


Research Article - (2026) Volume 11, Issue 1
Effect of Fentanyl versus Ketamine on the Incidence of Emergence Delirium from Sevoflurane Anaesthesia in Pediatric Patients
2Consultant Anesthesiologist at SDH Hospital, India
3Institution - GMERS Medical College, India
Received Date: Feb 15, 2026 / Accepted Date: Mar 19, 2026 / Published Date: Apr 14, 2026
Copyright: ©2026 Saumil H Shah, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Solanki, D. D., Shah, S. H., Prasad, T. (2026). Effect of Fentanyl versus Ketamine on the Incidence of Emergence Delirium from Sevoflurane Anaesthesia in Pediatric Patients. J Anesth Pain Med, 11(1), 01-24.
Abstract
Background: Emergence delirium (ED) is a transient confusional state occurring during recovery from general anesthesia, characterized by agitation, crying, restlessness, and disorientation. It is more commonly seen in pediatric patients, particularly following the use of inhalational anesthetics such as sevoflurane. Although ED is usually self-limiting, it can lead to complications such as self-injury, disruption of surgical sites, increased stress for caregivers, and the need for additional monitoring in the post-anesthesia care unit (PACU). Various pharmacological agents including opioids and dissociative anesthetics have been investigated to reduce the incidence of ED.
Aim: To compare the efficacy of intravenous fentanyl (1 μg/kg) and ketamine (0.5 mg/kg) administered 10 minutes before the end of surgery in preventing emergence delirium in pediatric patients undergoing general anesthesia with sevoflurane.
Materials and Methods: This prospective observational study included 60 pediatric patients aged 5–12 years undergoing elective surgeries under general anesthesia. Patients were randomly divided into two groups of 30 each. Group F received intravenous fentanyl 1 μg/kg, while Group K received intravenous ketamine 0.5 mg/kg, administered 10 minutes before completion of surgery. Standard general anesthesia was induced with propofol and maintained with oxygen, nitrous oxide, and sevoflurane. Emergence delirium was assessed using Aono’s four-point scale at 5, 10, 20, and 30 minutes postoperatively. Postoperative pain was evaluated using the Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS), and recovery was assessed using the Modified Aldrete Score. Statistical analysis was performed using independent sample t-test and chi-square test with a p-value <0.05 considered statistically significant.
Results: Demographic characteristics and intraoperative hemodynamic parameters were comparable between the two groups. The incidence of emergence delirium was significantly higher in the ketamine group compared to the fentanyl group. At 5 minutes postoperatively, ED was observed in 63.33% of patients in the ketamine group compared to 16.66% in the fentanyl group. Pain scores measured using CHEOPS were also higher in the ketamine group. Emergence time and extubation time were slightly prolonged in the ketamine group, although both groups maintained stable hemodynamic parameters and showed minimal adverse effects.
Conclusion: Intravenous fentanyl 1 μg/kg administered 10 minutes before the end of surgery is more effective than ketamine 0.5 mg/kg in reducing the incidence of emergence delirium in pediatric patients undergoing sevoflurane anesthesia. Fentanyl also provides better postoperative analgesia with a comparable safety profile.
Keywords
Emergence Delirium, Sevoflurane Anesthesia, Pediatric Anesthesia, Fentanyl, Ketamine
Abbreviations
%-Percentage
ASA- American Society of Anesthesiology
BP- Blood Pressure
CBC- Complete Blood Count
CHEOPS-Children’s Hospital of Eastern Ontario Pain Scale
CNS- Central Nervous System
EA- Emergence agitation
ECG- Electro Cardio Gram
ED- Emergence delirium
F- Female
Inj.- Injection
IR No- Registration Number
iv- Intra Venous
kg- Kilogram
LFT- Liver Function Test
M- Male
mg- miligram
min- minutes
ml- mililitre mm Hg- mili meter of mercury n-Number of patients N2O-Nitrous oxiode
NS- Not Significant
O2-Oxygen
P- Pulse
PACU-Post anaesthesia care unit
RBS- Random Blood Sugar
RFT- Renal Function Test
RR- Respiratory Rate
SBP- Systolic Blood Pressure
SD- Standard Deviation
SpO2- Oxygen Saturation
Sr. no- Serial Number
Wt- Weight
μg- microgram
Introduction
Emergence delirium (ED) is a transient confusional state that is associated with emergence from general anesthesia. It is defined as “a disturbance in a child`s awareness or attention to his /her environmentwithdisorientationandperceptual alterations including hypersensitivity to stimuli and hyperactive motor behaviour in the immediate post anaesthesia period”. This ‘dissociated state of consciousness’ can occur in adults as well as in children but it is much more common in the paediatric population. Emergence delirium is manifest on recovery of consciousness and usually last for 5-15 min; the child is typically irritable, uncooperative and inconsolable, with crying, moaning, writhing, kicking and exhibiting generally inappropriate behaviour. An Emergence agitation is emergence delirium associated with excessive motor activity but both term used interchangeably. Incidences of ED is more than 30%.
Children with emergence delirium appear wild and incoherent. They are inconsolable and do not appear to recognize familiar people [1]. It is self-limiting, resolves quickly and followed by an uneventful recovery. Even though it is usually self-limited, emergence delirium is still considered as a worrisome side effect because of the risks of falling, self-injury to the child or to the surgical site, the stress caused to both caregivers and families and increase in need for continuous monitoring of patients by recovery room staffs and physical restraint of patient [2].
In children, emergence delirium is most frequently associated with rapid “wake up” from inhalational anesthetic agents. Emergence delirium is most often associated with the less-soluble vapors, sevoflurane and desflurane, to a lesser extent with isoflurane and halothane anesthesia. There is 33% higher incidence of delirium during emergence with sevoflurane anesthesia when compared to halothane. Incidence of emergence excitement is more of a reflection of the anesthetic agent used rather than the rapidity of emergence [3].
Several drugs have been investigated to reduce the occurrence and the severity of emergence delirium with variable outcome [4-11]. These include propofol, fentanyl, ramifentanyl ketamine, α 2 agonists like clonidine, dexmeditomidine and they are found to be effective in decreasing the incidence of emergence delirium.
Ketamine is a non-competitive N-methyl-D-aspartate receptor antagonist and is an effective drug for sedation, analgesia and amnesia and the effect of ketamine on decreasing the incidence of EA was confirmed by many studies [4,5,12-14].
Fentanyl, a potent opioid receptor agonist; routinely used in the perioperative period can decrease EA following sevoflurane anesthesia by its high efficacy on perioperative analgesia as well as its sedative effect [6-8].
So this study was planned to compare the efficacy of Fentanyl 1μg/kg iv and Ketamine 0.5 mg/kg iv administered 10 minutes before the end of surgery for the prevention of emergence delirium from sevoflurane anaesthesia in pediatric patients aged 5 -12 years undergoing general anaesthesia for various elective surgeries.
The Aim of The Study
Present study was conducted to compare the efficacy of Fentanyl 1 μg/kg and Ketamine 0.5 mg/kg administered intravenously 10 minutes before the end of surgery for the prevention of emergence delirium in pediatric patients aged 5-12 years undergoing general anaesthesia for various elective surgeries.
Primary objective was to evaluate and compare the incidence of ED based on AONO score between two groups.
Secondary objective ware to compare the following parameters:
• Time to extubation
• Emergence time
• Recovery criteria
• Side effects
Review of Literature
Sevoflurane is a popular inhaled anesthetic widely used for induction and maintenance of anesthesia in pediatric age group. The major with sevoflurane anesthesia is its association with emergence delirium in children. Studies were conducted in the past comparing various agents to reduce the incidence and severity of emergence delirium.
Ashraf Arafat Abdelhalim and Ahmed Mohamed Alarfa
conducted a study on 120 children aged 3-7 years undergoing tonsillectomy surgery under sevoflurane anesthesia [2]. They divided them into three groups, group F receiving 1μg/kg fentanyl, group K receiving 0.5mg/kg ketamine and group C as control. Study drug given 10 minutes before the end of the surgery. They observed that the incidence of emergence delirium was significantly lower in both fentanyl and ketamine groups when compared to the control group with no significant difference between group F and group K. There was also no significant difference regarding recovery and discharge times from post anesthesia care unit. There were no significant differences in Children’s Hospital of Eastern Ontario Pain Scale. The incidence of nausea or vomiting was significantly more in fentanyl group compared to group K and group C.
Kyung Mi Kim, Ki Hwa Lee, Yong Han Kim et al did a study on paediatric patients (2–6 years old) undergoing ophthalmic surgery where they received premedication with either 0.1mg/ kg midazolam or 1mg/kg ketamine and they observed that the incidence of emergence delirium was significantly lower in the ketamine group than the midazolam group [11]. There was no significant difference in overall incidence of emergence delirium. Use of emergence agitation rescue medication fentanyl or midazolam was recorded. The frequency of midazolam used as rescue medication was significantly lower in the ketamine group than in the midazolam group.
Manal M. Rashad, Dalal E.M et al performed a study to compare the effect of intravenous injection of small dose of propofol, fentanyl or ketamine at the end of surgery, just before the discontinuation of sevoflurane on the incidence and severity of sevoflurane emergence agitation in children undergoing hypospadias repair operations [15]. They observed that the incidence of emergence agitation was significantly lower in propofol and fentanyl groups when compared to ketamine and control group. The time for awakening was significantly prolonged in propofol, ketamine and fentanyl groups, while PACU duration was significantly prolonged in fentanyl group. No significant complications occurred except a significantly higher incidence of vomiting in fentanyl group.
M.-S. Kim B.-E. Moon H. Kim J.-R. Lee designed a study to compare the effect of fentanyl and propofol on pediatric patients receiving sevoflurane anesthesia on the incidence of emergence delirium and they observed that the incidence of emergence delirium is lower in both propofol and fentanyl groups when compared to control group with no significant difference between the fentanyl and propofol groups [16]. The incidence of nausea and vomiting is more in fentanyl group. Fentanyl and propofol group have longer duration of stay in PACU when compared to control group with no difference between the fentanyl and propofol groups.
Dahmani S, Stany i, Brasher C, Lejeune C, Bruneau B et al observed in a meta-analysis that propofol, ketamine, fentanyl and preoperative or perioperative analgesia had a prophylactic effect in preventing emergence delirium [17]. The analgesic properties of these drugs do not seem to have a role in this effect.
Lee YS, Kim WY, Choi JH, Son JH et al observed the effect of two different doses of Ketamine on the incidence of emergence agitation in children undergoing tonsillectomy and adenoidectomy under sevoflurane general anesthesia and concluded that the incidence of emergence delirium and CHEOPS is low in ketamine group when compared to control group with no difference between the groups receiving 0.5 mg/kg of ketamine at the end of surgery and 1mg/kg of ketamine at the beginning of surgery [13]. Extubation time in ketamine group receiving 0.5 mg/kg at the end of surgery was significantly prolonged compared with ketamine group receiving 1mg/kg at the beginning of surgery and the control group.
