



Research Article - (2021) Volume 6, Issue 3
Effects on Cerebral Oxygen Balance in Coronary Artery Bypass Grafting: A Comparison of Conventional and Minimal Extracorporeal Circulation
2Department of Extracorporeal Circulation, The First Affiliated Hospital of Guangzhou Medical Univers, China
3Department of Extracorporeal Circulation, Wuhan Asia Heart Hospital, China
#Equally contribution
Received Date: Nov 09, 2021 / Accepted Date: Nov 15, 2021 / Published Date: Nov 25, 2021
Copyright: ©Hui Liu, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Zihao Liu, Ling Zhang, Yan Liu, Hui Liu (2021) Effects on Cerebral Oxygen Balance in Coronary Artery Bypass Grafting: A Comparison of Conventional and Minimal Extracorporeal Circulation. Cardio Open, 6(3): 166-173.
Abstract
Objective: To investigate the cerebral oxygen balance difference between minimal extracorporeal circulation (MECC) and conventional extracorporeal circulation (CECC) during coronary artery bypass grafting.
Methods: 20 patients undergoing coronary artery bypass grafting with cardiopulmonary bypass (CPB) were divided into two groups, the CECC group (n=10) and the MECC group (n=10). Blood withdrawn from radial artery and right jugular vein were analyzed at the following timepoints: during the anesthesia induction (T1), before CPB (T2), the initiation of CPB (T3), aorta crossclamped (T4), after temperature decreased (T5), during stable hypothermia (T6), initiation of rewarming (T7), aorta unclamped (T8), after weaning of CPB (T9), end of the operation (T10).The artery oxygen content (CaO2 ) and cerebral oxygen extraction ratio (OER) were calculated. The mean artery pressure (MAP), hemoglobin (Hb), nasopharyngeal temperature (NPT), and pump perfusion flow were recorded during the operation.
Results: (1) MAP and Hb of MECC group were significantly higher than those in the CECC group from T3 to T10 (P<0.05); perfusion flow in MECC group during CPB was significantly lower than those in CECC group (P<0.05); NPT in MECC group was significantly higher than those in CECC group (P<0.05). (2) During T3-T4 and T8-T9, jugular venous oxygen saturation in CECC group was significantly lower than those in MECC (P<0.05); OER in CECC group was significantly higher than those in MECC group (P<0.05). (3) The arterial lactic acid and venous lactic acid in these two groups were decreased gradually from T3 to T10. Thearteriovenous difference in lactic acid in CECC group were higher than those in MECC group during T3-T4 and T8-T9 (P<0.05).
Conclusion: Patients undergoing coronary artery bypass grafting with MECC enjoy more stable blood pressure, less intense hemodilution and lighter temperature disturbance than those with CECC, which indicating a better cerebral oxygen balance in CABG.
Keywords
Conventional Extracorporeal Circulation, Minimal Extracorporeal Circulation, Coronary Artery Bypass Grafting, Cere- bral Oxygen Balance
Introduction
Standard coronary artery bypass grafting (CABG) surgery em- ploys an arrest of the heart with cardioplegia, providing a mo- tionless, bloodless surgical field, and optimal conditions for the construction of coronary anastomoses. Due to the intractable ad- verse effects of cardiopulmonary bypass (CPB) like inflammatory response and neurologic dysfunction, pump-oxygenator circuits and cardioplegia techniques plateaued throughout the 1990s [1-5]. The off-pump coronary artery bypass (OPCAB), meaning CABG without the use of cardiopulmonary bypass, was then developed, and chosen by many practitioners because of the improvement in inflammatory response, myocardial injury, renal function, and co- agulation function [6-8]. However, this technique is not only lim- ited by the skills of surgeons and anesthesiologists, but also the patient’s circumstances [9-11].
