
Biomedical Science and Clinical Research(BSCR)
ISSN: 2835-7914 | DOI: 10.33140/BSCR
Impact Factor: 1.7


Research Article - (2025) Volume 4, Issue 4
Exercise Associated Collapse and Death in Thoroughbred Racehorses: A Mechanistic Argument for Heat Stroke as the Silent Killer
Received Date: Sep 05, 2025 / Accepted Date: Oct 08, 2025 / Published Date: Oct 17, 2025
Copyright: ©©2025 Meg Brownlow. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Brownlow, M. (2025). Exercise Associated Collapse and Death in Thoroughbred Racehorses: A Mechanistic Argument for Heat Stroke as the Silent Killer. Biomed Sci Clin Res, 4(4), 01-11.
Abstract
For some decades, cases of acute collapse followed by death during or shortly after racing have been attributed to ‘acute heart failure’, the premise being that an underlying cardiac abnormality becomes activated during strenuous exercise, triggering a lethal arrythmia which causes collapse and death. This has been acknowledged as a speculative diagnosis, because affected horses have not been examined at the point of collapse or during their demise, and in the majority of cases a thorough post mortem examination does not provide a definitive diagnosis of cardiac pathology.
In a recent editorial penned by a special interest group of veterinarians, the Exercise-Associated Sudden Death (EASD) condition was discussed at length, but there was no reference to the effect of adverse environmental conditions or heat shock/stroke as the possible cause or even a risk factor.
The reader may at this point be wondering how a racehorse could be affected by heat shock/stroke so quickly as to cause death in a matter of minutes during racing. The most important point to appreciate is the extreme quantity of metabolic heat produced when a racehorse performs strenuous exercise. This has been estimated at approximately 30 times the resting rate, and because only 20% is used for the exercise activity, 80% represents excess waste heat, which rapidly causes core body temperature to rise to a critical level if it is not dissipated to the environment.
It has been shown that the maximum rate of heat loss in any exercising animal is determined by three factors: (1) the capacity of heat loss mechanisms; for racehorses, a powerful sweating ability, (2) the cooling power of the environment, which dictates the degree of thermal strain and its CVS response, and finally, (3) the internal mechanisms which enable the transportation of heated blood from exercising muscles to the body surface.
Why do relatively few racehorses succumb to heat shock/stroke? The answer would appear to involve individual susceptibility; in this respect, all the horses arriving at the barriers may not be equal. A dysfunction in one of the abovementioned systems may predispose to a minor heat illness episode, but changes to all three could result in thermoregulatory failure, causing collapse and death. Another predisposing factor has recently been identified. Intestinal hypoperfusion from the exercise-associated reduction in blood supply has been shown to cause leakage of endotoxin into the central circulation. It has been demonstrated that under certain circumstances this may initiate a systemic inflammatory cascade, which perpetuates a positive feedback loop, driving continuous levels of endotoxin and cytokine production, and further activating systemic inflammation. This can become a key driver of the heat shock/stroke condition to its end stage, characterized by tissue necrosis, disseminated coagulation, and organ failure. The fact that this can be independent of hyperthermia means that an elevated temperature cannot be relied upon for its diagnosis.
This article is intended to challenge the ‘acute heart failure’ explanation in favour of another, also arguably a speculative diagnosis, in which heat shock/stroke may be responsible for many of these incidents, with circulatory failure as the mechanism of action. Such a change in diagnosis brings significant alterations to preventative strategies and a totally different clinical perspective to welfare implications for the TB racehorse.
Introduction
This article is not a review of the literature concerning exercise- associated sudden death (EASD) in TB horses, but instead presents a possible mechanistic insight into how and why heat shock may occur and indeed be causal. As the world warms due to climate change, it is obvious that if some cases of EASD are indeed due to heat shock, they are going to increase in frequency and become a significant welfare issue, unless racing veterinarians recognize their origin and take timely action to initiate appropriate preventative strategies.
There have been numerous articles concerning EASD in TB racehorses and most recently, an editorial penned by a special interest group was published in the Equine Veterinary Journal (Colgate: Editorial, November 2025, 57, 296-302.). This article pointed out the need for greater understanding of the condition and identification of risk factors associated with its occurrence. The aspect that drew the attention of this author was that there was no mention of the possible effect of adverse environmental conditions and the role of heat shock/stroke as a predisposing factor to the condition, or indeed as the possible cause.