Yoon Sook Lee, Woon Young Kim, Jae Ho Choi, Joo Hyung et al studied for effectiveness of ketamine on the incidence of emergence agitation in 93 children, ASA I-II, 2-14 years old, undergoing adenotonsillectomy [18]. The patients were allocated randomly to one of the three groups receiving saline (group C), ketamine 0.25 mg/kg (group K 0.25) or ketamine 0.5 mg/kg (group K 0.5). The children in each group were administered the study drugs 10 minutes before the end of surgery. They evaluated there were no significant differences in the extubation time, delivery time and postoperative nausea and vomiting between the three groups. There were significant differences in modified CHEOPS (Children’s Hospital of Eastern Ontario Pain Scale) between the three groups. They concluded that the incidence of emergence agitation was low in the K 0.25 and K 0.5 groups compared to the control group. However, there was no significant difference between the K 0.25 and K 0.5 groups.
Abu-Shahwan I, Chowdary K conducted a study for effectiveness of Ketamine in decreasing the incidence of emergence agitation in 85 premedicated children of 4-7 years undergoing dental repair under sevoflurane general anesthesia [14]. Children were premedicated with acetaminophen and midazolam. Anesthesia was induced and maintained with sevoflurane in N2O/O2. Group K received ketamine 0.25 mg/kg and Group S received saline. They evaluated recovery characteristics upon awakening and during the first 30 minutes using the Pediatric Anesthesia Emergence Delirium scale. They concluded that the addition of ketamine 0.25 mg/kg can decrease the incidence of emergence agitation in children after sevoflurane general anesthesia.
Dalens BJ, Pinard aM, Létourneau et al conducted a study for pediatric cerebral magnetic resonance imaging with small doses of ketamine or nalbuphine administered just before discontinuing sevoflurane anesthesia for prevention of emergence delirium [12]. They observed that the incidence of emergence delirium is lower in Ketamine and Nalbuphine group when compared to the control group.
Incidence of emergence delirium in Nalbuphine group is lower than that of Ketamine group.
Alper Kararmaz Paediatr Anaesth conducted a study to determine whether oral ketamine premedication affected the incidence of emergence agitation in children [19]. Thirty minutes before induction of anaesthesia, 80 children who were undergoing adenotonsillectomy with or without bilateral myringotomy and insertion of tubes received either ketamine 6 mg/kg per oral in group K or sour cherry juice alone in group C. Anaesthesia was maintained with desflurane. Emergence and recovery times were recorded. Tramadol was used for postoperative analgesia. Fentanyl (1 µg/kg was administered for the treatment of emergence agitation or severe pain that still continued after tramadol administration. Postoperative behaviour was evaluated using a 5-point agitation scale. They evaluated that the incidence of emergence agitation was 56% in group C and 18% in group K (P=0.001). They concluded that oral ketamine in premedication reduced the incidence of post anaesthesia emergence agitation in children without delaying recovery.
Joseph P Cravero designed a prospective, randomized, and controlled trial study to measure the effect of a small dose of iv fentanyl on the emergence characteristics of pediatric patients undergoing sevoflurane anesthesia without any surgical intervention. 32 ASA physical status I or II pediatric outpatients receiving sevoflurane anesthesia for magnetic resonance imaging scans were enrolled and assigned in a random and double-blinded manner to receive either placebo (saline) or 1 µg/kg iv fentanyl 10 minutes before discontinuation of their anesthetic agents [20]. The primary outcome measured was the percentage of patients with emergence agitation, the duration of agitation and the time to meet hospital discharge criteria. Patients who received fentanyl had a decreased incidence of agitation (12% versus 56%) when compared with placebo. There was no significant difference in time to meet hospital discharge criteria. Study concluded that the addition of a small dose of fentanyl to inhaled sevoflurane anesthesia decreases the incidence of emergence agitation independent of pain control effects.
Ira Todd Cohen conducted a study to examine the effect of a single intraoperative dose of fentanyl on emergence characteristics in children undergoing adenoidectomy. One hundred children, 2-7year old, were randomly assigned to receive desflurane or sevoflurane for maintenance of general anesthesia after an inhaled induction with sevoflurane and a 2.5 µg/kg dose of fentanyl [21].
An observer blinded to the anesthetic technique assessed the times to achieve emergence, extubation and recovery criteria, as well as emergence behaviors. The results showed a similar incidence of severe emergence agitation after general anesthesia with desflurane (24%) and sevoflurane (18%). Time to achieve extubation and post anesthesia care unit discharge criteria were shorter with desflurane than with sevoflurane. With this technique, desflurane allows for a more rapid emergence and recovery than sevoflurane. In children receiving desflurane or sevoflurane, the concurrent use of fentanyl in a dose of 2.5 µg/kg results in a small incidence of emergence agitation. The concurrent use of fentanyl in a dose of 2.5 µg/kg in children receiving desflurane or sevoflurane results in a low incidence of emergence agitation. Desflurane allows for a more rapid emergence and recovery than sevoflurane.
Pathophysiology of Emergence Delirium
Definition
Sikich and Lerman defined emergence delirium as “a disturbance in a child’s awareness of and attention to his/her environment with disorientation and perceptual alterations including hypersensitivity to stimuli and hyperactive motor behavior in the immediate post anesthesia period.” It occurs within the first 30 min of recovery from anesthesia, is self-limited (5–15min), and often resolves spontaneously [22].
Incidence
The incidence of emergence delirium in all postoperative patients is 5.3%. Incidence in children is (12-13%).
The incidence of emergence delirium after halothane, isoflurane, sevoflurane and desflurane ranges from 2-55% but may be as high as 80%.
Mearsurement Scale
Cravero scale
Pediatric anesthesia emergence delirium scale (PAED)
Watcha scale
AONO’s four-point scale
Emergence Agitation
Sedation-Agitation Scale (SAS)
Richmond Agitation Sedation Scale (RASS) [5,23-26]
Pathophysiology
The first sense to return during emergence from anesthesia is hearing, a sense that is made possible by the synapse between the acoustic thalamus and the lateral nucleus of the amygdala (LA) [27]. During post-anesthesia recovery, this connection is also responsible for auditory fear conditioning by exaggerating an inappropriate response to auditory stimuli.
Down regulation of large-conductance Ca2+activated potassium channels decrease in Ca2+ channels is associated with an increase in excitatory activity evoked by NMDA postsynaptic potentials at the thalamo-LA synapse, therefore enhancing stress induced behavior.
Postoperative emergence mimics Guedel Stage II (excitement stage) of anesthesiapronounced slowing pattern on the electroencephalogram due to the interference of neurotransmitter metabolism and function within the central nervous system.
Specific excitation of the Locus Ceruleus neurons by inhalational anesthetics, especially sevoflurane, which ultimately plays an important role in this paradoxical excitation potentiation by sevoflurane of GABAergic depolarization/excitation in neocortical neuron [28].
Etiological Factors
Pre-operative Risk Factors
Genetics
Genetic polymorphism in the regions of IL-1, IL-6, IL-10, TNFα play an important role in the immune response and inflammatory pathway that may predispose the patient to post operative delirium [29]. Currently there are insufficient studies to explain the basis behind the genetic predisposition of emergence delirium.
Age
Patients with age less than 40 years and age more than 64 years are more prone for emergence delirium [30]. Similarly, pediatric patients with less than 5 years of age reported to have higher incidence of emergence delirium [3].
There are decreased levels of acetyl choline, dopamine, norepinephrine and GABA present in both geriatric and pediatric population. Any disturbances to these neurotransmitters are implicated in development of emergence delirium [31].
Benzodiazepines
Studies have reported that preoperative use of benzodiazepines increase the risk of emergence delirium [31]. Other drugs that are associated with emergence delirium are
• Atropine
• Scopolamine
• Ketamine
• Barbiturates [32].
Perioperative Risk Factors
Inhalational Anesthetics
Several studies have shown that there is direct correlation between the use of inhalational anesthetics and the occurrence of emergence delirium [5]. Among the inhalational anesthetics emergence delirium appear more commonly with the use of sevoflurane than with desflurane and halothane [24]. This may be attributed to the low blood solubility which is a characteristic feature of newer inhalational anesthetics that cause rapid awakening thereby increasing the susceptibility of occurrence of emergence delirium [17].
Surgery
The occurrence of emergence delirium is associated with the type of surgery that the patient undergoes [31]. Patients who underwent breast and abdominal surgeries have higher incidence of emergence delirium [31]. Surgeries involving tonsils, middle ear and eye are also shown to have increased incidence of emergence Delirium [5].
Pain
The level of pain is an independent contributing factor for the occurrence emergence delirium [31]. Several studies have shown that alleviation of pain has decreased the incidence of emergence delirium [17,30]. Preoperative anxiety and underlying temperament of the patient undergoing surgery are also risk factors for occurrence of emergence delirium [3].
Temperament
Children who are more emotional, more impulsive, less social, and less adaptable to environmental changes were found to be at risk for development of emergence agitation. It may be due to the fact that there is some substrate innate to each child that may elicit a fearful response to outside stimuli, depending on the interaction between the child and the environment [32]. This reaction, which describes the “excitability, responsivity, or arousability” of the child, might be the underlying substrate from which both preoperative anxiety and emergence delirium arise [33].
Prevention and Treatment of Emergence Delirium
Simple preventive measures should be taken to treat children at risk. These include
• reducing preoperative anxiety,
• treating postoperative pain, and
• providing a stress-free environment for recovery. Several medications had been investigated to prevent and treat emergence agitation and delirium.
Benzodiazepines
Despite the increased risk of emergence delirium with preoperative use of benzodiazepines, studies have shown that there is decreased incidence of emergence delirium when the benzodiazepines is administered perioperatively [11].
NSAIDs and Opiods
Pain is an independent risk factor for emergence delirium especially in pediatric population. So adequate pain relief decreases the incidence of emergence delirium. Several studies have shown that NSAIDs like ketorolac and opiods like fentanyl and remifentanil decreases the incidence of emergence delirium [5,8,9].
α 2 Agonists
Among the α 2 agonists two drugs, clonidine and dexmeditomidine are shown to be effective in the management of emergence delirium.
Clonidine
Clonidine exhibit decrease in incidence of emergence delirium with an added advantage of good sedation during induction and better postoperative analgesia [17].
Dexmeditomidine
Dexmeditomidine has relatively benign safety profile and improved efficacy, hence it is preferred for prevention and management of emergence delirium. It also has an advantage of improved symptomatic coverage by decreasing the incidence of PONV, post operative pain, chill and restlessness associated with general Anesthesia [34].