The mini-CPB or minimal extracorporeal circulation (MECC) was introduced to minimize these flaws. The MECC consists of a membrane oxygenator, a centrifugal pump, an arterial filter, and heparin-coated tubing that reduces the priming volume by 450ml [12]. It helps improve the biocompatibility, mitigate the inflam- matory reactions, reduce postoperative bleeding by protecting the coagulation system, protect myocardium by reducing myocardial damage, reduce neurologic damage, as well as provide a motion- less and bloodless surgical condition. MECC is an easy and safe procedure for coronary artery bypass graft surgery [9]. In selected patients, the advantages of MECC equal those of OPCABG [9,13- 17].
Different bypass technologies lead to individualized intraoperation management. Cerebral oxygen balance during surgery is crucial to patients’ neurological function protection and prognosis. Region- al cerebral oxygen saturation (rSO2) obtained from a near-infra- red reflectance spectroscopy (NIRS) was proved to be correlated significantly with heart rate, mean artery pressure (MAP), central venous pressure, arterial carbon dioxide tension, arterial oxygen pressure, and base excess (BE); and is correlated positively with PaO2, MAP, and BE [18,19]. As the NIRS-based cerebral oxime- ter only detect oxygen saturation in a thin superficial layer, it can neither measure global cerebral oxygenation, nor differentiate be- tween arterial and venous blood [20]. In this work, we investigated the cerebral oxygen balance impact brought by MECC, compared the cerebral oxygen balance by monitoring a variety of indicators in patients who underwent coronary artery bypass grafting with these CPB technologies [21].
Materials and Methods
Study Patients: Patients diagnosed with coronary CECC were be classified into the CECC group (n=10); patients undergoing MECC were classified into the MECC group (n=10). The surgeons, anes- thesiologists, and perfusion doctors were specifically designated. General patients’ information is listed in Table 1.
Table 1: Preoperative Patient Data
|
|
CECC (n=10) |
MECC (n=10) |
|
Sex ratio (M/F) |
4.0 |
2.3 |
|
Age (years) |
59.8 ± 5.3 |
63.2 ± 5.0 |
|
Weight (kg) |
72.6 ± 4.8 |
69.8 ± 4.3 |
|
hypertension (%) |
60 |
50 |
|
Diabetes (%) |
30 |
10 |
|
Unstable angina pectoris (%) |
40 |
50 |
|
left ventricular ejection fraction (%) |
53.8 ± 4. 8 |
54.7 ± 5.5 |
Extracorporeal Circulation Protocol The MECC system (Jostra AG, Harlingen, Germany) consisted of a Rota flow® centrifugal pump (Jostra, Germany), a Quadro® arterial microemboli filter (Jostra, Germany), and a Quadrox® membrane oxygenator (Jostra, Germany), as shown in Figure 1A. All the components were en- tirely Bioline® coated (Jostra, Germany) [22]. The CECC system consisted of a roller pump (SIII, Stokert Shiley, Germany), a mem- brane oxygenator, a venous reflux chamber with a priming volume of 4000 ml (TERUMO, Japan), a blood filter (Kewei, Dongguan, China), and a non-heparin coated piping kit (Tianjin Plastics Research Institute, China), as shown in Figure 1B. Details of these systems are listed in Table 2 [23].
Table 2: Comparison of CECC and MECC system
|
|
CECC system |
MECC system |
|
Contact area (m2) |
12 |
3 |
|
Blood storage chamber |
Yes |
No |
|
Priming volume (mL) |
1500 |
500 |
|
Heparin coating |
Yes |
Yes |
|
Heparin (IU/kg) |
400 |
150 |
|
ACT requirement (s) |
>480 |
200-250 |
|
Water tank temperature required during rewarming (°C) |
40 |
38 |
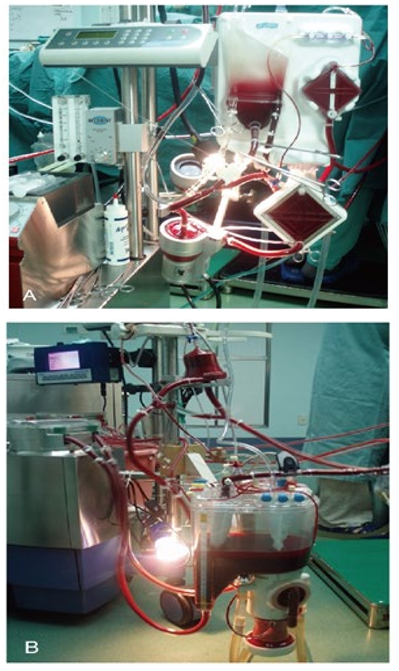
Figure 1: The minimal extracorporeal circulation system (A) and conventional extracorporeal circulation system (B).