EASDs have been documented in other athletic species, in human subjects, affecting both elite and recreational athletes, military personnel in training and deployment, and in the racing Greyhound [1-3]. This author has observed cases of exertional heat illness (EHI) and heat shock (HS) at the racetrack for some 20 years and documented the condition extensively [4, 10]. The more common form of heat illness, referred to as Exertional Heat Illness (EHI), is most commonly observed in the post-race period, with horses demonstrating central nervous system dysfunction (CNS) and varying levels of ataxia and disorientation, but there have also been at least four clinical cases of the more serious form, referred to as heat shock, during the author’s time as an on-course veterinarian (OTV), where the animal has returned to the enclosure on the verge of demise. In these horses there has been no detectable arrythmia, but instead signs of circulatory failure, with brick-red congested mucous membranes and slow capillary refill times. Treatment as for heat-affected horses was effective in saving these animals, but there may be other horses with such symptoms who go undetected or misdiagnosed, collapse and die.
Thoroughbred racehorses are superlative athletes, capable of galloping at speeds up to 65 km/hour. The inherent danger, however, is their very high rate of exercise-associated metabolic heat production (MHP), determined by both the intensity and duration of the specific exercise activity. Jessen [11]. estimated that the maximum metabolic rate in horses was in the order of 30 times that of their resting rate, compared to only 20 times in highly trained human athletes.
A negative consequence of such high levels of MHP in horses is that at least 80% is associated with the production of waste heat, which can pose serious problems if it is not discarded quickly and efficiently to the environment. The view of this author is that cases of collapse and sudden death at the racecourse could result from end-stage heat shock/stroke events which present like ‘acute heart failure’. The accuracy of the diagnosis is important because preventative strategies for each are quite different, and unfortunately, the lack of an elevated temperature does not rule out a heat-related diagnosis. As articulated by Hodgson [12] increases in core temperature often lag behind increases in muscle temperature, with rectal temperature the last to rise.
A mechanistic insight into collapse and death due to heat shock centres on heat loss mechanisms and their potential to become dysfunctional. It is possible for one system, even two, to fail without consequences, but if all three fail the animal faces a perilous situation.
The Maximum Rate of Heat Loss is Determined by Three Factors
The Cooling Power of the Environment
The environmental conditions prevailing when horses succumb to a heat shock episode are most likely to be those that cause a substantial level of ‘thermal strain’. From an epidemiological study, it was identified that the most dangerous weather conditions combined high levels of humidity (vapour pressure) with low or negligible wind speed. This type of environmental stress creates the greatest level of thermal strain because sweat cannot evaporate but remains on the skin surface or drips off the body without cooling the animal [6, 10]. It is important to note that in some situations, high levels of thermal strain, copious sweating, and loss of blood flow to the skin can begin before any exercise activity takes place and are largely dependent on the ambient environmental conditions and excitability of the individual animal. Figure 1 illustrates the effects of cardiac redistribution on a horse's whole-body blood flow, but it does not capture the dynamic changes as an individual transitions from rest to strenuous exercise, and then to the recovery stage. It needs to be emphasized that this process is constantly changing in response to prioritization of demand, sometimes having no adverse consequences but at other times quite the opposite. Thus, the circulatory system is closely associated with the thermoregulatory failure associated with heat shock/stroke.

Figure 1: Phases of cardiac redistribution or adjustments to blood flow with the various physiological stages of rest, maximum exercise, and recovery; and when there might be a maldistribution of blood flow, where blood is sequestered in the skin and becomes unavailable, causing circulatory failure, heat shock and death. Note that the phase borders are not discrete, but merge dynamically one into the other
The Capacity of Heat Loss Mechanisms is Affected by the Individuals Thermo Effector Physiological Determinants
The author has created an epidemiological triad as a model of disease causation for EHI/HS, to show how the condition might develop through the interaction of the three key factors: the agent (strenuous exercise) which elevates core body temperature to critical levels, the host, and the environment (see Figure 2). The ‘multiple hit hypothesis” suggested by Laitano [1] describes the interaction of certain environmental conditions with multiple intrinsic risk factors to create a ‘perfect storm’ for disease occurrence (see Figure 3).