Ketamine
Earlier studies have shown that ketamine itself is a risk factor for emergence delirium. However recent studies have shown that ketamine when given orally or intravenously in low doses is effective in preventing the occurrence of emergence delirium [11-13]. When emergence delirium does occur, non-pharmacological treatment involves ensuring patient safety, excluding physical discomfort and reassuring the patient, parents and healthcare workers regarding its transient nature. Pharmacological ‘rescue’ treatments that have been reported to be effective include intravenous boluses of sedative agents such as midazolam 0.025 mg/kg or propofol 0.5–1 mg/kg and opioids such as intravenous fentanyl 1–2 μg/kg [35-37].
Pharmacology of Fentanyl
Fentanyl is a phenyl piperidine-derivative synthetic opioid agonist that is structurally related to meperidine [38]. As an analgesic, fentanyl is 75 to 125 times more potent than morphine.
Chemical structure- tertiary amine which is a synthetic phenylpiperidine derivative
Physical Properties Available as
• Clear colourless solution for injection
• Transdermal patch
• Sublingual tablets
• Lozenges
• Iontophoretic transdermal system pKa of fentanyl is 8.4, 9% unionized at a pH of 7.4 Molecular weight- 286 Highly lipid soluble.
Mechanism of Action
Fentanyl is highly selective mu agonist, mu receptor appears to be specifically involved in the mediation of analgesia. Opiods appear to exert their effects by interacting with presynaptic Gi protein receptor leading to hyper-polarisation of cell membrane by increasing K+ conductance. Inhibition of adenylate cyclase, leading to reduced production of cAMP and closure of voltage sensitive calcium channels occurs.The decrease in membrane excitability that results may decrease both pre and post synaptic responses.
Route of Administration/ Doses
Premedication - intramuscular route -50 to 100 µgm Anesthetic induction is usually achieved by combining a loading dose of fentanyl (2 to 6 µg/kg) with a sedative-hypnotic, most commonly thiopental or propofol, and a muscle relaxant.
Maintenance of anesthesia can be achieved with N2O (60% to 70%)in O2, low concentrations of potent inhaled anesthetic agents, and additional fentanyl (intermittent boluses of 25 to 50 µg every 15 to 30 minutes or a constant infusion of 0.5 to 5.0 µg/kg/hour).
Epidural route – 50 to 100 µgm
As an adjuvant in spinal anesthesia- 5-25 µgm The drug acts rapidly in 2-5 minutes due to its rapid lipid solubility when administered intravenously. Small doses have duration of action of 30-60 minutes whereas high doses may be effective for 4-6 hrs.
Transdermal fentanyl patch-serum fentanyl concentration increases gradually with equilibrium occurring between 12-24 hrs. It should be replaced every 72 hrs.
Iontophoretic transdermal system devices should be replaced or stopped after 24 hrs.
Effects
Cardiovascular System
The most significant effect is bradycardia of vagal origin. Cardiac output, mean arterial pressure, systemic and pulmonary vascular resistance remain unaffected. It obtunds the cardiovascular response to laryngoscopy and intubation.
Respiratory System
It is a potent respiratory depressant causing a decrease in both respiratory rate and tidal volume. It diminishes the ventilator response to hypoxia and hypercarbia. It is a potent antitussive agent. Fentanyl causes chest wall rigidity- wooden chest phenomenon may occur due to its effect on mu receptors located on the GABAergic interneurons. It causes minimal histamine release, so bronchospasm is rare.
Central Nervous System
Fentanyl is 50-80 times more potent an analgesic than morphine and has little sedative and hypnotic property. Miosis is produced due to the stimulation of Edinger Westphal nucleus. Opioids reduce cerebral oxygen consumption, cerebral blood flow, cerebral blood volume, and intracranial pressure. Large doses of Fentanyl may rarely cause seizure like motor activity. No epileptic spike wave patterns are demonstrable in EEG. Stimulation of the medullary chemoreceptor trigger zone is responsible for opioid-induced nausea and vomiting.
Gastro Intestinal
Decreases gastro intestinal motility and decreases gastric acid secretion. Biliary colic may result from opioid-induced contraction of the sphincter of Oddi
Endocrine
Fentanyl obtund the metabolic stress response to surgery by decreasing the secretion of stress hormones like catecholamines and cortisol. It does not increase the activity of ADH.
Toxicity/Side Effects
• Respiratory depression- due to the appearance of secondary peak in the plasma fentanyl concentration due to elution from the muscle
• Nausea and vomiting
• Dependence
Pharmacokinetics Absorption
Fentanyl is absorbed orally and has a bioavailability of 33%. Orally administered fentanyl becomes highly ionized in the stomach (99.9%), leading to slow absorption in the small bowel and subsequent first pass metabolism.
Distribution
Fentanyl is 81-94% bound to plasma proteins Vd is 0.88-4.41 l/kg.
Short duration of action of single dose of drug is due to redistribution, whereas continuous infusion may lead to saturation of tissues and prolonged duration of action.
It is more lipid soluble, crosses the blood brain barrier easily and has faster onset of action.
Intrathecal fentanyl does not cause delayed respiratory depression, as due to its high lipid solubility, it is rapidly absorbed in the spinal cord.
Metabolism
Fentanyl is metabolized primarily by N-deaklylation to norfentanyl with subsequent hydroxylation to hydroxy propionyl derivatives. It also undergoes hydroxylation and amide hydrolysis. Cytochrome P450 3A plays predominant role.
Excretion
10% of administered dose is excreted in urine.
Clearance -13ml/kg/min.
Elimination half-life -141-853 minutes.
Halothane decreases the clearance of fentanyl by 48%.
Clearance of fentanyl is decreased in patients with renal and hepatic impairment.
Drug Interaction
Fentanyl decreases the apparent MAC of coadministered volatile agents increases the effect of nondepolarizing muscle relaxant.
Pharmacology of Ketamine
Ketamine is a water-soluble phencyclidine derivative [39]. The Ketamine molecule contains an asymmetric carbon atom with two enantiomers. The S (+) isomer and R (-) isomer.
Chemical Structure
Pharmacokinetics
Ketamine is highly lipid soluble and undergoes rapid breakdown and redistribution to peripheral tissues. It is metabolized extensively in the liver by N-demethylation and ring hydroxylation pathways. Nor Ketamine is main metabolite and is onethird to one-fifth as potent as Ketamine as an anaesthetic.
Ketamine is excreted in urine and faeces as nor Ketamine and as hydroxylated derivatives. It has a cumulative effect. Gradual resistance builds up on repeated administration.
Pharmacodynamics
• Cardiovascular System: Ketamine increase in heart rate, blood pressure and cardiac output, mediated principally through sympathetic nervous system.
• Respiratory System: Ketamine has minimal effect on central respiratory drive and produces relaxation of airway and bronchial smooth muscles.
• Central Nervous System: Ketamine has cataleptic, amnestic, profound analgesic and dose dependent anesthetic actions. The cataleptic state is an akinetic state with the loss of orthostatic reflexes, but without impairment of consciousness. The dissociative state produced by Ketamine is unique in which patient appears awake but is detached from the surroundings with eye remaining open.
• Eye: Ketamine increases intraocular pressure and causes nystagmus.
• Gastrointestinal System: Ketamine increases intragastric pressure, it increases salivary secretions.
Onset of Action
![]() Intravenous route: 30 seconds
Intravenous route: 30 seconds
![]() Intramuscular route: 1 to 5 mins
Intramuscular route: 1 to 5 mins
Mechanism of Action
The main mechanism of action of Ketamine is noncompetitive antagonism or the N-methyl D-aspartic acid (NMDA) receptor. Ketamine also interacts with opioid receptor, monoamine, cholinergic, purinergic and adrenoreceptore system as well as having local anaesthetic effects. Ketamine depresses some parts of thalamus and neocortex while stimulates limbic system. This leads to what is called as dissociative anesthesia.
Doses For induction
![]() Intravenous route: 0.5-2 mg/kg
Intravenous route: 0.5-2 mg/kg
![]() Intramuscular route: 4-6mg/kg
Intramuscular route: 4-6mg/kg
![]() Oral route: 3-10mg/kg
Oral route: 3-10mg/kg
Advantages and Uses:
• Induction agent of choice for
![]() Asthamatic
Asthamatic
![]() Shock
Shock
![]() Children
Children
• Sole agent for minor procedures
• COPD- potent bronchodilator (iv anesthetic drug of choice).
Disadvantage
• Incidence of hallucination and emergence reaction
• Increases muscle tone
• Increases pharyngeal and laryngeal secretions.
• Increases myocardial oxygen demand.
• All pressures like intraocular, intragastric, intracranial are markedly raised.
Contraindications
• Head injury
• Patient with intracranial space occupying lesion
• Eye injury
• Ischemic heart disease
• Vascular aneurysm
• Patient with psychiatric disease and drug addicts
• Hypertensives
• Hyperthyroidism
• Pheochromocytoma
Pharmacology of Sevoflurane History
Chemical Structure
Derivative of methyl isopropyl ether.
Physical Properties
Halogenated volatile inhalational anesthetic agent which contains only fluoride ion.
No chlorine or bromine ion like other halogenated agents, therefore no effect on the ozone layer.
Appearance -Clear, Colorless liquid
Formula- C4H3F7O
Odour - Non pungent
Molecular weight- 200.5
Boiling point at 1 atmospheric pressure- 58.5 ºC
Saturated vapor pressure(SVP) at 20º C-160 mm of hg
Blood-gas solubility -1.60.
MAC of Sevoflurane:
|
Age of patient |
MAC |
|
0-1 month |
3.3% |
|
1- 6 months |
3.0% |
|
6 months-3 years |
2.8% |
|
3-12 years |
2.5% |
|
Adults |
1.7-2.1% |
|
Elder |
1.48% |
Pharmacokinetics
Uptake and distribution:
• Low blood gas partition coefficient.
• Very low solubility in blood resulting in rapid onset of action
• Rapid elimination through lungs resulting in faster recovery.
Metabolism
• Occurs in liver, catalyzed by the cytochrome P4502E1 enzyme.
• Sevoflurane broken down into inorganic fluoride ions and organic fluoride metabolite Hexafluoro isopropanol (HFIP).
• HFIP conjugated with glucuronic acid to from HFIP glucuronide.
• Approximately 5% of the Sevoflurane dose may be metabolized.
Elimination
• Primarily excreted through the lung.
• Up to 3.5% of the Sevoflurane dose appears in the urine as inorganic fluoride.
Pharmacodynamics
Central Nervous System
• Slight increase in CBF and ICP at normocarbia.
• Decrease in CMRO2.
•Dose dependent changes in EEG.
• Emergence reaction: Agitation, Patient movement.