Jugular Bulb Catheterization
The jugular bulb is a dilatation in the rostral internal jugular vein right below the jugular foramen [24]. In normal patients, bilateral jugular bulb saturations are equal and probably represent drainage from all parts of the brain [25,26]. Continuous monitoring of the jugular venous oxygen saturation (SjvO2), which is sampled from this position, can be used as an indicator of cerebral oxygenation (20-22) for accuracy, the catheterization is performed as previ- ously described [27]. A 5F double-lumen central venous catheter (Yixinda, Shenzhen, China) is carefully placed in the right jugular vein towards the brain. During the operation, patient’s head was kept still, to prevent the catheter displacement. To withdraw blood samples for analysis, 5ml blood should be taken first, followed by a slow withdraw of 2ml blood [27].
Anesthesia Procedure
The anesthesia procedure consists of:
1. Intramuscular injection of morphine 10 mg and penehyclidine hydrochloride 0.1 mg, as preoperative medications
2. Intravenous injection of midazolam 0.05-0.1 mg/kg, etomi- date 0.2 0.3 mg/kg, vecuronium bromide 0.15-0.2 mg/kg, and sufentanil 1.5-2 mcg/kg, for induction and endotracheal intu- bation
3. Propofol 1-4 mg/(kg.h), sufentanil 1 2 mcg/(kg.h) for anesthe- sia maintenance
4. Midazolam and vecuronium bromide were given intermittent- ly. Invasive blood pressure was established in the left radial artery before induction. A three-lumen venous catheter was placed in the right jugular vein, adjacent to the jugular bulb catheterization. Before CPB, the mechanical ventilation pa- rameters were as follows: tidal volume 8-12 ml/kg, respirato- ry rate 8-12 times/min, inhale/exhale ratio
Data Process
Serial blood samples were analyzed during the anesthesia induc- tion (T1), before CPB (T2), the initiation of CPB (T3), aorta cross- clamped (T4), after temperature decreased (T5), during stable hypothermia (T6), initiation of rewarming (T7), aorta unclamped (T8), after weaning of CPB (T9) and end of the operation (T10). The MAP, hemoglobin (Hb), nasopharyngeal temperature (NPT), pump perfusion flow, arterial blood and jugular bulb blood gas analyses were recorded at the same time. The SjvO2, partial pres- sure of jugular venous oxygen (PjvO2), artery oxygen saturation (SaO2), partial pressure of oxygen (PaO2), arterial lactic acid (AL), and venous lactic acid (VL) were used to calculate the rest indica- tors with the formulas in Table 3.
Table 3: Calculated Parameters and Formulas
|
Description |
Formula |
|
Artery oxygen content(ml/dl) |
CaO2 = (Hb×1.39×SaO2+0.003×PaO2) |
|
Cerebral oxygen extraction ratio (%) |
OER = (CaO2 - CjvO2)/CaO2 |
|
Jugular venous oxygen content (ml/dl) |
CjvO2 = (Hb×1.39×SjvO2+0.003×PjvO2) |
|
Arteriojugular lactic acid difference (mmol/L) |
ADVL = VL-AL |
|
Hb: Hemoglobin; SaO2: artery oxygen saturation; PaO2: partial pressure of oxygen; SjvO2: jugular venous oxygen saturation; PjvO2: partial pressure of jugular venous oxygen; AL: arterial lactic acid; VL: venous lactic acid. |
|
Statistical Processing
Continuous variables are reported as mean ± standard deviation. Categorical variables are reported as frequency and proportion. The statistical analysis has been performed by chi-square test for categorical variables and Student’s t test and Mann Whitney test for continuous variables, utilizing Prism (Version 8, GraphPad Software, Inc). The difference was considered s statistically signif- icant when P value <0.05.