Figure 2: The epidemiological triad traditionally used to illustrate relationships between infectious agent, host, and environment for diseases, but used here for heat shock/stroke to show the relationships between the agent (strenuous exercise) which acts as the causal agent for metabolic heat production, and the contributing effects of environmental and host risk factors, which might contribute to disease occurrence
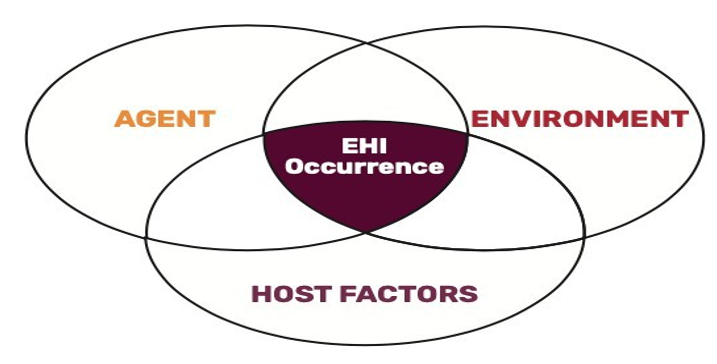
Figure 3: Multiple-hit hypothesis. This figure shows how a case of heat shock/stroke might involve multiple factors that come together to cause a ‘perfect storm’ and result in a heat shock episode [1, 2].
One of the most important findings of the epidemiological study performed by Brownlow and Brotherhood [6] was that environmental conditions could not explain the occurrence of all post-race EHI cases, and in fact only 48% were accounted for by the environment. Recent investigations into cases of EHI/HS in human subjects have also shown a greater relevance of intrinsic host factors to the occurrence of HS episodes. In TB racehorses it has been found that lack of acclimatization, lack of fitness, significant levels of hypo-hydration and immune dysfunction were important predisposing risk factors, and these have also been implicated experimentally [12-15].
The Efficiency of Internal Heat Transfer from the Exercising Muscles to the Body Surface: The Redistribution of Cardiac Output
It was Carl Jessen [11], a renowned thermal physiologist, who wrote that the most serious challenge to the cardiovascular system of any athletic species is strenuous exercise in the heat, which he likened to a situation of acute haemorrhage. Initially, blood flow prioritizes working muscle, but then as the heat load escalates, thermoregulatory requirements become important. There are increases to skin blood flow, which, depending upon host and environmental factors, can mean that a substantial proportion of the finite blood volume becomes sequestered in the skin, and effectively unavailable to the general circulation (see Figure 1).
The Redistribution of Blood Volume as a Normal Physio- logical Response
The redistribution of blood flow occurs as a physiological response to the competing demands for the musculoskeletal system, critical organ perfusion, and thermoregulation. Some vascular regions, such as the gastrointestinal and renal portions, are subjected to reductions in their blood supply and ‘lend’ part of that blood flow to other regions. If these redistributive mechanisms are overwhelmed, however, the shift of blood volume to the skin may exceed regional compensations; heat dissipation becomes ineffective because total blood flow is reduced, and core body temperature continues to rise. The problem that may emerge is that the heart’s output reaches its upper limit, with adverse consequences to all cardiac indices, so that cardiac filling pressure, arterial pressure, and stroke volume are all diminished. The only way that the systemic circulation can maintain an adequate blood flow is to increase heart rate, which must rise to maximal levels to meet requirements.
If Compensatory CVS Adjustments Fail, There is a Maldistribution of Cardiac Output, which Represents the Tip- ping Point for Circulatory Failure
When compensatory adjustments fail, the individual can no longer maintain blood flow and circulatory collapse ensues. This is referred to as a Maldistributive defect (see Figure 4) and is associated with a hypovolemic state which is characterized by venous vasodilation and peripheral pooling. Cardiac function continues to diminish and at this stage, the heart itself is subjected to low flow. Myocardial ischemia may occur, resulting in lethal arrythmias and conduction disturbances [16]. Collapse due to heat shock/stroke and sudden death may follow.

Figure 4: Diagrammatic representation of the maldistribution of cardiac output associated with high levels of thermal strain, which may be experienced in horses racing in hot and humid conditions. There is increased blood flow to the skin for heat dissipation, and although blood flow to exercising muscle is maintained, that to the liver, kidney, and gastrointestinal tract is reduced. The result is that CVS redistributions or adjustments must take over to maintain vital cardiac pressures and central blood volume. If these do not occur, there will be circulatory failure, and the horse may collapse and die suddenly of a heat shock/stroke event. Note the extreme distension in the saphenous vein on the medial side of the horse’s hind leg in the accompanying figure.
An Additional Pathway, Driven by Endotoxemia, Contributing to End-Stage Heat Stroke, Collapse and Death
Most recently, an exercise-induced gastrointestinal syndrome (EIGS) has been identified as possibly one of the most important host risk factors for end-stage heat stroke in human subjects (see Figure 5 and 6) [17, 19]. The presence of the EIGS pathway has also been documented to occur in horses [9].