Cardiovascular System
• Minimal effect on heart rate.
•Mildly depress cardiovascular contractility through an effect on calcium channel.
•Reduction in cardiac output and systemic vascular resistance causes fall in systemic blood pressure.
• Reduces pulmonary arterial pressure.
• Dose not sensitizes myocardium to epinephrine.
•Cardioprotective properties - Dose not lead to coronary steal.
Respiratory System
•Nonpungent, non-irritant effect on airway.
• Low blood gas solubility, makes it suitable for inhalational induction especially in children.
• Respiratory depressant - decrease minute ventilation.
• Bronchodilator.
•Abolishes hypoxic pulmonary vasoconstriction.
Neuromuscular Effects
• At deeper levels of anesthesia it provides sufficient relaxation to allow tracheal intubation especially in children. â?ª Potentiates effects of neuromuscular blocking agents.
Renal Effects
• Slightly decrease renal blood flow and concentration ability.
Hepatic
•Decreases portal vein blood flow, but increases hepatic artery blood flow, thereby maintaining total hepatic blood flow and oxygen delivery.
Biotransformation and Toxicity
• No evidence of toxicity reported with inorganic fluoride or organic metabolite HFIP.Production of compound A when exposed to sodalime / beralime. Compound A {fluoromethyl 2, 2-difluoro-1- (trifluoromethyl) vinyl ether} has been reported nephrotoxic in animal studies and there are fears it may also be toxic to humans. Production of compound A is more with fresh gas flow less than 2 liters per minute.
Contraindications
• Known allergy or sensitivity.
• Malignant hyperthermia. Advantages of Sevoflurane Particular to Children
•Non pungent, Non-irritant.
• Rapid and smooth induction.
• Adequate muscle relaxation for tracheal intubation.
• Hemodynamically stable.
Uses of Sevoflurane
• Induction and maintainance of general anesthesia.
• Suitable for insertion of LMA.
Material and Method
This prospective observational study was carried out at our tertiary care centre. A total of 60 pediatric patients aged 5-12 years undergoing various elective surgeries under general anaesthesia were included. Inclusion Criteria (I) patients undergoing elective surgery under general anaesthesia (ll) Age 5 to 12 years (IlI) ASA l &ll (IV) Written informed consent from parents. Exclusion Criteria (I) ASA grade III and IV (II) Cognitive or developmental disorder (III) Patients on sedative medication (IV) Neurological condition that may limit patient’s ability to communicate with or understanding nursing personnel. (V) Patients requiring additional dose of muscle relaxant. 8.1. Pre-anesthetic Evaluation Preoperative evaluation was carried out in all patients who satisfied the above mentioned inclusion criteria on the day prior to surgery. The detailed history, general and systemic examination and routine investigations including all blood investigations like CBC, RBS, S. electrolytes, RFT, LFT and other special investigations like X-ray chest and ECG were done when needed. Patients were kept NBM for 6 hours. Parents were explained about the purpose of the study and about the possible adverse events that can occur due to the study drug, and written informed consent was obtained from those parents who were willing to allow their children to take part in the study. 8.2. Preoperative Preparation Patients were taken in operation theater, routine monitors like electrocardiogram, noninvasive blood pressure cuff and pulse oximeter, capnography were applied to the patients and baseline vitals were noted and iv fluid started. Patients were randomly divided into two groups, each group included 30 patients. Randomization was done with simple odd and even technique. Every odd numbered case was assigned to Group-F(fentanyl) and every even numbered case to Group-K(ketamine). In GROUP F, patients received 1µg/kg of fentanyl 10 minutes before the end of surgery, (n=30). In GROUP K, patients received 0.5mg/kg of ketamine 10 minutes before the end of surgery, (n=30) Technique of anesthesia: GENERAL ANESTHESIA with endotracheal intubation. 8.2.1. Premedication All patients were premedicated with: Inj. Ondansetron hydrochloride 0.15mg/kg iv Inj. Glycopyrrolate 0.004mg/kg iv Preoxygenation done with 100% O2 for 3 minutes. 8.2.2. Induction Inj. Propofol 2mg/kg iv Inj. Atracurium basilate 0.5mg/kg iv After complete relaxation, laryngoscopy and intubation were done with proper sized endotracheal cuffed tubes. Bilateral air entry was checked and the cuff was inflated. Tube was then fixed and patient kept on ventilator. Paracetamol suppository 15mg/kg is kept after induction. 8.2.3. Maintenance Anesthesia was maintained with oxygen+ nitrous oxide (50:50), sevoflurane and Atracurium besylatein incremental dose of 0.1 mg/kg iv as per requirement to maintain surgical relaxation. Ten minutes before the end of surgery, the study drugs were injected iv according to the allocated group. At end of surgery, once hemostasis was achieved, the inhalational anaesthetics were discontinued, manual ventilation was performed with 100% O2 at 6L/min. After onset of spontaneous respiration, the neuro muscular blockade was reversed with Inj. Neostigmine 0.05mg/kg iv and Inj. Glycopyrrolate 0.008mg/kg iv. After thorough oropharyngeal suctioning, after return of sufficient spontaneous breathing, gag reflex, facial grimaces and purposeful motor movements, patient was extubated and put in recovery position. 8.3. Parameters Monitered 8.3.1. Emergence Time Defined as the time of first response to command or eye opening on command after discontinuation of inhalational anesthetics. Time to Extubation Defined as time from the end of surgery to tracheal extubation. Duration of Anesthesia recorded as the time from intubation to extubation. 8.3.2. Incidence of Emergence Delirium All patients were observed continuously in post anaesthesia care unit(PACU) for at least 30 min. The primary outcome of the study is the incidence of post-operative emergence delirium, which is assessed every 5 min during the first 30 min using Aono’s four point scale as follows: (1) Asleep (2) Awake but calm (3) Agitated but consolable (4) agitated and difficult to console Grades 1 and 2 in the scale of behavior are considered as no delirium and Grades 3 and 4 are considered as the presence of delirium. 8.3.2.1. The Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS) Crying, facial expression, verbal statements, position of torso, touching of the wound and movement of legs is used for post-operative pain assessment and it is measured at 5, 10, 20 and 30 min post-operatively. Minimum score - 4 Maximum score – 13 ≥ 6 score require analgesic
|
CRY |
No cry |
1 |
|
|
Moaning |
2 |
|
|
Crying |
3 |
|
|
Screaming |
4 |
|
FACIAL |
Smiling |
0 |
|
|
Composed |
1 |
|
|
Grimace |
2 |
|
VERBAL |
Smiling |
0 |
|
|
Composed |
1 |
|
|
Grimace |
2 |
|
VERBAL |
Positive |
0 |
|
|
None |
1 |
|
|
Complaints other than pain |
1 |
|
|
Pain complaints |
2 |
|
|
Pain & non pain complaints |
2 |
|
TORSO |
Neutral |
1 |
|
|
Shifting |
2 |
|
|
Tense |
2 |
|
|
Shivering |
2 |
|
|
Upright |
2 |
|
|
Restrained |
2 |
|
TOUCH |
Not touching |
1 |
|
|
Reach |
2 |
|
|
Touch |
2 |
|
|
Grab |
2 |
|
|
Restrained |
2 |
|
LEGS |
Neutral |
1 |
|
|
Squimming,kicking |
2 |
|
|
Draw up tensed |
2 |
|
|
Standing |
2 |
|
|
Restrained |
2 |
Fentanyl 0.5 μg/kg was administered IV to treat pain whenever the CHEOPS was greater than 6 or to treat ED score 3 or 4 lasting for more than 3 min.
Modified Aldrete Post Anaesthesia Score
|
PARAMETER |
Description of patient |
Score |
|
Activity level |
Moves all extremities voluntarily/on command |
2 |
|
Moves 2 extremities |
1 |
|
|
Cannot move extremities |
0 |
|
|
Respirations |
Breathes deeply and coughs freely |
2 |
|
Is dyspneic, with shallow, limited breathing |
1 |
|
|
Is apneic |
0 |
|
|
Circulation (blood pressure) |
Is 20 mmHg > preanaesthetic level |
2 |
|
Is 20 to 50 mmHg > preanaesthetic level |
1 |
|
|
Is 50 mmHg > preanaesthetic level |
0 |
|
|
Consciousness |
Is fully awake |
2 |
|
Is arousable on calling |
1 |
|
|
Is not responding |
0 |
|
Oxygen saturation as determined by pulse oximetry |
Has level > 90% when breathing room air |
2 |
|
Requires supplemental O2 to maintain level >90% |
1 |
|
|
Has level < 90% with O2 supplementation |
0
|
Children were considered ready for discharge from the PACU when the modified Aldrete post-anesthesia score is ≥9.
Maximum score- 10 .
Time to Recovery is recorded as the time from extubation to reach the modified aldrete score of > 9.
Incidence of Adverse Events such as nausea, vomiting, oxygen desaturation, shivering, somnolence and hallucination were re-corded.
Statistical analysis was performed with the help GraphPad prism 9 software. Baseline characteristics of both the groups were tabu-lated by descriptive statistics (mean , standard deviation) and fre¬quency table.
Continuous data were compared by Independent sample t test.
Categorical data were analysed by chi squre (x2 ) test.
Significance was defined by P values less than 0.05.
Proforma
Patient Details Group P or F:
Date: ………………… Name: ……………………… I.R.No. ……………..
Age: …… years Sex: Male/Female
Weight:............ kg
Diagnosis:................................ Surgery performed:
…………………………
ASA grade I/II:...........
History
Past illness: ………………………………………………………
Past operation/anesthesia: ………………………………………
Drug allergy: ……………………………………………………
Drug History: ……………………………………………………
General Examination
Mental Status: conscious/cooperative
Pulse:.................... regular/missed
BP: …...………….. RR: ……………………
Temp:
Weight:
Built/Nourishment: ………………………
Teeth: ………………………………..
Mallampatti Class I/II
Spine: ………………………………………………
Tongue/Nail/Conjunctiva: …………………………
JVP/Lymphnode/edema feet: …………………….
RS: …………………………………………
CVS: …………………………………………
Others: …………………………………………
Investigations
Hb: …………….CBC: Blood Group:
……………
Sugar:FBS:….........................PPBS:…………………RBS:
…………….
S.Urea: ………….. S.Creatinine: ………………
S.Electrolytes:……………………………
LFT:...........................................................................
X-ray: ………………………..
USG:………………………………
ECG:......................................................................................
Others:....................................................................................
