
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2019) Volume 4, Issue 2
Endometrial Carcinoma staging Issues Laparotomy versus Laparoscopic Approach which is More Feasible and Safer?
2Department of Pathology, Faculty of Medicine Zagazig University. Zagazig, Egypt
3Department of General Surgery, Faculty of Medicine - Zagazig University. Zagazig, Egypt
Received Date: May 19, 2019 / Accepted Date: May 31, 2019 / Published Date: Jun 12, 2019
Copyright: ©Walid Mohamed Elnagar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Surgical staging of endometrial cancer is considered one of the main pathways for managing those categories of cases. Uterine cancers are considered a challenging surgical scenario in many situations due to anatomical changes in tissue planes and metastatic disease besides the presence of obesity in many cases requiring management.
Aim: To compare laparoscopy versus laparotomy for complete uterine cancer surgical staging.
Methodology: Cases having clinical stage I to IIA endometrial carcinoma have been randomly allocated to laparoscopy or open laparotomy including hysterectomy, salpingo - oophorectomy, pelvic cytology, pelvic and para-aortic lymphadenectomy. The chief research study outcomes were the 6-week morbidity, mortality issues, hospitalization period and conversion rates from laparoscopy to laparotomy.
Results: There was no statistical significant difference as regards the Surgical stage, tumor type, types and numbers of nodes of the studied research groups in which there was no statistical significant difference as regards surgical staging, tumor type observed, peritoneal cytology, type of nodes, no nodes, Para aortic nodes only, pelvic nodes only, both pelvic and para - aortic nodes, any pelvic node, no. of nodes median (IQR) values = 0.996, 0.998, 0.929, 0.607, 0.928, 0.669, 0.541, 0.562, 0.680, 0.934 consecutively.
Conclusions and recommendations: The current research elucidates the privilege of laparoscopic surgical staging for early stage endometrial cancer, however future research studies are required to be performed in multi centric fashion and to put in consideration variability’s in BMI, coexisting medical morbidities e.g. DM, hypertension besides the racial and ethnic differences.
Introduction
Uterine malignancies are one of the common issues faced by gynecological oncologists that require multidisciplinary management as it is frequently diagnosed in presence of coexisting medical morbidities such as obesity, DM and hypertensive diseases. Surgical staging of endometrial cancer is considered one of the main pathways for managing those categories of cases. Uterine cancers are considered a challenging surgical scenario in many situations due to anatomical changes in tissue planes and metastatic disease besides the presence of obesity in many cases requiring management [1,2]. Laparoscopic gynecological practice is becoming a growing trend in practice. Implementing operative gynecological procedures could enhance the survival rates of patients and reduce morbidity issue in various aspects, however open approaches are sometimes required in complicated cases with advanced disease stages and extensive tissue adhesions affecting normal anatomical tissue planes. The requirement of comparing and contrasting between open and laparoscopic approaches is becoming a growing research issue all over the globe particularly in gynecological oncological practice however laparoscopic management and staging of endometrial cancer requires skillful laparoscopists that is not always feasible in all oncological centers [3,4]. Zones of metastasis observed by oncologists involve pelvic and par aortic lymph nodes, adnexa and peritoneal surfaces. Gynecologists use the International Federation of Gynecology and Obstetrics staging system for management endometrial carcinoma cases. Stage IA disease are managed by surgery only [5,6]. Internationally approved and recognized guidelines in oncological surgical practice recommend performance of total hysterectomy, bilateral salpingo-oophorectomy and the surgical staging as primary management pathway for cases having endometrial cancer that is restricted to the uterus besides performance of pelvic or paraaortic lymphadenectomy aiming for definite surgical staging and for deciding the requirement of adjuvant therapy [7,8]. Post operative management pathways, e.g. radiotherapy or chemotherapy, are accustomed according to histological cell type, nuclear, cytologic grading, myometrial and cervical tissues depth of pathological invasion, invasiveness of lymph vascular space, peritoneal cytology and disease staging. Surgical staging in cancer endometrium used to be performed historically via open laparotomy as complete cytoreduction of all metastatic sites could improve clinical outcomes with adjuvant therapy [9,10].