Results
Changes in MAP, Hb, NPT, and Pump Perfusion Flow
MAP: From T3 to T9, the MAP in the MECC group was signifi- cantly higher than that in the CECC group (P <0.05). In the MECC group, MAP from T4 to T8 were significantly lower than that of T2 (P <0.05), but MAP were > 60 mmHg in all cases. In the CECC group, MAP from T3 to T9 were significantly lower than that of T2 (P <0.05). See Figure 2A.
Hb: Hb in both groups decreased after T3 (P <0.05). From T3 to T10, the Hb in MECC group was significantly higher than that in the CECC group (P <0.05). Hb from T3 to T9 in the CECC group were all < 8 g/dL. Hb in the MECC group from T1 to T10 were all > 8 g/dL. See Figure 2B.
NPT: From T5 to T7 the values in MECC group were significantly higher than those in the CECC group P <0.05. The temperature of stable hypothermia ranged from 30 to 32 °C in CECC, and 34 to 35 °C in MECC. See Figure 2C.
Pump Perfusion Flow: The perfusion flow of the CECC group ranged from 2.4 to 2.8 L/(min.m2), and 2.0 to 2.4 L/(min.m2) in the MECC group. From T3 to T8, the perfusion flow in MECC group were significantly lower than those in the CECC group P <0.05 See Figure 2D.

Figure 2: Records of MAP (A), Hb (B), NTP (C) and perfusion flow (D) during the surgery in CECC and MECC groups. Serial values were recorded at consecutive timepoints: the anesthesia induction (T1), before CPB (T2), the initiation of CPB (T3), aorta cross-clamped (T4), after temperature decrease (T5), during stable hypothermia (T6), initiation of rewarming (T7), aorta unclamped (T8), after weaning of CPB (T9) and end of the operation (T10). *P<0.05 indicates a statistically significant difference when compared to the value of T2 in the same group, and #P<0.05 indicates a statistically significant difference comparing the values at the same time between groups. MAP, mean artery pressure; Hb, hemoglobin; NPT, nasopharyngeal temperature; CPB, cardiopulmonary bypass; CECC, conventional extracorporeal circulation; MECC, minimal extracorporeal circulation
Changes of Cerebral Oxygen Metabolism
SjvO2: In the CECC group, SjvO2 in T3, T4, and T7 to T9 were significantly lower than that in T2 (P <0.05). SjvO2 in the CECC group, from T3 to T10 (except for the stable hypothermia phase, T6), were significantly lower than those in the MECC group P <0.05. The peak of both groups at T6 were (CECC: 73.7 ± 9.9%; MECC: 73.5 ± 8.7%). In the CECC group, SjvO2 reached its nadir at T4 and T8. SjvO2 in the MECC group from T1 to T10 were all > 50%. See Figure 3A.
CaO2: In both the MECC and CECC groups, CaO2 decreased sig- nificantly from T3 to T10, compared to T2 (P <0.05). A noticeable decreasing trend can be found in the MECC and CECC group. CaO2 in the MECC group from T3-T10 were significantly higher than those in the CECC group P <0.05. See Figure 3B.
OER: In the CECC group, the OER from T3 to T4 increased and reached the first peak at T4 (42.4 ± 4.1%), which were both sig- nificantly higher than T2 P <0.05; while the OER from T5 to T6 decreased and reached the nadir at T6 (24.7. ± 2.7%), which were both significantly lower than T2 P <0.05. At T7 the value reached its second peak (43.9 ± 4.1%). As for the MECC group, values from T5 to T10 were significantly lower than that of T2 (P <0.05), and reached the nadir at T6 (25.5 ± 2.9%). OER in the MECC group at T4, 5, 7-10 were significantly lower than those in the CECC group (P <0.05). See Figure 3C.