Anaesthesia Record
General Anaesthesia
Premedication
Inj. Ondansetron hydrochloride : 0.15 mg/kg iv
Inj. Glycopyrrolate: 0.04 mg/kg iv
Preoxygenation done with 100% O2 for 3 min Induction:
Inj Propofol 2mg/kg iv
Inj Atracurium besylate 0.5mg/kg iv
Maintenance : Oxygen+ Nitrous oxide (50:50), sevoflurane and
Inj Atracurium besylate in incremental dose of 0.1 mg/kg iv Ten
min before surgery (according to group allocated)
Group F (n=30): Inj. Fentanyl citrate 1µg/kg iv [ ]
Group K (n=30): Inj. Ketamine 0.5 mg/kg iv [ ]
Reversal : Inj. Neostigmine 0.05mg/kg iv and
Inj. Glycopyrrolate 0.008mg/kg iv
Duration of Surgery
Emergence Time
Time to Extubation
Duration of Anaesthesia
|
SCORE |
5 min |
10 min |
20min |
30 min |
|
1(Asleep) |
|
|
|
|
|
2(Awake but calm) |
|
|
|
|
|
3(Agitated but consolable) |
|
|
|
|
|
4(Severe agitation) |
|
|
|
|
Table 1: Post-Operative Emergence-Delirium Aono`S Four Point Scale
|
S. No. |
PARAMETERS |
5 min |
10 min |
20 min |
30 min |
|
1 |
Cry |
|
|
|
|
|
2 |
Facial expression |
|
|
|
|
|
3 |
Verbal response |
|
|
|
|
|
4 |
Torso |
|
|
|
|
|
5 |
Touch |
|
|
|
|
|
6 |
Legs |
|
|
|
|
Table 2: The Children`s Hospital of Eastern Ontario Pain Scale (CHEPOS)
|
S. No. |
PARAMETERS |
5 min |
10 min |
20 min |
30 min |
|
1 |
Activity level |
|
|
|
|
|
2 |
Respiration |
|
|
|
|
|
3 |
Circulation (BP) |
|
|
|
|
|
4 |
Consciousness |
|
|
|
|
|
5 |
Oxygen saturation |
|
|
|
|
Table 3: Modified Aldrete Post Anaesthesia Score
Time to Recovery
|
Complications |
YES/NO |
|
Nausea |
|
|
Vomiting |
|
|
Oxygen desaturaion |
|
|
Shivering |
|
|
Somnolence |
|
|
Hallucination |
|
Table 4: Adverse Effects
Observation and Results
This prospective study comprised of 60 paediatric patients. Patients were randomaly divided into two Groups, 30 patients in each Group.Group F(n=30) – Inj. Fentanyl 1µg/kg IV Group K(n=30) – Inj. Ketamine hydrochloride 0.5mg/kg iv The data collected from all the selected cases were recorded and tabulated in a Master Chart.
|
Patient data |
Group F |
Group K |
P Value |
|
Number(n) |
30 |
30 |
- |
|
Age (MEAN±SD) |
8±2.38 |
8.46±2.04 |
0.41 |
|
Sex (M:F) |
15:15 |
16:14 |
- |
|
Weight (MEAN±SD) |
20.16±3.99 |
20.3±4.64 |
0.90 |
|
ASA(I:II) |
22:8 |
20:10 |
- |
Table 5: Demographic Data
Demographic data regarding sex, age, weight and ASA grading of patients were comparable in both the Groups. Demographic distribution of patients in both the groups were statistically not significant as p value >0.05.
|
Type of surgery |
Group F |
Group K |
||
|
(n=30) |
% |
(n=30) |
% |
|
|
Adenotonsillectomy |
5 |
16.66 |
5 |
16.66 |
|
Tonsillectomy |
3 |
10 |
6 |
20 |
|
Cleft lip cleft palate surgeries |
4 |
13.33 |
6 |
20 |
|
Circumcision |
6 |
20 |
3 |
10 |
|
Inguinal herniotomy |
8 |
26.66 |
4 |
13.33 |
|
Debridment for septic arthritis |
4 |
13.33 |
6 |
20 |
Table 6: Type of Surgery
|
TIME |
G R O U P S |
Pulse (/min) |
Respiratory rate(/ min) |
SpO2(%) |
SBP (mmHg) |
DBP (mmHg) |
|||||
|
MEAN±S D |
P value |
MEAN ±SD |
P value |
MEAN± SD |
P value |
MEAN± SD |
P value |
MEAN± SD |
P value |
||
|
Baseline |
F |
118.7±6.7 |
0.44 |
23±2 |
0.43 |
99±0.6 |
0.48 |
101±8.1 |
0.96 |
67±6 |
0.12 |
|
K |
117.3±7.6 |
23±1.8 |
99±0.5 |
101±10 |
69±7 |
||||||
|
Immediately after intubation |
F |
121±7.13 |
0.71 |
23±1.6 |
0.63 |
99.3±0.6 |
0.82 |
104±8.3 |
0.07 |
72±10 |
0.59 |
|
K |
120±8 |
24±1.6 |
99.3±0.5 |
101±7.8 |
67±6 |
||||||
|
10 min |
F |
117±7.6 |
0.42 |
23±1.5 |
0.64 |
99.3±0.4 |
0.58 |
101±11 |
0.41 |
66.4±7.13 |
0.15 |
|
K |
119±7.7 |
23±1.3 |
99.2±0.4 |
99±6.4 |
64±3.7 |
||||||
|
20 min |
F |
116±7.4 |
0.65 |
23±1.3 |
0.99 |
99.3±0.5 |
0.41 |
101±5.1 |
0.77 |
67±5 |
0.11 |
|
K |
116±8 |
23±0.9 |
99.2±0.4 |
102±7.4 |
65±4 |
||||||
|
30 min |
F |
116±5.5 |
0.81 |
23±1.2 |
0.20 |
99.1±0.5 |
0.56 |
100±5.7 |
0.83 |
65.9±4.05 |
0.09 |
|
K |
116±6.2 |
22±0.9 |
99±0.3 |
99±6.4 |
64.2±3.6 |
||||||
|
35 min |
F |
114±5.6 |
0.69 |
22±1 |
0.81 |
99±0.5 |
0.55 |
102±7.3 |
0.07 |
65.9±8 |
0.12 |
|
K |
113±6.4 |
22±1 |
99±0.4 |
99±6.4 |
63.4±3.2 |
||||||
|
40 min |
F |
110±12 |
0.68 |
22±1 |
0.42 |
99±0.7 |
0.54 |
100±6.4 |
0.39 |
67±8 |
0.12 |
|
K |
111±6.1 |
22±1 |
99±0.5 |
99±7 |
64±4 |
||||||
|
45 min |
F |
110±4.9 |
0.95 |
22±1 |
0.33 |
99±1 |
0.99 |
100.6±5.6 |
0.07 |
68±7 |
0.43 |
|
K |
110±5.7 |
22±1 |
99±0 |
104±6.3 |
67±4 |
||||||
|
50 min |
F |
113±4.4 |
0.62 |
23±1 |
0.44 |
99±0.3 |
0.19 |
101±5.6 |
0.39 |
65.2±4 |
0.43 |
|
K |
112±5.3 |
22±1 |
99±0.5 |
99±8.2 |
64±3.3 |
||||||
|
55 min |
F |
109±1.4 |
0.14 |
21±1 |
0.30 |
100±0.7 |
0.80 |
93±1.4 |
0.18 |
64±3 |
0.19 |
|
K |
112±1.6 |
23±1 |
100±0.5 |
112±13.4 |
73±7 |
Table 7: Intra Operative Haemodynamic Changes
There were no changes in Pulse rate, Respiratory rate, SpO2, Blood Pressure in both Groups intra operatively and no statistical differences were found.(P >0.05)
|
Group |
Duration of Anaesthesia (min) |
Duration of surgery (min) |
||
|
MEAN±SD |
P value |
MEAN±SD |
P value |
|
|
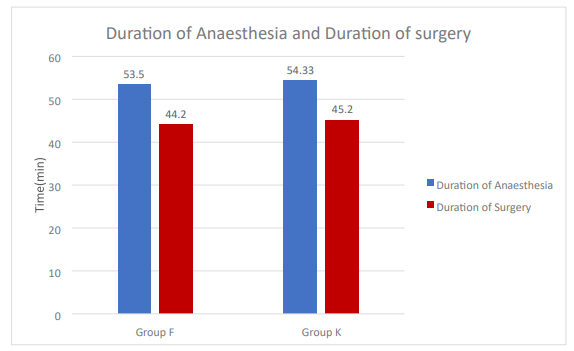
Group F |
53.5±7.31 |
0.62 |
44.2±6.34 |
0.54 |
|
Group K |
54.33±5.87 |
45.2±6.12 |
||
Table 8: Duration of Anaesthesia and Duration of Surgery
In both Groups Duration of Anaesthesia and Duration of surgery were comparable
|
Group |
Time of Emergence (min) |
Time of Extubation (min) |
||
|
MEAN±SD |
P value |
MEAN±SD |
P value |
|
|
Group F |
9.13±1.71 |
<0.001 |
11.3±2.58 |
<0.001 |
|
Group K |
9.76±1.9 |
11.6±1.62 |
||
Table 9: Time of Emergence and Time of Extubation
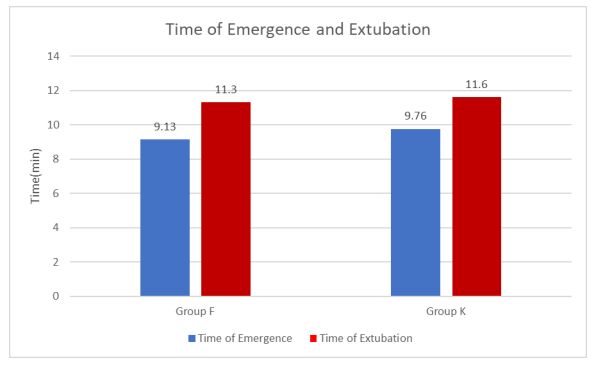
Time of Emergence and time of extubation were delayed in Group K compared to Group F.
|
TIME (min) |
G R O U P S |
Pulse (/min) |
Respiratory rate (/ min) |
SpO2(%) |
SBP (mmHg) |
DBP (mmHg) |
|||||
|
MEAN± SD |
P value |
MEAN± SD |
P value |
MEAN± SD |
P value |
MEAN± SD |
P value |
MEAN± SD |
P value |
||
|
5 min |
F |
101±7.7 |
0.27 |
18.9±1.9 |
0.09 |
99.2±0.5 |
1 |
98.7±6.7 |
0.11 |
64.2±3.7 |
0.38 |
|
K |
103±4.5 |
19.7±1.3 |
99.2±0.7 |
101±7.3 |
|
||||||
|
10 min |
F |
103.3±7.6 |
0.56 |
20.13±2.2 |
0.11 |
99.4±0.5 |
0.06 |
98.2±4.3 |
0.07 |
64.1±2.9 |
0.10 |
|
K |
104.5±7.7 |
21.03±2.1 |
99.1±0.7 |
100.6±5.4 |
65.6±3.78 |
||||||
|
20 min |
F |
103±7.5 |
0.07 |
19.7±1.9 |
0.10 |
99.4±0.5 |
0.11 |
97.2±4.7 |
0.15 |
64.8±2.6 |
0.17 |
|
K |
106.3±6.2 |
20.6±2.2 |
99.2±0.6 |
100.3±10 |
66.7±7 |
||||||
|
30min |
F |
101.7±8 |
0.13 |
19.4±1.8 |
0.15 |
99.3±0.5 |
0.29 |
100±4.5 |
0.66 |
63.2±2.9 |
0.16 |
|
K |
104.3±5.2 |
20.1±1.7 |
99.2±0.6 |
100±4.4 |
64.7±4.9 |
||||||
Table 10: Post-Operative Haemodynamic Changes
There were no changes in Pulse rate, Respiratory rate, SpO2, Blood Pressure in both Groups post operatively.