Laparoscopic surgical performance for cancer endometrium have been first mentioned in the 1990s consequently robotic surgical interventions began to spread in gyne-oncosurgical practice in the 2000s. Globally implementation and usage of minimally invasive surgical interventions and management for endometrial cancer have been raised from about 9.3% to around 61.7% according to recent statistical analysis. Early endometrial cancer has shown to be feasibly managed by laparoscopic approaches in comparison to conventional laparotomy. The laparoscopic surgery is correlated to lower rates of blood loss and fewer postoperative complications, without influencing the oncologic clinical and survival outcomes of cases affected by this disease [11,12].
Aim of the Work
To compare laparoscopy versus laparotomy for complete uterine cancer surgical staging.
Methodology
Cases having clinical stage I to IIA endometrial carcinoma has been randomly allocated to laparoscopy or open laparotomy involving hysterectomy, salpingo oophorectomy, pelvic cytology, pelvic and para-aortic lymphadenectomy. There were 100 cases randomly selected 35 cases were assigned for laparotomy from that 1 case refused surgery leaving 34 cases for analysis and 65 cases assigned for laparoscopy from those 2 cases refused surgery leaving 63 cases for analysis. As regards the laparotomy arm 1 case underwent and completed elective laparoscopy and 1 case underwent elective laparoscopy but required conversion to laparotomy further more 4 cases deemed ineligible following centralized pathology review 1 case ineligible history, primary site of disease, Inadequate material submitted for central review As regards laparoscopy arm 46 cases Completed laparoscopy, 17cases required conversion to laparotomy 9 cases deemed ineligible following centralized pathology review from them 1 case had Ineligible histology, 2 cases Ineligible primary site of disease, 1 case no cancer identified, 3 cases Inadequate material submitted for central review, 1 case Improper pre protocol treatment.
The chief research study outcomes were the 6-week morbidity and mortality issues, hospitalization period, conversion rates from laparoscopy to laparotomy. Inclusive research criteria were clinical stage I to IIA endometrial carcinoma, normal CBC, renal and hepatic function tests. Conversion from laparoscopy to laparotomy was a decision of the senior operating surgeon. Cases requiring conversion were recorded in a prospective manner. Lymph node dissection number and site were documented. Cytology has been obtained on entering the peritoneal cavity. Pelvic lymph nodes were to be removed from the distal one half of the common iliac artery down to the circumflex iliac vein and nodal tissue was to be removed anterior to the obturator nerve and surrounding the iliac arteries and vein. The para-aortic nodes included those overlying the vena cava between the inferior vena cava and aorta and to the left of the aorta. The technique for laparoscopic hysterectomy involved laparoscopic assisted techniques, total laparoscopic approaches.
Reasons for conversion of laparoscopy to laparotomy, operative time, blood loss, transfusions, intraoperative, postoperative complications, usage of antibiotics, readmissions, reoperations. Intraoperative injuries were documented e.g. bowel, veins, arteries, ureter, bladder or other site. Postoperative adverse clinical and surgical events were recorded on a 6-week clinical follow-up.
Statistical Analysis
Data were collected, revised, coded and entered to the Statistical Package for Social Science (IBM SPSS) version 23. The quantitative data were presented as mean, standard deviations and ranges when parametric and median with inter-quartile range (IQR) when non parametric and percentiles was used to assess the distribution of some parameters. Also, qualitative variables were presented as number and percentages. The comparison between groups regarding qualitative data was done by using Chi-square test and Fisher exact test when the expected count in any cell found less than 5.The comparison between two independent groups with quantitative data and parametric distribution was done by using Independent t-test while with non parametric data was done by using Mann-Whitney test. Logistic regression analysis was used to assess predictors of conversion. The confidence interval was set to 95% and the margin of error accepted was set to 5%. So, the p-value was considered significant at the level of < 0.05.
