacomboio ENM, Neto CR, Hungulo OFS, Ekundi-ValentimE. Blood Group (ABO/Rh) and Clinical Conditions Common in Children with Nephrotic Syndrome and Sickle Cell Anemia in Angola. J Blood Disord Med. 2021; 4(1): dx.doi. org/10.16966/2471-5026.128.
- Sacomboio E, Sebastião D, Sacomboio-Filho F. Sickle Cell Trait and Blood Groups (ABO and Rh) in Angolans Submitted to Hemoglobin Electrophoresis. Hematol Oncol Curr Res. 2020; 2(1): 1004.