AONO’s four point scale:
Emergence delirium was assessed using AONO’s four point scale at 5,10,20 and 30 minutes. The score of 3 and 4 are considered as presence of emergence delirium.
|
Four point scale |
5min |
10 min |
20 min |
30 min |
||||
|
Group F (n) (%) |
Group K (n) (%) |
Group F (n) (%) |
Group K (n) (%) |
Group F (n) (%) |
Group K (n) (%) |
Group F (n) (%) |
Group K (n) (%) |
|
|
Score 1 |
22(73.33) |
11(66.66) |
19(63.33) |
8(26.66) |
1(3.33) |
1(3.33) |
0 |
0 |
|
Score 2 |
3(10) |
0 |
8(26.66) |
9(30) |
29(96.66) |
15(50) |
30(100) |
24(80) |
|
Score 3 |
5(16.66) |
19(63.33) |
3(10) |
13(43.33) |
0 |
14(46.66) |
0 |
6(20) |
|
Score 4 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
MEAN±SD |
1.43±0.74 |
2.26±0.96 |
1.46±0.70 |
2.16±0.81 |
1.96±0.19 |
2.43±0.55 |
2.0±0 |
2.2±0.45 |
|
P value |
0.0005 |
0.0007 |
0.0001 |
0.011 |
||||
Table 11: Post-Operative Emergence-Delirium
n=number of pts
Agitation score : score 1- Asleep; score 2-Awake but calm; score 3-Agitated but consolable; score 4-Severely agitated and inconsolable
According to AONO score, Emergence delirium was more in Group K compared to Group F.
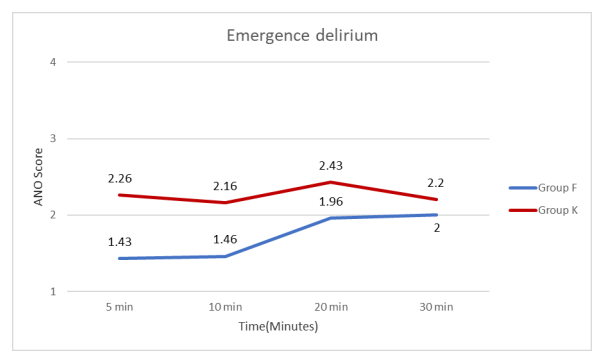
According to Aono score ED was present in 63.33% of patients in Group K & only 16.66% of patients in Group F at 5 min; while it was 43.33% of patients in Group K & only 10% of patients in Group F at 10 min; at 20 min none of the patients were having ED in Group F while it was 46.66% of patients in Group K. The above finding shows ED was more in Group K compared to Group F. Crying, facial expression, verbal statements, position of torso, touching of the wound and movement of legs is used for post-operative pain assessment and it is measured at 5, 10, 20 and 30 min post-operatively. Maximum score-13; minimum score-4: ≥ 6 score require analgesic.
|
CHEOPS |
5min |
10 min |
20 min |
30 min |
||||
|
Group F (n) (%) |
Group K (n) (%) |
Group F (n) (%) |
Group K (n) (%) |
Group F (n) (%) |
Group K (n) (%) |
Group F (n) (%) |
Group K (n) (%) |
|
|
Score 4 |
0 |
0 |
0 |
0 |
1(3.33) |
0 |
6(20) |
2(6.66) |
|
Score 5 |
15(50) |
0 |
23(76.66) |
1(3.33) |
24(80) |
6(20) |
22(73.33) |
12(40) |
|
Score 6 |
9(30) |
11(36.66) |
3(10) |
15(50) |
2(6.66) |
21(70) |
2(6.66) |
16(53.33) |
|
Score 7 |
1(3.33) |
1(3.33) |
1(3.33) |
4(13.33) |
3(10) |
1(3.33) |
0 |
0 |
|
Score 8 |
1(3.33) |
3(10) |
1(3.33) |
5(16.66) |
0 |
2(6.66) |
0 |
0 |
|
Score 9 |
2(6.66) |
6(20) |
0 |
3(10) |
0 |
0 |
0 |
0 |
|
Score 10 |
0 |
6(20) |
0 |
1(3.33) |
0 |
0 |
0 |
0 |
|
Score 11 |
1(3.33) |
3(10) |
2(6.66) |
1(3.33) |
0 |
0 |
0 |
0 |
|
Score 12 |
1(3.33) |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
Score 13 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
MEAN ±SD |
6.16±1.84 |
8.13±1.83 |
5.66±1.62 |
7.03±1.42 |
5.23±0.69 |
5.96±0.70 |
4.86±0.53 |
5.46±0.61 |
|
P value |
0.0001 |
0.001 |
0.0001 |
0.0001 |
||||
Table 12: Cheops (Children’s Hospital of Eastern Ontario Pain Scale)
According to CHEOPS pain score was ≥6 in all patients of Group K while it was only in 15 patients of Group F at 5 min; 29 patients in Group K compared to only 7 patients in Group F at 10 min and at 20 min, 24 patients had CHEOPScore ≥6 in Group K compared to only 5 patients in Group F. While at 30 min, 16 patients in Group K compared to only 2 patients in Group F.
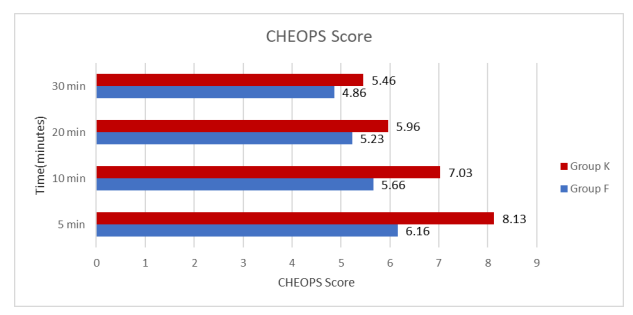
The post operative pain score was compared at 5,10,20 and 30minutes according to the CHEOPS in two Groups. and found that there were higher scores in Ketamine compared to Group F. It is difficult to distinguish between post operative pain and ED in younger children as symptom of both might be similar. In present study pain is not a contributing factor in incidence of ED as Paracetamol suppository was kept after induction of anaesthesia.
|
Modified aldrete post anaesthesia score |
5 min |
10 min |
20 min |
30 min |
||||
|
Group F (n) (%) |
Group K (n) (%) |
Group F (n) (%) |
Group K (n) (%) |
Group F (n) (%) |
Group K (n) (%) |
Group F (n) (%) |
Group K (n) (%) |
|
|
Score 7 |
10(33.33) |
20(66.66) |
2(6.66) |
10(33.33) |
0 |
0 |
0 |
0 |
|
Score 8 |
20(66.66) |
10(33.33) |
28(93.33) |
20(66.66) |
3(10) |
10(33.33) |
0 |
0 |
|
Score 9 |
0 |
0 |
0 |
0 |
27(90) |
20(66.66) |
2(6.66) |
10(33.33) |
|
Score 10 |
0 |
0 |
0 |
0 |
0 |
0 |
28(93.3) |
20(66.66) |
|
MEAN ±SD |
7.66±0.46 |
7.33±0.47 |
7.93±0.19 |
7.66±0.47 |
8.9±0.26 |
8.66±0.47 |
9.93±0.26 |
9.66±0.47 |
|
P value |
0.009 |
0.009 |
0.029 |
0.009 |
||||
Table 13: Modified Aldrete Post Anaesthesia Score
Maximum total score =10; a score of >9 is required for discharge.
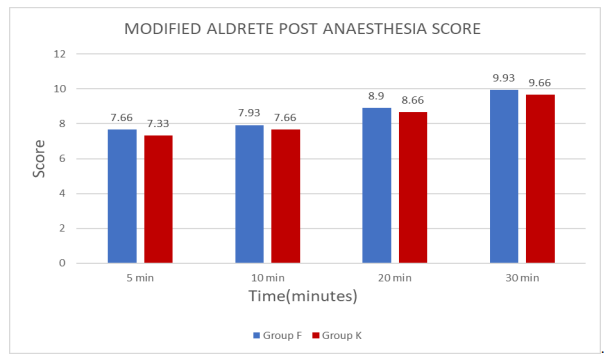
Activity level, Respiration, Circulation (Blood Pressure), Consciousness, O2 Saturation as determined by pulse oximetry were measured at 5, 10, 20 and 30 min post-operatively to document recovery time.
Modified Aldrete score measured at 5, 10, 20 and 30 min post-operatively was more in Group F compared to Group K.
|
Time To Recovery(min) |
Group F |
Group K |
|
MEAN |
19.96 |
22.56 |
|
SD |
2.00 |
2.78 |
|
P VALUE |
0.0001 |
|
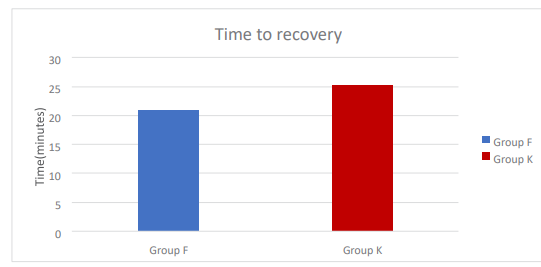
Table 14: Time to Recovery
Recorded as the time from extubation to reach the modified Aldrete score of > 9.
According to modified Aldrete score recovery time was delayed in Group K compared to Group F.
|
Complication |
Group F (n) (%) |
Group K (n) (%) |
|
Nausea |
1(3.33) |
1(3.33) |
|
Vomiting |
1(3.33) |
1(3.33) |
|
Oxygen desaturaion |
0 |
0 |
|
Shivering |
0 |
0 |
|
Somnolence |
0 |
0 |
|
Hallucination |
0 |
0 |
Table 15: Complication
Complications like nausea and vomiting was seen in both the groups in equal number of patients.