Results
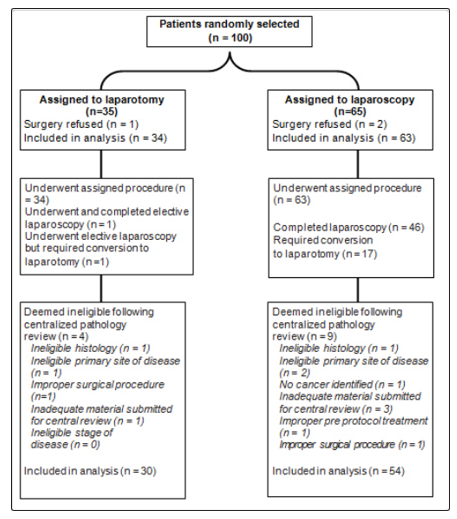
Table 1: Patients characteristic of the studied groups
|
Patients characteristics |
Laparotomy |
Laparoscopy |
Test value |
P-value |
Sig. |
|
No. = 30 |
No. = 54 |
||||
|
Age (years), mean ± SD |
62.8 ± 4.5 |
63.1 ± 3.9 |
0.320* |
0.750 |
NS |
|
Weight (kg), mean ± SD |
75.4 ± 15.3 |
74.1 ± 10.3 |
0.464* |
0.644 |
NS |
|
Height (m), mean ± SD |
1.65 ± 0.21 |
1.64 ± 0.29 |
0.166* |
0.868 |
NS |
|
BMI (kg/m2), mean ± SD |
27.69 ± 3.5 |
27.55 ± 2.96 |
0.194* |
0.846 |
NS |
*: Independent t-test; •: Chi-square test
Table 1 reveals and displays that there was no statistically significant difference between laparotomy and laparoscopy research groups as regards mean ± SD age, weight, height, BMI (p values = 0.750, 0.644, 0.868, 0.846, consecutively
Table 2: Surgical stage, tumor type, types and numbers of nodes of the studied groups
|
|
Laparotomy |
Laparoscopy |
Test value |
P-value |
Sig. |
|
No. = 30 |
No. = 54 |
||||
|
Surgical stage |
|||||
|
IA |
11 (36.7%) |
20 (37.0%) |
1.186• |
0.996 |
NS |
|
IB |
9 (30.0%) |
15 (27.8%) |
|||
|
IC |
3 (10.0%) |
6 (11.1%) |
|||
|
IIA |
1 (3.3%) |
1(1.9%) |
|||
|
IIB |
1 (3.3%) |
2 (3.7%) |
|||
|
IIIA |
1 (3.3%) |
3 (5.6%) |
|||
|
IIIC |
3 (10.0%) |
5 (9.3%) |
|||
|
IVB |
1 (3.3%) |
1 (1.9%) |
|||
|
Unstaged |
0 (0.0%) |
1 (1.9%) |
|||
|
Tumor type |
|||||
|
Endometrioid adenocarcinoma |
24 (80.0%) |
43 (79.6%) |
0.215• |
0.998 |
NS |
|
Ana plastic/other carcinoma |
0 (0.0%) |
0 (0.0%) |
|||
|
Clear cell carcinoma |
1 (3.3%) |
1 (1.9%) |
|||
|
Mixed epithelial carcinoma |
1 (3.3%) |
2 (3.7%) |
|||
|
Serous carcinoma |
3 (10.0%) |
6 (11.1%) |
|||
|
Sarcoma |
1 (3.3%) |
2 (3.7%) |
|||
|
Peritoneal cytology |
29 (96.7%) |
52 (96.3%) |
0.008• |
0.929 |
NS |
|
Type of nodes |
|
|
1.832• |
0.607 |
NS |
|
No nodes |
1 (3.3%) |
2 (3.7%) |
0.008• |
0.928 |
NS |
|
Para-aortic nodes only |
1 (3.3%) |
1 (1.9%) |
0.182• |
0.669 |
NS |
|
Pelvic nodes only |
2 (3.3%) |
2 (3.7%) |
0.373• |
0.541 |
NS |
|
Both pelvic and para-aortic nodes |
26 (86.7%) |
49 (90.7%) |
0.335• |
0.562 |
NS |
|
Any pelvic nodes |
27 (90.0%) |
50 (92.6%) |
0.170• |
0.680 |
NS |
|
No. of nodes, median (IQR) |
16 (11 - 23) |
17 (10 - 26) |
0.107‡ |
0.934 |
NS |
‡: Mann-Whitney test; •: Chi-square test
Table 2 Reveals and displays the Surgical stage, tumor type, types and numbers of nodes of the studied research groups in which there was no statistical significant difference as regards surgical staging, tumor type observed, peritoneal cytology, type of nodes, no nodes, para aortic nodes only, pelvic nodes only, both pelvic and par aortic nodes, any pelvic nodes, No. of nodes, median (IQR) ( p values = 0.996, 0.998, 0.929, 0.607, 0.928, 0.669, 0.541, 0.562, 0.680, 0.934 consecutively)
Table 3: Relation between BMI and conversion rate
|
BMI |
Converted cases |
% from total |
|
< 25 |
1 |
1.9% |
|
25 - 30 |
2 |
3.7% |
|
30 - 35 |
3 |
5.6% |
|
35 - 40 |
4 |
7.4% |
|
> 40 |
7 |
13.0% |
|