Figure 3: Records of SjvO2 (A), CaO2 (B), and OER (C) during the surgery in CECC and MECC groups. Serial values were recorded at consecutive timepoints: the anesthesia induction (T1), before CPB (T2), the initiation of CPB (T3), aorta cross-clamped (T4), after temperature decrease (T5), during stable hypothermia (T6), initiation of rewarming (T7), aorta unclamped (T8), after weaning of CPB (T9) and end of the operation (T10). *P<0.05 indicates a statistically significant difference when compared to the value of T2 in the same group, and #P<0.05 indicates a statistically significant difference comparing the values at the same time between groups. SjvO2, jugular venous oxygen saturation; CaO2, artery oxygen content; OER, cerebral oxygen extraction ratio; CPB, cardiopulmonary bypass; CECC, conventional extracorporeal circulation; MECC, minimal extracorporeal circulation.
Changes of Lactic Acid Metabolism
AL and VL: In both the MECC and CECC groups, AL and VL from T3 to T10 were increased gradually and were significantly higher than T2 (P <0.05). Comparing the two groups, T7-T10 in AL and T3-T10(except T6) in VL were higher in the CECC group (P <0.05). See Figure 4A, 4B.
ADVL: ADVL from T3 to T5 and T7 to T10 in CECC group were significantly higher than those in MECC group P <0.05. There was no significant difference between the two groups at T6. The trend was consistent with the OER, and opposite to the SjvO2. The line chart is shown in Figure 4C.

Figure 4: Records of arterial lactic acid (A), venous lactic acid (B), and ADVL (C) during the surgery in CECC and MECC groups. Serial values were recorded at consecutive timepoints: the anesthesia induction (T1), before CPB (T2), the initiation of CPB (T3), aorta cross-clamped (T4), after temperature decrease (T5), during stable hypothermia (T6), initiation of rewarming (T7), aorta unclamped (T8), after weaning of CPB (T9) and end of the operation (T10). *P<0.05 indicates a statistically significant difference when compared to the value of T2 in the same group, and #P<0.05 indicates a statistically significant difference comparing the values at the same time between groups. ADVL, arteriojugularlactic aciddifference; CPB, cardiopulmonary bypass; CECC, conventional extracorporeal circu- lation; MECC, minimal extracorporeal circulation.
Conclusion
In this work, 20 cases of CABG surgery under CECC and MECC were retrospectively analyzed by comparing a series of cerebral oxygen related indicators. As MECC is little performed in Chi- na, the data collected in this work is limited but precious. To our knowledge, this is the first exploration focused on cerebral oxy- gen balance with different extracorporeal circulation techniques. Since NIRS-baseed cerebral oximeter detects rSO2 with several flaws, we believed indirectly observing cerebral oxygen through hemodynamics and blood gas tests might be more easy-operating and overall reflected, as evidence showed strong correlation with indicators like rSO2 and MAP, PaO2 and BE [18-21].
Similar to the previous studies, improvements from MECC also showed benefits in our observation [13-15]. As the circulation cir- cuit is much shortened, blood dilution is remarkably reduced. A more stably maintained vascular tension and milder MAP fluctu- ation were observed, which was likely triggered by the mitigated drop-off in catecholamine concentration. The MAP in the MECC group was >60 mmHg at moments. It is reported that patients with a MAP maintaining at 70-90 mmHg during CABG surgery had better prognosis than those at 50-70 mmHg [28]. MAP maintain- ing at 60-90 mmHg could avoid hypoperfusion cerebral ischemia and ensure cerebral oxygen supply [20,29]. The reduced blood dilution with MECC led to a higher hematocrit during the entire CPB period, ensuring sufficient oxygen supply to the brain and other vital organs. In addition, heparin-coated circuit reduces the tube-wall absorption of propofol, which helps ensure the depth of anesthesia, thus reducing cerebral oxygen consumption caused by insufficient anesthesia depth [30].
At the initiation of CPB (T3), SjvO2 only fluctuated mildly, even though MAP has dropped by 45 mmHg, indicating that cerebral oxygen supply and demand were roughly matched [31]. Never- theless, during the CPB (T3-T4) and aorta unclamped (T8) stag- es, SjvO2 in the MECC group was higher than that in the CECC group, while OER and ADVL were markedly lower than those in the MECC group. These findings suggest the CECC group is risky of imbalance between cerebral oxygen supply and consumption in these two stages.