Discussion
Emergence delirium(ED) is manifest on recovery of consciousness and usually last for 5-15 min; the child is typically irritable, unco-operative and inconsolable with crying, moaning, kicking and exhibiting generally inappropriate behaviour. Despite its spontaneous resolution, Emergence delirium is still considered as a potentially serious complication because of the risks of self-injury, and because of the stress caused to both caregivers and families.
Non pharmacological interventions involves ensuring patient safety, excluding physical discomfort and reassuring the patient, parents regarding its transient nature; Standard pharmacological interventions such as propofol, a2-adrenoceptor (AR) agonists (clonidine, dexmedetomidine), midazolam, ketamine and fentanyl have been shown to have prophylactic effects in preventing emergence delirium in children.
Earlier studies have shown that ketamine itself is a risk factor for emergence delirium. However recent studies have shown that ketamine when given orally or intravenously in low doses is effective in preventing the occurrence of emergence delirium. Intramuscular injection of ketamine in a relatively low dose (2-3 mg/kg) is effective in uncooperative children as the last resort to avoid inhalation induction by force or for the insertion of an intravenous catheter. Ketamine may be combined with glycopyrrolate to reduce secretions. Ketamine has also been given via the oral, nasal transmucosal, or rectal routes.
Pain is an independent risk factor for emergence delirium especially in pediatric population. So adequate pain relief decreases the incidence of emergence delirium Fentanyl is a phenyl piperidine-derivative synthetic opioid agonist that is structurally related to meperidine. Fentanyl is 50-80 times more potent an analgesic than morphine and has little sedative and hypnotic property. Several studies have shown that NSAIDs like ketorolac and opioids like fentanyl and remifentanyl decreases the incidence of emergence delirium. In our study, Fentanyl is compared with Ketamine with regards to the incidence of post-operative emergence delirium by Aono’s four-point scale, time of extubation, post-operative pain assessment by CHEOPS, discharge from the recovery room criteria by modified Aldrete post-anesthesia score and occurrence of complications from general anesthesia in pediatric patients.
Demographic Data Patients in our study were demographically similar in both groups. There are no statistically significant variations regarding age, body weight and gender.
Surgical Procedures, Duration of Anaesthesia and Duration of Surgery Majority of patients undergoing surgical procedures like adenotonsillectomy, tonsillectomy, cleft lip & cleft palate surgeries, circumcision, inguinal herniotomy and debridment for septic arthritis were included in our study. Mean duration of anaesthesia and mean duration of surgery were comparable in both the groups.
Intraoperative Heamodynamic Data Intraoperative hemodynamic changes (pulse, respiratory rate, blood pressure, SpO2) were recorded. There were no changes in intraoperative hemodynamic changes between both the groups intra operatively and were no statistically significant differences found (P >0.05).
Time of Emergence and Time of Extubation
Time of emergence in Group K (9.76±1.9 min) was more compared to Group F (9.13±1.71 min) with p value <0.001 which was statistically significant. Time of extubation in Group K (11.6±1.62) was more compared to Group F (11.3±2.58) with p value <0.001 which was statistically significant.
Time of emergence and time of extubation both are more with inj. ketamine than inj. fentanyl group.
Kyung Mi Kim et al compare the effect of pre operative midazolam(0.1mg/kg) or ketamine(1mg/kg) on the incidence of emergence agitation following sevoflurane anaesthesia in pediatric patients undergoing ophthalmic surgeries [11].
They found that extubation time in ketamine Group was 15.76±5.61 min.
This finding differs from our study due to dose of ketamine and time of drug given.
There were no changes in pulse rate, respiratory rate, SpO2, blood pressure between both the Groups at 5min,10 min,20 min,30 min post operatively and were no statistically significant differences found (P >0.05).
Post-Operative Emergence-Delirium by Aono’s Four Point Scale to assess incidence of post-operative emergence delirium. The score of 3 and 4 are considered as presence of emergence delirium. In our study according to Aono score ED was present in 63.33% of patients in Group K & only 16.66% of patients in Group F at 5 min; while it was 43.33% of patients in Group K & only 10% of patients in Group F at 10 min; at 20 min none of the patients were having ED in Group F while it was 46.66% of patients in Group K. The above finding shows ED was more in Group K compared to Group F.
Ashraf Arafat et al found the incidence of emergence delirium was significantly less in children who received either ketamine or fentanyl (15%, 17.5%) when compared to the incidence of emergence delirium in placebo group (42.5%) [2].
Manal et al in their study compared the effect of intravenous injection of small dose of propofol, fentanyl or ketamine at the end of surgery, just before the discontinuation of sevoflurane on the incidence and severity of sevoflurane emergence agitation in children undergoing hypospadias repair operations [15]. In their study the incidence of emergence agitation was significantly lower in propofol and fentanyl group when compared to ketamine and control group.
Consistent with this study the number of patients with emergence delirium is higher in ketamine group when compared to fentanyl group. However, conflicting results have been reported by Chen et al. who demonstrated that iv administration of 0.25 mg/kg ketamine (maximum 7.5mg) in combination with 0.5 µg/kg of fentanyl prior to the end of sevoflurane-remifentanil based anesthesia was not effective in preventing emergence delirium in un-pre-medicated children who underwent cataract surgery compared to either 0.05 mg/kg midazolam or 1 mg/kg propofol in combination with 0.5 µg/kg of fentanyl. We have used 0.5 mg/kg ketamine and 1µg/kg fentanyl in present study.
Cravero et al have shown that addition of fentanyl 1 µg/kg iv given 10 min before the discontinuation of inhaled sevoflurane anesthesia decreased incidence of post-operative agitation from 56% to 12% in children scheduled for magnetic resonance imaging scans without any surgical intervention [21]. In our study also administration of 1 µg/kg fentanyl towards the end of sevoflurane anesthesia decreases the incidence of emergence delirium which correlates with this study.
The time interval for measuring the incidence of EA, which is an important factor was chosen to be within 30 min during PACU stay according to results of Cole et al., who scored children every 10 min on arrival in PACU up to 1 hour and found that the peak of agitation occurs in the first 30 min after admission.
Post-Operative Pain Assessment by CHEOP Score is found to be higher in ketamine group at 5,10,20 and 30 minutes. There is significant difference at 5 minutes (6.16±1.84 in fentanyl group vs 8.13±1.83 in ketamine group) with a p value of 0.0001, at 10 minutes (5.66±1.62 in fentanyl group vs 7.03±1.42 in ketamine group) with a p value of 0.001, at 20 minutes (5.23±0.69 in fentanyl group vs 5.96±0.70 in ketamine group) with a p value of 0.0001 and at 30 minutes (4.86±0.53 in fentanyl group vs 5.46±0.61in ketamine group) with a p value of 0.0001 which is statistically significant.
Finding of our study differ form study of Ashraf Arafat et al there was no significant difference between the three groups at 5,10,20and 30 min postoperatively (P>0.05) [2]. It is often difficult to distinguish between post-operative pain and EA in younger children as symptoms of both might be similar so that different assessments tools have been used by different investigators to differentiate between the two. Although post-operative pain is regarded as a contributing factor in the etiology of EA, there are more supporting reports of increased EA after sevoflurane, in pain-free children even if adequate analgesia given intra-operatively or even if regional block was applied.
Therefore, pain cannot be considered as the sole contributing factor to EA. However, pain was probably not a contributing factor in the incidence of EA in the current study, as Paracetamol suppository was kept after induction of anesthesia, consequently, addition of a small dose of either fentanyl or ketamine to sevoflurane anesthesia can be considered even in the absence of substantial post-operative pain to decrease the incidence of EA.
Recovery Time was prolonged in Ketamine group (22.56±2.78 min) than in fentanyl group (19.96±2.00 min) and the data are statistically significant with a p value of 0.0001.
Manal M. Rashad, Dalal E.M et al studed the inj ketamine(0.25mg/ kg) and inj. fentanyl (1µg/kg) in pediatric patients aged 1-3 years for their effect on sevoflurane emergence agitation given just before discontinuation of sevoflurane [15]. They found time for awakening was significantly prolonged in both the drug groups versus control group, due to study drug was given just before the end of anaesthesia in their study.
A study by Abu-Shahwan and Chowdary reported that an iv injection of ketamine 0.25 mg/kg, 10 min before the end of surgery in young children pre-medicated with midazolam for dental operation reduced the incidence of emergence delirium under general anesthesia with sevoflurane without a delay in recovery [14].
Finding of present study might differ from other studies because of the variations in study design; characteristics of patient population, premedication given, type of surgical procedures, the route and timing of administration of the study drugs and lastly criteria used to define and assess the phenomenon of emergence delirium by different assessment tools.
Complication like nausea and vomiting was seen in both the groups in equal number of patients.Complication like Oxygen desaturation, shivering, somnolence and hallucination not seen in either groups.
Limitation of present study is small sample size, not double blinded and patients recruited for the study are children aged 5 to 12 years. We did not used PAED as Aono score was easily applicable.
Summary and Conclusion
This prospective observational study was carried out at our tertiary care center. A total of 60 pediatric patients aged 5-12 years undergoing various elective surgeries under general anaesthesia were included.
Patients were randomly divided into two groups, each group included 30 patients.
Group F(n=30) – Inj. Fentanyl citrate 1µg/kg iv.
Group K(n=30) – Inj. Ketamine hydrochloride 0.5mg/kg iv.
A detailed preanesthetic evaluation of all patients were done. All routine investigations were carried out and informed consent from each patient`s parents was taken. In the operation theatre, standard monitors were attached and iv line was taken. Baseline vitals were noted.
All patients premedicated with:
-Inj. Glycopyrrolate 0.004 mg/kg iv
-Inj. Ondansetron hydrochloride 0.08 mg/kg iv
Preoxygenation done with 100 O2 for 3 min.
Standard general anaesthesia was given.
Paracetamol suppository 15mg/kg was kept after induction.
Intraoperative hemodynamic changes (pulse, respiratory rate, blood pressure, SpO2) were recorded.
Ten minutes before the end of surgery, the study drugs were injected intravenously according to the allocated group. Time of emergence, time of extubation, the incidence of post-operative emergence delirium by Aono’s four point scale, post-operative pain assessment by CHEOPS, discharge from PACU by modified Aldrete score and recovery time were observed.
The demographic data was similar in both the groups with respect to age, sex, weight and ASA grade.
Duration of Anaesthesia and Duration of surgery were comparable in both Groups.
Emergence time was delayed in Group K (9.76±1.9 min) compared to Group F (9.13±1.71 min).
Time of extubation was more in Group K (11.6±1.62 min) compared to Group F (11.3±2.58 min).
Post-operative hemodynamic changes (pulse, respiratory rate, blood pressure, SpO2) were comparable in both Groups.