Total |
17 |
31.5% |
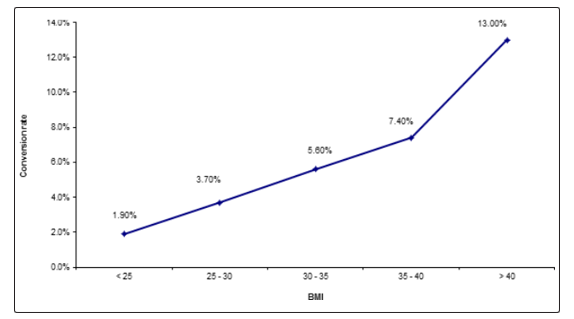
Figure 1 and table 3 reveal and display that as BMI increases the rate of conversion of laparoscopy to laparotomy increases in which cases BMI <25 had 1.9% conversion from total number (1 case only) 2cases having BMI 25-30 had conversion (3.7% from total number of cases) 3 cases having BMI 30-35(5.6% from total number of cases ) 4 cases having BMI 35-40(7.4% from total number of cases) 7cases having BMI above 40 (13% from total number of cases)
Table 4: Complications and adverse events of the studied research groups
|
|
Laparotomy |
Laparoscopy |
Test value |
P-value |
Sig. |
||
|
No. |
% |
No. |
% |
||||
|
Intraoperative complications |
5 |
16.7% |
11 |
20.4% |
0.172• |
0.678 |
NS |
|
Any |
2 |
40.0% |
5 |
45.5% |
|||
|
Bowel |
1 |
20.0% |
1 |
9.1% |
|||
|
Vein |
1 |
20.0% |
1 |
9.1% |
|||
|
Artery |
0 |
0.0% |
1 |
9.1% |
|||
|
Bladder |
0 |
0.0% |
1 |
9.1% |
|||
|
Ureter |
0 |
0.0% |
1 |
9.1% |
|||
|
Other |
1 |
20.0% |
1 |
9.1% |
|||
|
Postoperative adverse events |
16 |
53.3% |
20 |
37.0% |
2.091• |
0.148 |
NS |
|
Any |
6 |
37.5% |
8 |
40.0% |
|||
|
Urinary tract infection |
1 |
6.3% |
1 |
5.0% |
|||
|
Fever |
2 |
12.5% |
2 |
10.0% |
|||
|
Pelvic cellulitis |
0 |
0.0% |
1 |
5.0% |
|||
|
Abscess |
0 |
0.0% |
1 |
5.0% |
|||
|
Venous thrombophlebitis |
1 |
6.3% |
0 |
0.0% |
|||
|
Pulmonary embolus |
1 |
6.3% |
1 |
5.0% |
|||
|
Bowel obstruction |
1 |
6.3% |
0 |
0.0% |
|||
|
Ileus |
2 |
12.5% |
2 |
10.0% |
|||
|
Pneumonia |
0 |
0.0% |
1 |
5.0% |
|||
|
Wound infection |
1 |
6.3% |
2 |
10.0% |
|
|
|
|
Urinary fistula |
0 |
0.0% |
0 |
0.0% |
|||
|
Bowel fistula |
0 |
0.0% |
0 |
0.0% |
|||
|
Congestive heart failure |
0 |
0.0% |
0 |
0.0% |
|||
|
Arrhythmia |
1 |
6.3% |
1 |
5.0% |
|||
|
Perioperative and postoperative period |
24 |
80.0% |
19 |
35.2% |
15.502 |
0.000 |
HS |
|
Blood transfusion |
3 |
10.0% |
5 |
26.3% |
1.337• |
0.247 |
NS |
|
Antibiotics |
14 |
46.7% |
9 |
47.4% |
0.512• |
0.474 |
NS |
|
Readmission |
4 |
13.3% |
3 |
15.8% |
0.006 • |
0.938 |
NS |
|
Reoperation |
2 |
6.7% |
1 |
5.3% |
0.154 • |
0.694 |
NS |
|
Treatment-related deaths |
1 |
3.3% |
1 |
5.3% |
0.029 • |
0.864 |
NS |
|
Hospital stay > 2 days |
29 |
96.7% |
29 |
53.7% |
16.656• |
0.000 |
HS |
•: Chi-square test
Table 4 Reveals and displays the complications and adverse events of the studied research groups (laparotomy and laparoscopy research groups) in which there was no statistical significant difference as regards intraoperative complications, postoperative adverse events blood transfusion requirement, antibiotics administration, readmission rates, reoperation rates, treatment related mortalities (p values= 0.678, 0.148, 0.247, 0.474, 0.988, 0.694, 0.864 consecutively) whereas there was statistical significant difference between laparotomy and laparoscopy research groups as regards, perioperative and post-operative time period, hospital stay more than 2 days ( p values = 0.000 consecutively).