The contributing factors might include:
1. Greater decline in MAP and Hb caused by enhanced blood dilution levels in CECC, leading to insufficient cerebral ox- ygen supply.
2. Rapid rewarming, as in the CECC, was more likely to cause Hb desaturation and affect brain metabolism than slow re- warming [31-33].
3. Brain tissues near the large blood vesselsare preferentially rewarmed, causing excessive craniocerebral rewarming and increase of cerebral oxygen consumption [34]. When the NPT reached 37°C, the brain tissue near the large blood vessels might reached 39-40°C already.
4. The oxygen debt to be repaid during rewarming is more, due to a much lower temperature required in the CECC group during CPB stage, while a higher water tank temperature2°C (38°C for MECC and 40°C for CECC) for rewarming stage. Taken together, the cerebral oxygen supply is compromised, yet the consumption might be even higher, causing a cerebral oxygen supply-consumption imbalance. Difference in SjvO2 and ADVL between two groups verified the beneficial effects mentioned above brought by MECC. By maintaining the NPT at approximately 34-35°C and rectal temperature at 36°C, MECC ensured better microvascular circulation and perfu- sion, lowered lactic acid production during CPB, a higher MAP, and abundant Hb for oxygen supply.
As is well known, hypothermia slows down the myocardium metabolism and enhance hypoxia tolerance for vital organs. Yet, there are also negative effects brought by low temperature, includ- ing mitochondrial dysfunctionand ion transportation dysfunction [35,36]. CPB under normothermia is reported enjoy a lower inci- dence of perioperative myocardial infarction, using of the intraaor- tic balloon pump, low output syndrome, and show little harm to other organs [37,38]. Similar to previous work, during the stable hypothermia stage (T6), SjvO2 in the CECC and MECC were akin (73.7±9.9% and 73.5±8.7%, respectively), which suggest that ce- rebral oxygen balance of the two groups was basically identical, in spite of a higher temperature in MECC group [31]. Due to higher MAP and Hb concentration and sufficient microvascular perfusion pressure, higher temperature with MECC system is practicable as well. Also, OER of the two groups at this stage showed alike trends.
There were limitations in this study. The transcranial Doppler ul- trasound was not applied to measure cerebral blood flow in our study. Combining our measurement and transcranial Doppler ul- trasound might further verify brain perfusion and oxygenation. However, it was not easy to provide continuous measurements during the surgery. In addition, limited sample size might amplify the systematic error.
Conclusion
In summary, we explored the indicators with two extracorporeal circulation techniques and results showed cerebral oxygen sup- ply and demand might not be as well matched in patients with the CECC as it did with the MECC. MECC has a smaller priming volume, lighter blood dilution effect and temperature interference, more stable blood pressure, and more ensured cerebral oxygen supply, thus indicates providing a better cerebral oxygen balance for patients underwent CABG.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The Institutional Review Board of the First Affiliated Hospital of Guangzhou Medical University approved the study protocol. The study outcomes will not affect the future patient management. This study is based on data retrieved from a hospital medical record system. All personal data have been protected and secured according to current national and international laws.
References
- Hirleman E, Larson DF (2008) Cardiopulmonary bypass and edema: physiology and pathophysiology. Perfusion 23: 311- 322.
- Apostolakis E, Filos KS, Koletsis E, Dougenis D (2010) Lung dysfunction following cardiopulmonary bypass. Journal of cardiac surgery 25: 47-55.
- Paparella D, Yau TM, Young E (2002) Cardiopulmonary by- pass induced inflammation: pathophysiology and treatment. An update. European Journal of Cardio-Thoracic Surgery 2: 232-244.
- Goldsborough MA, Selnes OA, McKhann GM (1997) Ad- verse cerebral outcomes after coronary bypass surgery. The New England journal of medicine 336: 1606.
- Newman MF, Kirchner JL, Phillips-Bute B, Gaver V, Grocott H, et al. (2001) Longitudinal assessment of neurocognitive function after coronary-artery bypass surgery. The New En- gland journal of medicine 344: 395-402.