Figure 5: General diagram of the pathophysiological pathway for exertional heat illness in the TB racehorses showing the relationshipsbetween the heat toxicity and endotoxemic pathway, and their final end point, to heat stroke and sepsis

Figure 6: Shows that strenuous exercise and thermal strain from heat stress conditions can produce a rise in core body temperature, which causes injury to the GIT and a redistribution of cardiac output to other areas which are prioritized when exercising. This can result in changes to the permeability of the intestinal cells, which become ‘leaky’, allowing endotoxin (LPS) to gain access to the central circulation. If the individual animal has a good immune system, LPS is deactivated, and exercise can continue without consequence. This is referred to as a ‘heat tolerant state’. If on the other hand, if there is immune dysfunction, LPS readily gains access to the central circulation and is not deactivated. The individual is predisposed to EHI states and is described as ‘heat intolerant’. When LPS is active in the central circulation and reaches a critical level, it triggers the SIRS and cytokine proliferation, which have adverse downstream consequences such as coagulopathies, multi-organ damage and death
McConaghy [20, 21]. demonstrated that there was an exercise- as-sociated GIT hypoperfusion, which caused the intestinal cells to become ‘leaky’ and allowed endotoxin to gain access to the sys-temic circulation.
Baker et al [22]. confirmed that in active racehorses, translocation of endotoxin occurred through a ‘leaky’ bowel into the systemic circulation and was a normal response to strenuous exercise. It was also established that there was a unique relationship between LPS and anti-LPS antibody, where the latter could deactivate excess amounts of LPS, so that there were no harmful effects. The anti-LPS function was regarded as part of a functioning immune system. In a seminal study, Donovan [23]. showed that strenuous exercise on a high-speed treadmill to absolute fatigue induced not only substantial levels of endotoxemia but also a systemic pro-inflammatory cytokine response, which lasted in the systemic circulation in that study for up to 2 hours.
It has been emphasized by most researchers in human subjects that the EIGS pathway should not be underestimated in its contribution to heat stroke occurrence, changes to the intestinal mucosa causing the ‘leaky bowel’ syndrome could last for up to 24 hours in human subjects [24, 28]. From the work of Baker, it is apparent that the individual racehorse’s immune system is critical for clearance of endotoxin from the circulation and that there would be individual variability in that response. There are many circumstances that can lead to immune dysfunction in racehorses; for instance, upper respiratory tract infections in horses in training, inflammatory musculoskeletal disorders, recent GIT illnesses such as colic, or even sleep deprivation [29].
Discussion
The author is suggesting a new pathophysiological approach for EASD cases, one that does not strictly adhere to the acute heart failure paradigm. It is argued that some cases of sudden collapse and death may be a result of circulatory failure, due to an inability to sustain strenuous exercise when there are conditions of thermal strain, dysfunction of thermoregulatory mechanisms, and the maldistributive effects on total blood flow. Subsequent myocardial ischemia causes lethal arrythmias and conduction disturbances, followed by heart failure, shock, collapse and death. Heart failure is therefore a secondary manifestation of a heat- related condition.
Death Due to Heat Shock/Stroke Does not Produce any Post Mortem Abnormalities that Distinguish it from Acute Heart Failure
One of the major problems in making a diagnosis of heat shock/ stroke is that at post mortem examination it is almost impossible to differentiate between cases of acute heart attack and heat shock. Pathological findings in cases of acute heat toxicity may include hepatocellular necrosis, DIC, and intrathoracic haemorrhages, but histological changes may not be immediately apparent if the onset and demise associated with a heat shock event is rapid, and it has been shown that a human patient must survive for at least 6 hours for the abnormalities to evolve [30, 33].
The Superimposition of the Exercise-Induced Gastrointesti¬nal Syndrome Necessitates a New Case Definition for EASD, Which Includes Horses that do not Die Immediately but Some-time Later from Terminal Sepsis and MOD
There are also difficulties in the differentiation of heat stroke sepsis and septic shock due to other agents. Researchers in the field have suggested that sepsis cannot be viewed as a specific illness but rather a syndrome that encompasses an uncertain pathobiology. Both septic shock and that due to the EIGS syndrome will exhibit a similar inflammatory response. In the latter however, once endotoxin activates the SIRS it perpetuates a positive feedback loop, driving continuous cytokine production and resulting in the exacerbation of inflammation, coagulopathies and multi¬organ damage. This can progress to a multi-system illness with terminal sepsis, indistinguishable from that due to other infectious agents. Death can be over a protracted period, and it is this time lapse between the primary thermal insult (strenuous exercise) and the animal’s death sometime later that creates confusion with the diagnosis. The development of MOD due to heat stroke is characterized by inflammation, tissue necrosis and coagulopathies, with the liver, lung, and kidney as the major target organs [30-33].