Table 5: Predictors of conversion
|
|
Converted (No. = 17) |
Not converted (No. = 37) |
P-value* |
OR (95% CI), p-value |
|
Increasing BMI than 30 |
7 (41.2%) |
4 (10.8%) |
0.010 |
5.7750 (1.3992 to 23.8361), 0.015 |
|
Metastatic disease |
15 (88.2%) |
20 (54.1%) |
0.014 |
6.3750 (1.2732 to 31.9213), 0.024 |
|
Increasing age than 65 |
15 (88.2%) |
19 (51.4%) |
0.009 |
7.1053 (1.4201 to 35.5509), 0.017 |
*: Chi-square test
Table 5 Reveals and displays the predictors of conversion of laparoscopy to laparotomy procedure in which Increasing BMI, metastatic disease, age above 65 years were the main predictors however were statistically insignificant (p values = 0.010, 0.014, 0.009).
Discussion
Endometrial cancer is one of the common gynecological malignancies that requires careful staging to implement proper management protocols. The minimal invasive laparoscopic approaches is considered one of the best management pathways as it reduces various risk issues correlated to open procedures. One of the corner stone issues that early endometrial cancer is considered feasible by laparoscopic approaches with full accomplishment of surgical resection requirement for management, but obesity prevalent in cancer endometrium cases is considered a surgical and medical challenge for the multidisciplinary management team requiring full coordination and decision making in accordance to the best of the patients benefit [13,14]. Conversion of laparoscopic procedures to open procedure is a common surgical scenario that arises when matters get complicated to handle intraoperatively e.g. due to dense adhesions, obesity and advanced disease. On the other hand, gyne-oncological practice using laparoscopic approaches is a rising field in oncology due to improved laparoscopic tools and safety concerns arising from advances in anesthetic agents implemented [15].
Obesity is one of the common risk factors for the development of endometrial cancer. Additionally, obese women have higher surgical risk in the staging surgery for early endometrial cancer. Various randomized controlled research trials have revealed similar to the current research study that the laparoscopic surgery is correlated to longer operative time, lower intraoperative blood loss in comparison to traditional laparotomy in a statistically significant fashion [1,3]. Prior research studies like the current research study have revealed and displayed that the differences as regards operative time, lymph node numbers removed and hospital stay are statistically significant which furthermore shows great similarity and harmony to the current research study findings [2,5].
A prior retrospective research study to assess the surgical outcomes of the laparoscopic surgery for cases having low-risk endometrial cancer in comparison to laparotomy, the research recruited 120 study subjects having low-risk endometrial cancer, laparoscopic staging surgical procedure involved only the pelvic lymphadenectomy and not the para-aortic lymphadenectomy [4,12].
The laparoscopic surgery had lower intraoperative blood loss and shorter hospital admission time. The operative time has been statistically significantly longer for the laparoscopic surgery in comparison to laparotomy. Researchers from prior research studies have concluded that longer operative time is a drawback for laparoscopic surgery [7,15].
Prior research studies interestingly have revealed and displayed that although difficulties in surgery and challenges are anticipated but laparoscopic approach for endometrial cancer cases has a major privilege over traditional approaches even in obese patients. A Korean research team of investigators have shown that there was no statistically significant difference as regards operative time between the laparoscopic surgery and traditionally known laparotomy approach for obese cases. On the other hand, the disadvantage of longer operative time in the laparoscopic approach has been contradicting observed by various research groups. Interestingly, it was shown by various oncological research teams that the uterine size is a cornerstone factor as regards the feasibility of laparoscopic surgery since large uterus is correlated to space restriction and complexity of transvaginal specimen retrieval [9,11].
A prior research meta-analysis has shown that cases that have undergone laparoscopic surgery have similar intraoperative complications incidence in comparison and contrast to those cases having a classic laparotomy procedure. Those research findings have shown great similarity and harmony to the current research. Another research team of investigators performed a prior research study similar to the current research in approach and methodology have shown that the conversion rate from the laparoscopic surgery to the laparotomy had a statistical range = 0% to 25.8%. Interestingly according to gyne-oncological surgical experience usage of the uterine manipulator for lysis of the adhesion increases the feasibility of the procedure [8,10,14].