- Ascione R, Lloyd CT, Gomes WJ, Caputo M, Bryan AJ, et al. (1999) Beating versus arrested heart revascularization: eval- uation of myocardial function in a prospective randomized study. European journal of cardio-thoracic surgery 15: 685- 690.
- Ascione R, Lloyd CT, Underwood MJ, Gomes WJ, Angelini GD (1999) On-pump versus off-pump coronary revascular- ization: evaluation of renal function. The Annals of thoracic surgery 68: 493-498.
- Gerritsen WBM, Van Boven WJP, Driessen AHG, Haas FJLM, Aarts LPHJ (2001) Off-pump versus on-pump coronary artery bypass grafting: oxidative stress and renal function. European journal of cardio-thoracic surgery 20: 923-929.
- LaPar DJ, Mery CM, Kozower BD, Kern JA, Kron IL, et al. (2012) The effect of surgeon volume on mortality for off- pump coronary artery bypass grafting. The Journal of thoracic and cardiovascular surgery 143: 854-863.
- Bonchek LI (2003) Surgeon skill influences OPCAB success. The American heart hospital journal 1: 314.
- Shimosaka MIKA, Inoue M, Takahashi HISATO, Takahashi M, Miyajima KEISUKE, et al. (2016) Ultrafast-track An- esthesia (UFTA) in the Operating Room and the Anesthetic Management for Off-pump Coronary Artery Bypass (OP- CAB). Masui. The Japanese journal of anesthesiology 65: 336-340.
- Remadi JP, Marticho P, Butoi I, Rakotoarivelo Z, Trojette F, et al. (2004) Clinical experience with the mini-extracorporeal circulation system: an evolution or a revolution. The Annals of thoracic surgery 77: 2172-2175.
- Harig F, Feyrer R, Mahmoud FO, BlumU, Von der EmdeJ (1999) Reducing the post-pump syndrome by using hepa- rin-coated circuits, steroids, or aprotinin. The Thoracic and cardiovascular surgeon 47: 111-118.
- Fromes Y, Gaillard D, Ponzio O, Chauffert M, Gerhardt MF, et al. (2002) Reduction of the inflammatory response follow- ing coronary bypass grafting with total minimal extracorpore- al circulation. European Journal of Cardio-Thoracic Surgery 22: 527-533.
- Gerritsen WB, Van Boven WJ, Wesselink RM, Smelt M, Morshuis WJ, et al. (2006) Significant reduction in blood loss in patients undergoing minimal extracorporeal circulation. Transfusion Medicine 16: 329-334.
- Immer FF, Pirovino C, Gygax E, Englberger L (2005) Mini- mal versus conventional cardiopulmonary bypass: assessment of intraoperative myocardial damage in coronary bypass sur- gery. European journal of cardio-thoracic surgery 28: 701- 704.
- Zangrillo A, Garozzo FA, Biondi-Zoccai G, Pappalardo F, Monaco F, et al. (2010) Miniaturized cardiopulmonary bypass improves short-term outcome in cardiac surgery: a meta-anal- ysis of randomized controlled studies. The Journal of thoracic and cardiovascular surgery 139: 1162-1169.
- Schober A, Feiner JR, Bickler PE, Rollins MD (2018) Effects of changes in arterial carbon dioxide and oxygen partial pres- sures on cerebral oximeter performance. Anesthesiology 128: 97-108.
- Schmidt C, Heringlake M, Kellner P, Berggreen AE, Maurer H, et al. (2018) The effects of systemic oxygenation on cere- bral oxygen saturation and its relationship to mixed venous oxygen saturation: a prospective observational study compari- son of the INVOS and ForeSight Elite cerebral oximeters. Ca- nadian Journal of Anesthesia/Journal canadien d’anesthésie 65: 766-775.
- Li G, Yang L, Sun Y, Shen SE (2020) Cerebral oxygen desatu- ration in patients with totally thoracoscopic ablation for atrial fibrillation: A prospective observational study. Medicine 99: e19599.
- Watzman HM, Kurth CD, Montenegro LM, Rome J, Steven- JM, et al. (2000) Arterial and venous contributions to near-in- frared cerebral oximetry. The Journal of the American Society of Anesthesiologists 93: 947-953.