Change of Focus by Some Members of the Medical Profession from Acute Cardiac Failure to Heat (Stroke) in Cases of Exercise- Associated Sudden Death
Recently, some members of the medical profession working in the field at sporting events have stepped back from a speculative diagnosis of primary heart failure to explain sudden deaths, and have asked the question, “Is heat stroke more prevalent than an arrhythmic death?” [34]. These authors maintain that several lines of evidence indicate that the hazards of heat stroke during sport are under-appreciated and under-diagnosed. They concluded from their study involving 137,580 athletes participating in endurance sports, that fatal or life-threatening events were caused almost exclusively by heat (stroke) and that serious cardiac events were extremely rare and outnumbered by heat stroke events by a factor of 10.
The Importance of Having Infrastructure for Cooling on Hand and the Ability to Perform Whole Body Cooling Strategies Even if the OTV is Unsure of a Heat Shock/Stroke Diagnosis
When working at the racetrack, it is important to be prepared for a situation where a horse is on the verge of collapse, but where a diagnosis of either heart failure or heat shock is not definitive. It is the author’s opinion that whole-body cooling may be a crucial lifesaving intervention if performed immediately, but this necessitates access to infrastructure such as a mobile cooling device that can go anywhere on track at a moment’s notice.
Whole-body cooling has been shown to perform three critical tasks in cases of heat shock. Firstly, it can rapidly reduce organ and tissue temperatures. Secondly, it redirects blood sequestered in the skin by causing cutaneous vasoconstriction, and most importantly, re- establishes the pathway for cooling by reversing maldistributive effects, allowing ‘hot’ blood to flow from deeper tissues to the skin surface. Finally, by normalizing cardiac output, it supports the central circulation, improving cardiac indices and blood pressure regulation. Whilst the author also uses other medications as previously described, whole-body cooling in the first instance in such situations can be lifesaving. As articulated by Armstrong a highly respected authority on heat illness states and a prolific writer in the field, “heat shock/stroke treatment is a battle against endotoxemia that is won by rapid whole-body cooling and likely lost if that cooling is delayed” [35].
Suggested Preventative Strategies A Change of Focus is Required to Address the Importance of the Intestinal Microbiome (IM) as a Key Factor in the Aetiology of Heat Shock/Stroke Episodes
From the seminal work of Armstrong [34] it has been recognized that the intestinal microbiome has assumed a new relevance as a predisposing factor for heat shock/stroke episodes. This, together with the fact that racehorses have been shown to have similar exercise and hyperthermia-induced increases to intestinal permeability, allowing leakage of endotoxin into the central circulation and perpetuating the SIRS and cytokine proliferation cycle, which potentially drives a heat stroke episode as described in human athletes, allowing leakage of endotoxin into the central circulation is especially important.
Researchers have documented a multitude of factors which can act to alter the IM ecosystem to further increase intestinal permeability. These include any pre-existing illness or fever, antibiotic and/or non-steroidal anti-inflammatory administration, gastroenteritis (especially diarrhoea), poor cardiovascular fitness, sleep deprivation, lack of acclimatization, poor diet, and dehydration. Although these factors have been cited before in a general sense, it is their unique relationship to the IM that gives them a greater relevance here.
Beginning with the premise that preserving or restoring the integrity of the intestinal barrier by preventing the ‘leaky’ transfer of LPS from the intestine to the general circulation is essential to block the progression to heat shock/stroke episodes, some form of treatment to the IM is a logical step. It is further suggested, however, that some horses that collapse and die during or shortly after their racing have multiple issues, that may be ill-defined, which predispose them to EASD.
Probiotic Supplements as a Preventative Strategy
An exciting new development in this sphere comes from the work of Jacobs and colleagues [36]. who have performed first-phase trials on the use of a probiotic supplement, Bacillus coagulans GBI-30 6086,* ‘top-dressed’ on an individual horse’s feed ration. Horses were then subjected to an exercise challenge, and it was found that various markers of exercise-induced inflammation were reduced. It was hypothesized that this specific probiotic imparted an effect on the gut barrier through a direct interaction with enterocytes, decreasing their permeability Preliminary investigations suggest its routine use may attenuate post-exercise inflammation in racehorses [37].