Conclusion and Recommendations
The current research elucidates the privilege of laparoscopic surgical staging for early stage endometrial cancer, however future research studies are required to be performed in multicentric fashion and to put in consideration variabilities in BMI, coexisting medical morbidities e.g. DM, hypertension besides the racial and ethnic differences that could affect the anatomical disease presentation. Advances in laparoscopic tools should be investigated in a comparative manner in managing those categories of cases such as advances in 2D and 3D imaging systems of laparoscopic tools.
References
- Obermair A, Janda M, Baker J, Kondalsamy-Chennakesavan S, Brand A, et al (2012) Improved surgical safety after laparoscopic compared to open surgery for apparent early endometrial cancer: Results from a randomized controlled trial. Eur J Cancer 48: 1147-1153.
- National Comprehensive Cancer Network (2016) NCCN clinical practice guidelines in oncology uterine neoplasm’s version 2 professional’s physician gls/f guidelines.asp. http:// www.nccn.org/
- Wright DJ, Burke WM, Tergas AL, Hou JY, Huang Y, et al (2016) Comparative effectiveness of minimally invasive hysterectomy for endometrial cancer. J Clin Oncol 34: 1087-1096.
- Mourits MJ, Bijen CB, Arts HJ, TerBrugge HG, Van der Sijde R, et al (2010) Safety of laparoscopy vs laparotomy in early-stage endometrial cancer: A randomized trial. Lancet Oncol 11: 763-771.
- Janda M, Gebski V, Brand A, Hogg R, Jobling TW, et al (2010) Quality life after total laparoscopic hysterectomy versus total abdominal hysterectomy for stage I endometrial cancer (LACE): A randomized trial. Lancet Oncol 11: 772-780.
- Chu LH, Chang WC, Sheu BC (2016) Comparison of the laparoscopic versus conventional open method for surgical staging of endometrial carcinoma. Taiwanese J Obstet Gynecol 55: 188-192.
- Galaal K, Bryant A, Fisher AD, Al-Khaduri M, Kew F, et a (2012) Laparoscopy versus laparotomy for the management of early stage endometrial cancer. Cochrane Database Syst Rev 12
- Zullo F, Falbo A, Palomba S (2012) Safety of laparoscopy vs laparotomy in the surgical staging of endometrial cancer: A systematic review and meta-analysis of randomized controlled trials. Am J Obstet Gynecol 207: 94-100.
- Gunderson CC, Java J, Moore KN, Walker JL (2014) The impact of obesity on surgical staging, complications and survival with uterine cancer: A Gynecologic Oncology Group LAP2 ancillary data study. Gynecol Oncol 133: 23-27.
- Uccella S, Bonzini M, Palomba S, Fanfani F, Ceccaroni M, et al (2016) Impact of obesity on surgical treatment for endometrial cancer: A multicenter study comparing laparoscopy vs open surgery, with propensity-matched analysis. J Minim Invasive Gynecol 23: 53-61.
- Yoshida E, Terao Y, Hayashi N, Mogushi K, Arakawa A, et al (2017) Promoter-level transcriptome in primary lesions of endometrial cancer identified biomarkers associated with lymph node metastasis. Sci Rep 7:14160.
- Lee CL, Kusunoki S, Huang KG, Wu KY, Huang CY, et al (2016) Long-term survival outcomes of laparoscopic staging surgery in treating endometrial cancer: 20 years of follow-up. Taiwanese J Obstet Gynecol 55: 545-551.
- Baek MH, Lee SW, Park JY, Kim D, Kim JH, et al (2014) Feasibility and safety of laparoscopic surgery for obese Korean women with endometrial cancer: Long-term results at a single institution results. J Korean Med Sci 29: 1536-1543.
- Barnett JC, Havrilesky LJ, Bondurant AE, Fleming ND, Lee PS, et al (2011) Adverse events associated with laparoscopy vs laparotomy in the treatment of endometrial cancer. Am J Obstet Gynecol 205: 143.1-6.
- Uccella S, Bonzini M, Palomba S, Fanfani F, Malzoni M, et al (2016) Laparoscopic vs, open treatment of endometrial cancer in the elderly and very elderly: An age-stratified multicenter study on 1606 women. Gynecol Oncol 141: 211-217.