The primary outcome of the study is the incidence of post-operative emergence delirium, which was assessed every 5 min during the first 30 min using Aono’s four point scale which is higher with Group K compared to Group F.
The Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS) was higher with Ketamine group compared to Fentanyl group.
Children were considered ready for discharge from PACU when the modified
Aldrete post-anesthesia score is ≥9, time to achieve this score is recorded as time of recovery, which is more in Group K (22.56±2.78 min) compared to Group F(19.96±2.00 min).
Complications like nausea and vomiting was seen in both the groups in equal number of patients.
To conclude Fentanyl is effective in decreasing the occurrence of emergence delirium with faster emergence, extubation and recovery compared to Ketamine given 10 min before end of surgery [41].
References
- Coté, C. J., Lerman, J., & Anderson, B. (Eds.). (2024). A Practice of Anesthesia for Infants and Children, E-Book.
- Abdelhalim, A. A., & Alarfaj, A. M. (2013). The effect of ketamine versus fentanyl on the incidence of emergence agitation after sevoflurane anesthesia in pediatric patients undergoing tonsillectomy with or without adenoidectomy. Saudi journal of anaesthesia, 7(4), 392-398.
- Forkin, K. T., & Nemergut, E. C. (2016). Miller’s anesthesia.Anesthesiology, 124(4), 977-978.
- Kararmaz, A., Kaya, S., Turhanoglu, S., & Ozyilmaz, M. A. (2004). Oral ketamine premedication can prevent emergence agitation in children after desflurane anaesthesia. Pediatric Anesthesia, 14(6), 477-482.
- Khattab, A. M., & El-Seify, Z. A. (2009). Sevoflurane-emergence agitation: Effect of supplementary low-dose oral ketamine premedication in preschool children undergoing dental surgery. Saudi Journal of Anaesthesia, 3(2), 61-66.
- Cohen, I. T., Hannallah, R. S., & Hummer, K. A. (2001). The incidence of emergence agitation associated with desflurane anesthesia in children is reduced by fentanyl. Anesthesia & analgesia, 93(1), 88-91.
- Cravero, J. P., Beach, M., Thyr, B., & Whalen, K. (2003). The effect of small dose fentanyl on the emergence characteristics of pediatric patients after sevoflurane anesthesia without surgery. Anesthesia & Analgesia, 97(2), 364-367.
- Cohen, I. T., Finkel, J. C., Hannallah, R. S., Hummer, K. A., & Patel, K. M. (2002). The effect of fentanyl on the emergence characteristics after desflurane or sevoflurane anesthesia in children. Anesthesia & Analgesia, 94(5), 1178-1181.
- Chen, J., Li, W., Hu, X., & Wang, D. (2010). Emergence agitation after cataract surgery in children: a comparison of midazolam, propofol and ketamine. Pediatric Anesthesia, 20(9), 873-879.
- Fazi, L., Jantzen, E. C., Rose, J. B., Kurth, C. D., & Watcha, M.
F. (2001). A comparison of oral clonidine and oral midazolam as preanesthetic medications in the pediatric tonsillectomy patient. Anesthesia & Analgesia, 92(1), 56-61.
- Kim, K. M., Lee, K. H., Kim, Y. H., Ko, M. J., Jung, J. W.,& Kang, E. (2016). Comparison of effects of intravenous midazolam and ketamine on emergence agitation in children: randomized controlled trial. Journal of International medical research, 44(2), 258-266.
- Dalens, B. J., Pinard, A. M., Létourneau, D. R., Albert, N. T., & Truchon, R. J. (2006). Prevention of emergence agitation after sevoflurane anesthesia for pediatric cerebral magnetic resonance imaging by small doses of ketamine or nalbuphine administered just before discontinuing anesthesia. Anesthesia & Analgesia, 102(4), 1056-1061.
- Lee, Y. S., Kim, W. Y., Choi, J. H., Son, J. H., Kim, J. H., &Park, Y. C. (2010). The effect of ketamine on the incidence of emergence agitation in children undergoing tonsillectomy and adenoidectomy under sevoflurane general anesthesia. Korean journal of anesthesiology, 58(5), 440-445.
- ABUâ?SHAHWAN, I. B. R. A. H. I. M., & Chowdary, K.(2007). Ketamine is effective in decreasing the incidence of emergence agitation in children undergoing dental repair under sevoflurane general anesthesia. Pediatric Anesthesia, 17(9), 846-850.
- Rashad, M. M., & Soud, D. E. (2014). The effect of different drugs on sevoflurane emergence agitation in pediatric patients undergoing hypospadias repair surgery. Egyptian Journal of Anaesthesia, 30(2), 123-127.
- Kim, M. S., Moon, B. E., Kim, H., & Lee, J. R. (2013).Comparison of propofol and fentanyl administered at the end of anaesthesia for prevention of emergence agitation after sevoflurane anaesthesia in children. British journal of anaesthesia, 110(2), 274-280.
- Dahmani, S., Stany, I., Brasher, C., Lejeune, C., Bruneau, B., Wood, C., ... & Murat, I. J. B. J. A. (2010). Pharmacological prevention of sevoflurane-and desflurane-related emergence agitation in children: a meta-analysis of published studies. British journal of anaesthesia, 104(2), 216-223.
- Lee, Y. S., Kim, W. Y., Choi, J. H., Son, J. H., Kim, J. H., &Park, Y. C. (2010). The effect of ketamine on the incidence of emergence agitation in children undergoing tonsillectomy and adenoidectomy under sevoflurane general anesthesia. Korean journal of anesthesiology, 58(5), 440-445.
- Kararmaz, A., Kaya, S., Turhanoglu, S., & Ozyilmaz, M. A. (2004). Oral ketamine premedication can prevent emergence agitation in children after desflurane anaesthesia. Pediatric Anesthesia, 14(6), 477-482.
- Cravero, J. P., Beach, M., Thyr, B., & Whalen, K. (2003). The effect of small dose fentanyl on the emergence characteristics of pediatric patients after sevoflurane anesthesia without surgery. Anesthesia & Analgesia, 97(2), 364-367.
- Cohen, I. T., Finkel, J. C., Hannallah, R. S., Hummer, K. A., & Patel, K. M. (2002). The effect of fentanyl on the emergence characteristics after desflurane or sevoflurane anesthesia in children. Anesthesia & Analgesia, 94(5), 1178-1181.
- Sikich, N., & Lerman, J. (2004). Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale. Anesthesiology, 100(5), 1138-1145.
- Aono, J., Ueda, W., Mamiya, K., Takimoto, E., & Manabe, M. (1997). Greater incidence of delirium during recovery from sevoflurane anesthesia in preschool boys. Anesthesiology, 87(6), 1298-1300.
- Bajwa, S. A., Costi, D., & Cyna, A. M. (2010). A comparison of emergence delirium scales following general anesthesia in children. Pediatric Anesthesia, 20(8), 704-711.
- Cravero, J. P., Beach, M., Dodge, C. P., & Whalen, K. (2000). Emergence characteristics of sevoflurane compared to halothane in pediatric patients undergoing bilateral pressure equalization tube insertion. Journal of clinical anesthesia, 12(5), 397-401.
- Kawaraguchi, Y., Miyamoto, Y., Fukumitsu, K., Taniguchi, A., Hirao, O., Kitamura, S., & Kinouchi, K. (2002). The effect of ketamine on reducing postoperative agitation after sevoflurane anesthesia in pediatric strabismus surgery. Masui. The Japanese Journal of Anesthesiology, 51(12), 1343-1348.
- Oh, A. Y., Seo, K. S., Kim, S. D., Kim, C. S., & Kim, H. S.(2005). Delayed emergence process does not result in a lower incidence of emergence agitation after sevoflurane anesthesia in children. Acta anaesthesiologica scandinavica, 49(3), 297-299.
- Viswanath, O., Kerner, B., Jean, Y. K., Soto, R., & Rosen, G. (2015). Emergence delirium: a narrative review. J Anesthesiol Clin Sci, 4(2), e1-e8.
- Thomas, D., Lagoo, J., & Kilpadi, K. (2015). Emergence agitation in children after sevoflurane anaesthesia: a comparative evaluation of ketamine and varying doses of fentanyl. Sri Lankan Journal of Anaesthesiology, 23(1).
- Cole, J. W., Murray, D. J., McALLISTER, J. D., & Hirshberg,G. E. (2002). Emergence behaviour in children: defining the incidence of excitement and agitation following anaesthesia. Pediatric Anesthesia, 12(5), 442-447.
- Lepouse, C., Lautner, C. A., Liu, L., Gomis, P., & Leon, A. (2006). Emergence delirium in adults in the post-anaesthesia care unit. BJA: British Journal of Anaesthesia, 96(6), 747-753.
- Vlajkovic, G. P., & Sindjelic, R. P. (2007). Emergence delirium in children: many questions, few answers. Anesthesia & Analgesia, 104(1), 84-91.
- Kain, Z. N., Caldwell-Andrews, A. A., Maranets, I., McClain, B., Gaal, D., Mayes, L. C., ... & Zhang, H. (2004). Preoperative anxiety and emergence delirium and postoperative maladaptive behaviors. Anesthesia & Analgesia, 99(6), 1648-1654.
- Inomata, S., Maeda, T., Shimizu, T., Satsumae, T., & Tanaka,M. (2010). Effects of fentanyl infusion on tracheal intubation and emergence agitation in preschool children anaesthetized with sevoflurane. British journal of anaesthesia, 105(3), 361-367.
- Beskow, A., & Westrin, P. (1999). Sevoflurane causes more postoperative agitation in children than does halothane. Acta anaesthesiologica scandinavica, 43(5), 536-541.
- Hallén, J., Rawal, N., & Gupta, A. (2001). Postoperative recovery following outpatient pediatric myringotomy: a comparison between sevoflurane and halothane. Journal of clinical anesthesia, 13(3), 161-166.
- Welborn, L. G., Hannallah, R. S., Norden, J. M., Ruttimann,U. E., & Callan, C. M. (1996). Comparison of emergence and recovery characteristics of sevoflurane, desflurane, and halothane in pediatric ambulatory patients. Anesthesia & Analgesia, 83(5), 917-920.
- Stoelting, R. K., & Hillier, S. C. (2012). Pharmacology and physiology in anesthetic practice. Lippincott Williams & Wilkins.
- TK Agasti: Test Book of Anesthesia: First Edition: 2011. Chapter 14. Page no358.
- Wylie and Churchill Devidson`s A practice of Anaesthesia (Seventh Edition) Chapter 58&59.
- Dichâ?Nielsen, J. O., Svendsen, L. B., & Berthelsen, P. (1992). Intramuscular lowâ?dose ketamine versus pethidine for postoperative pain treatment after thoracic surgery. Acta anaesthesiologica scandinavica, 36(6), 583-587.