Kerry Group Kwang Bangna Khet Bangnai Bangkok 10260/ Thailand Others have used Beta-Glucan **, a cell wall component of fungi and yeasts, to supplement diets in horses injected with E. coli lipopolysaccharides [38]. They found that in clinical trials this specific polymer had an immunomodulatory action that was able to modify the response to pro-inflammatory stimuli or even that of sepsis, and could potentially be useful in the control of endotoxemia in horses. This product might also be extremely useful in preserving the integrity of the intestinal barrier in TB racehorses. ** beta glucans from Saccharomyces cerevisiae at a dose of 10mg/kg/day orally
Planning and Education Might be Able Reduce Heat Shock/ Stroke Morbidity and Mortality
In the author’s opinion most cases of heat shock/stroke are associated with conditions of thermal strain and a relative failure of thermoregulation due to a combination of certain intrinsic risk factors. Knowing this, efforts to reduce episodes revolve around awareness and prevention. OTVs need to understand the nature and type of predisposing factors that might be responsible and be able to recognize early warning signs. In consultation with trainers, it may be recommended that an individual animal has an exercise and work intensity limit in accordance with its present level of fitness and acclimatization. The finding by Lambert and others [17], that after a strenuous exercise episode the bowel in human athletes may be ‘leaky’ for some 24 hours, may indicate that a longer time interval exists for endotoxemia to accumulate in the circulation and exert its SIRS-inducing effect. As previously cited from the priority in treating heat shock/stroke is the battle against endotoxemia, and this defines the primary preventative objective.
Recommended Development of Strategies to Detect Risk of Heat Shock: The Need to Target Horses After a ‘Hard Run’ or Prior to Racing
1. Routine blood profiling 24 hours before racing to detect evidence of immune dysfunction.
2. Blood endotoxin assay after last run.
3. Biomarkers of multiorgan injury from the last run. These include Alanine Transaminase (ALT - liver), Creatine Kinase (CK - skeletal muscle), Blood Urea Nitrogen (BUN - kidney), intestinal FABP2, a plasma biomarker of intestinal injury [39].
4. Trainer-centred fitness assessment (for discussion).
5. Trainer-centred acclimatization assessment (for discussion).
6. Veterinarian-centred hydration assessment, including blood profiling and specifically plasma osmolality [40].
7. Trial into the use of a specific probiotic, Bacillus Coagulans (4 billion Bacillus coagulans GBI-30, 6086 Kerry Group, County Kerry, Ireland), as a feed supplement to attenuate post-exercise inflammation in horses [36].
8. Trial into use of Beta-Glucan supplementation (purified B-1,3/1,6- glucan extracted from the cell wall of brewer’s yeast Saccharomyces cerevisiae 10mg.kg orally) to protect against endotoxemia [38].
9. Experimental trial on the use of pre-race cooling strategies adapted from and the effect on the incidence of heat stroke/ stroke [41].
Conclusion
From the author’s viewpoint, whenever horses collapse and die suddenly, either during a race, a short time later, or indeed some days later, the causation may be a heat shock/stroke episode. The longer time frame scenario is complicated by the presence of endotoxemia, sepsis, and multiple organ damage, and the time difference between the initial strenuous exercise thermal insult and death creates a clinical disconnect, which causes confusion and misdiagnosis; nevertheless, the probability of its causality must be considered.
In racehorses, it is the very high level of metabolic heat production which endangers their thermoregulatory system, and exercise in the heat represents the ultimate challenge. Studies have shown that intrinsic risk factors are probably more important than those of the environment, and most recently the intestinal microbiome has been identified as a most important predisposing factor. It is suggested that heat shock is the insidious ‘silent killer’ in some or all of these sudden death cases. Becoming familiar with its pathophysiology and understanding its mechanism brings us closer to successful management.
It is also important to address the geographical context. Those locations where the environment is already characterized by warm weather and high levels of humidity will have a higher incidence of the condition as the climate gets hotter and wetter. Racing jurisdictions should be proactive and put in place mobile cooling devices, able to be used anywhere on track and within race-day enclosures. Where racing takes place in cooler climates with a low incidence of heat-related events, organisers should be prepared for an increase in their occurrence, as described above.
References
- Laitano, O., Leon, L.R., Roberts, W.O,. & Sawka, M.N. (2019). Controversies in Exertional Heat Stroke diagnosis, prevention andtreatment. Journal Applied Physiology, 127, 1338-1348.