- Van Boven WJ, Gerritsen WB, Waanders FG, Haas FJ, Aarts LP (2004) Mini extracorporeal circuit for coronary artery bypass grafting: initial clinical and biochemical results: a comparison with conventional and off-pump coronary artery bypass grafts concerning global oxidative stress and alveolar function. Perfusion 19: 239-246.
- Puehler T, Haneya A, Philipp A, Wiebe K, Keyser A, et al. (2009) Minimal extracorporeal circulation: an alternative for on-pump and off-pump coronary revascularization. The An- nals of thoracic surgery 87: 766-772.
- Williams PL, Warwick R, Dyson M, Bannister LH (1989) Gray’s Anatomy, Churchill Livingstone. Edinburgh-Lon- don-Melbourne-New York.
- Shenkin HA, Harmel MH, Kety SS (1948) Dynamic anatomy of the cerebral circulation. Archives of Neurology & Psychia- try 60: 240-252.
- Gibbs EL, Lennox WG, Gibbs FA (1945) Bilateral internal jugular blood: Comparison of AV differences, oxygen-dex- trose ratios and respiratory quotients. American Journal of Psychiatry 102: 184-190.
- Matta BF, Lam AM (1997) The rate of blood withdrawal af- fects the accuracy ofjugular venous bulb: oxygen saturation measurements. The Journal of the American Society of Anes- thesiologists 86: 806-808.
- Jolfaei OA, Bagheri K, Motamedi O, Akbari M (2012) The ef- fect of mean arterial pressure during cardiopulmonary bypass on clinical and para clinical parameters during and after cor- onary artery bypass graft surgery: 4AP7-2. European Journal of Anaesthesiology| EJA 29: 69-70.
- Yoshitake A, Goto T, Baba T, Shibata Y (1999) Analysis of factors related to jugular venous oxygen saturation during car- diopulmonary bypass. Journal of cardiothoracic and vascular anesthesia 13: 160-164.
- Bailey JM, Mora CT, Shafer SL, Multicenter Study of Periop- erative Ischemia Research Group. (1996) Pharmacokinetics of propofol in adult patients undergoing coronary revascular- ization. The Journal of the American Society of Anesthesiolo- gists 84: 1288-1297.
- Nakajima T, Kuro M, Hayashi Y, Kitaguchi K, Uchida O, et al. (1992) Clinical evaluation of cerebral oxygen balance during cardiopulmonary bypass: on-line continuous monitor- ing of jugular venous oxyhemoglobin saturation. Anesthesia and analgesia 74: 630-635.
- Cook DJ, Orszulak TA, Daly RC, Buda DA (1996) Cerebral hyperthermia during cardiopulmonary bypass in adults. The Journal of thoracic and cardiovascular surgery 111: 268-269.
- Croughwell ND, Newman MF, Blumenthal JA, White WD, Lewis JB, et al. (1994) Jugular bulb saturation and cognitive dysfunction after cardiopulmonary bypass. The Annals of tho- racic surgery 58: 1702-1708.
- Sapire KJ, Gopinath SP, Farhat G, Thakar DR, Gabrielli A, et al. (1997) Cerebral oxygenation during warming after cardio- pulmonary bypass. Critical care medicine 25: 1655-1662.
- Hiller S, DeKroon R, Xu L, Robinette J, Winnik W, et al. (2014) α-Lipoic acid protects mitochondrial enzymes and attenuates lipopolysaccharide-induced hypothermia in mice. Free Radical Biology and Medicine 71: 362-367.
- Buse S, Blancher M, Viglino D, Pasquier M, Maignan M, et al. (2017). The impact of hypothermia on serum potassium concentration: a systematic review. Resuscitation 118: 35-42.
- Lichtenstein S (1991) Warm heart surgery 339:1305.
- Min Z, Jianying Z, Chongtian W (2005) Observation and comparision on normothermia CPB and hypothermia CPB in CABG surgeries (in Chinese). Journal of Dalian Medical Uni- versity 27: 450-452.