- Garcia, C.K., Renteria, L.L., Leite_Santos, G,. Leon, L.R.& Laitano, O. (2022). Exertional heat stroke: pathophysiology and riskfactors. BMJ Medicine, 1e000239.
- Karamatic S.L., Anderson, G.A., Parry, B.W., Slocombe, R.R.& Mansfield, C.S. (2018). Prevalence and risk factors for medical events following exercise at Australian Greyhound race meetings. Australian Veterinary Journal, 96,4,120-126.
- Brownlow, M.A., Dart, A.J,. & Jeffcott, L.B. (2016). Exertional Heat Illness: a review of the syndrome affecting racing Thoroughbreds in hot and humid climates. Australian Veterinary Journal, 94, 240-247.
- Brownlow, M.A., & Mizzi, X.A. (2020). Thermoregulatory capacity of the Thoroughbred racehorse and its relationship to the pathogenesis of exertional heat illness. Equine Veterinary Education, 34, 4,214-221.
- Brownlow, M.A., & Brotherhood, J.M. (2021). An investigation into environmental variables influencing post-race exertional heat illness in thoroughbred racehorses in temperate eastern Australia. Australian Veterinary Journal,99, 433–481.
- Brownlow, M.A., & Mizzi, X.A. (2021). Exertional heat illness in Thoroughbred racehorses: pathophysiology, case definition and treatment rationale. Equine Veterinary Education, 34,5, 259–271.
- Brownlow, M.A., & Mizzi, X.A. (2022a). Epidemiology of exertional heat illness in Thoroughbred racehorses in temperate eastern Australia; the role of extrinsic (environmental) factors in disease causation. Equine Veterinary Education, 34,12, 660–672.
- Brownlow, M.A., & Mizzi, X.A. (2022b). Perspective Article: Pathophysiology of exertional heat illness in the Thoroughbred racehorse: broadening perspective to include an exercise induced gastrointestinal syndrome in which endotoxemia and systemic inflammation may contribute to the condition. Equine Veterinary Education, 00.1-10.
- 10.Brownlow, M.A., & Mizzi, X.A. (2023). An overview of exertional heat illness in Thoroughbred racehorses: pathophysiology, diagnosis and treatment rationale. Animals, 13, 610.
- Jessen, C. (Ed.) (2000). Pathophysiology of Temperature Regulation: Hyperthermia and Heat Stroke. In: Temperature Regulation in Humans and Other Mammals. New York: Springer-Verlag, pp.16–164.
- Hodgson, D.R,. Davis, R.E., & McConaghy, F.F. (1999). Thermoregulation in the horse in response to exercise. British Veterinary Journal 150:219– 220.
- Geor, R., & McCutcheon, L.J. (1998). Hydration effects on physiological strain of horses during exercise-heat stress. Canadian Journal Applied Physiology, 84, 2042-2051.
- Geor, R.J., McCutcheon, L.J. & Ecker, G.L. (2000). Heat storage in horses during submaximal exercise before and after humid heat acclimation. Journal Applied Physiology, 89, 2283-2293.
- Marlin, D.J., Scott, C.M., Schroter, R.C., Harris, R.C., Harris, P.A., Roberts, C.A. & Mills, P.C. (1999). Physiological responses of horses to a treadmill simulated speed and endurance test in high heat and humidity before and after heat acclimation. Equine Veterinary Journal, 31, 31-42.
- Baker, B., Gaffin, S.L., Marchand,M., & GI.,K. (2022). The cardiovascular system in heat stroke. CJC Open, 4(2), 158-163.
- Lambert, G.P., Gisolfi, C.V., Nyberg, D.J., Moseley, P.L., Oberley, L.N., & Kregal, K.C. (2002). Hyperthermia-induced intestinal permeability and the role of oxidative and nitrosative stress. Journal Applied Physiology, 92, 1750–1762.
- Lambert, G.P (2004). Role of gastrointestinal permeability in exertional heatstroke. Exercise Sports Science Reviews, 32,185-190.
- Lambert, G.P. (2008). Intestinal barrier dysfunction, endotoxemia and gastrointestinal symptoms: the canary in the coal mine during exercise- heat stress? In: Marino, F.E. (Ed.) Thermoregulation and Human Performance. Physiological and Biological Aspects. Basel Switzerland: Karger, pp. 61–73.
- McConaghy, F.F., Hales, J.R.S., & Hodgson, D.R. (1997). Cardiovascular responses to heat and exercise in horses.Annals of the New York Academy of Sciences, 813,1, 600–603.
- McConaghy, F.F., Hodgson, D.R., Rose, R.J., & Hales, J.R.S. (1996). Redistribution of cardiac output in response to heat exposure in the pony. Equine Veterinary Journal, 28,S22, 42–46.
- Baker, B., Gaffin, S.L., Wells, M., Wessels, B.C. & Brock-Utne, J.G. (1988). Endotoxemia in racehorses following exertion. Journal of South African Veterinary Association, 59 (2), 63–66.
- Donovan, D.C., Jackson, C.A., Colahan, P.T., Norton, N., & Hurley, D. (2007). Exercise-induced alterations in pro-inflammatory cytokines and prostaglandin F2alpha in horses. Veterinary Immunology and Immunopathology, 118, 3–4,263–269.
- Bouchama, A., & Knochel J.P. (2002). Heat Stroke. New England Journal Medicine, 346, 1978-1988.
- Leon, L.R. (2007). Heat stroke and cytokines. Progress Brain Research, 162, 481-524.
- Lim, C.T., & MacKinnon L.T., (2006). The role of exercise-induced immune system disturbances in the pathology of heat stroke. The dual pathway model of heat stroke. Sports Medicine, 36, 39-64.
- Lim, C.L. (2018). Heat sepsis precedes heat toxicity in the pathophysiology of heat stroke – a new paradigm on an ancient disease. Antioxidants, 7, 149-167.
- Lim, C.L., & Suzuki, K. (2016). Systemic inflammation mediates the effects of endotoxemia in the mechanisms of heat stroke. Biological Medicine, 9, 1,1-4.
- Perkins, N.R., Reid, S.W.J., & Morris, R.S. (2005). Profiling the New Zealand Thoroughbred Racing Industry 2: Conditions interfering the training and racing. New Zealand Veterinary Journal, 53,1,69-76.
- Li, Ruilong., Guo, D.,, I, T., Hu., P, & Xu. T., (2024). Progress in heat stroke-induced multiple organ damage. Perioperative Precision Medicine, 2,3, 73-79.
- Iba. T., Kondo, Y., Maier, C.L., Helms, J., Ferrer,R., & Levy JH. (2025). Impact of hyper- and hypothermia on cellular and whole body physiology. Journal Intensive Care 13: 4.
- Iba, T., Helms,J., Levi, M., & Levy, J.H. (2023). Inflammation, coagulation and cellular injury in heat-induced shock. Inflammation Research, 72,(3) 463-473.
- Iba, T., Connors, J.M., Levi, M., & Levy, J.H. (2022). Heatstroke-induced coagulopathy: Biomarkers, mechanistic insights and patient management. eClinical Medicine, 44,101276.
- Yanklelson, L., Sadeh,B., Gershovitz L., Werthein, J., Heller, K., Halpern, P & Viskin, S. (2014). Life threatening events during endurance sports. Is heat stroke more prevalent than arrhythmic death?. Journal American College Cardiology, 64,5,463- 469.
- Armstrong, L.E., Lee, E.C, & Armstrong E.M. (2018). Interactions of Gut Microbiota, Endotoxemia, Immune Function, and Diet in Exertional heatstroke. Journal Sports Medicine, Article ID 5724575, 1-33.
- Jacobs, R.D., Grum, D., Trible. B., Ayala, D.I., Kamezos, T.P., & Gordon, M.E. (2024). Oral probiotic administration attenuates post exercise inflammation in horses. Translational Animal Science 8,txae124.
- Azard, M.A.K., Sarker, M., & Wan, D. (2018). Immunomodulatory effects of probiotics on cytokine profiles. Biomedical Research International. 8063647.
- Lacerenza , M.D., Arantes, J.S., Reginato, G.M., & Passarelli,D. (2024). Effects of B-Glucan Supplementation on LPS-Induced Endotoxemia in Horses. Animals, 14,474.
- KIng, M.A.,Leon, L.R., Mustico, Haines, J.M., & Clanton,T.L. (2015). Biomarkers in multiorgan injury in a preclinical model of exertional heat stroke. Journal Applied Physiology,118,1207-1220.
- Brownlow, M.A., & Hutchins, D.R. (1982). The concept of osmolality: its use in the evaluation of ‘dehydration’ in the horse. Equine Veterinary Journal, 106-110.
- Ohmura, H., Ebisuda, Y., Takahashi, Y., & Mkai, K. (2025). Effects of pre-exercise cooling in hot environments on performance and physiological responses in Thoroughbred horses. Journal Equine Science, 36,1. 19-23.