
Advancements in Journal of Urology and Nephrology(AJUN)
ISSN: 2689-8616 | DOI: 10.33140/AJUN
Impact Factor: 1.0



Research Article - (2025) Volume 7, Issue 1
Distribution of Cancer of the Kidney and Cancer of the Penis in Jamaica 2008
Received Date: Sep 09, 2025 / Accepted Date: Oct 06, 2025 / Published Date: Oct 15, 2025
Copyright: ©Â©2025 LA McLish. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Mclish, L. A. (2025). Distribution of Cancer of the Kidney and Cancer of the Penis in Jamaica 2008. Adv J Uro Nephro, 7 (1), 1-8.
Abstract
Objective: To investigate the distribution of cancer of the kidney and cancer of the penis in Jamaica in 2008.
Methods: This study encapsulated all fourteen parishes. Data was obtained from the Jamaica Cancer Registry located in the Pathology Department of the University Hospital of the West Indies. Population denominators were obtained from the 2011 census taken by the Statistical Institute of Jamaica. The statistical packages which were used to analyze the data were SPSS and Microsoft excel.
Results: The mean age at which cancer of the kidney was diagnosed in Jamaica 2008 was (47.04 ± 4.54) years. None of the individuals diagnosed in 2008 were smokers. The crude incidence rate (CIR) is an estimate of the probability that a person will develop cancer. In Jamaica in 2008 the CIR for males was 1.1 and for females it was 0.7 hence (male/ female ratio, 1.57). The age standardized incidence rate (ASIR) of cancer of the kidney in Jamaica 2008 was0.9 (95% CI, 0.53 – 1.27). In Jamaica 2008 the ASIR for cancer of the kidney in males was 1.3 (95% CI, 0.67 – 1.93) and that for females was 0.8 (95% CI, 0.31 – 1.29). The distribution of cancer of the kidney across all parishes in Jamaica 2008 was investigated using the CIR. The highest probability of developing cancer of the kidney was Kingston and St. Andrew (2.0), then St. Catherine (1.2), St. Thomas (1.1), Manchester (1.1), St. Mary (0.9), St. Elizabeth (0.7) and St.Ann (0.6).
The mean age at which penile cancer was diagnosed was (55.92 ± 4.69) years in Jamaica 2008. In 2008 the CIR of penile cancer in Jamaica was 0.9 and the ASIR was 1.5 (95% CI, 0.95 – 2.05). The highest probability of developing cancer of the penis was in Kingston and St. Andrew (2.2), then St. Catherine (1.2), Manchester (1.0) and Clarendon (0.8).
Conclusion: In mitigating cancer of the kidney and cancer of the penis the public should be educated regarding the potential risk factors. In the case of cancer of the kidney these include advancing age, male gender etc. and in the case of cancer of the penis these include human papillomavirus infection, large number of sexual partners etc. Circumcision in childhood or adolescent should be promoted as it can drastically reduce the risk of penile cancer. Screening of these cancers should be facilitated by the various health administrators and different regions (parishes) targeted as this will reduce the financial burden associated with these cancers.
Keywords
Registry, Cancer, Crude Incidence Rate, Age Standardized Incidence Rate, Probability
Introduction
Since the inception of the Jamaica Cancer Registry in 1958 the incidence of cancer in Jamaica has been monitored by reports being produced regularly [1]. These reports are based upon the incidence of cancer in males and females in Kingston and St. Andrew which forms the population base of the registry [1,2]. Gibson et al. determined that cancer of the kidney and other unspecified urinary organs in the case of males had a crude incidence rate of 1.9 and an age standardized rate of 2.0 for the period 2003 to 2007 [2]. In the case of females for this period the crude incidence rate was 1.4 and the age standardized rate was 1.5. Gibson et al. also determined for the period 2003 to 2007 that cancer of the penis had a crude incidence rate of 1.2 and an age standardized rate of 1.2.
This present study has been undertaken to investigate the distribution of cancer of the kidney and cancer of the penis across all fourteen parishes in Jamaica in the year 2008.
Methods
Study Population
This research project consists of persons from all parishes in Jamaica. A map of Jamaica is shown in figure 1 [3].

Figure 1: Map of Jamaica showing all the parishes
Data was obtained from the Jamaica Cancer Registry located in the Pathology Department of the University Hospital of the West Indies. The methodology of the registry has been previously stated [4,5]. Cases are registered from information gathered from public and private hospitals and general practitioners in Kingston and St. Andrew then verified by pathologists at Jamaica Cancer Registry in accordance with standard techniques of registration [6].
Data Extraction
Variables that were obtained from the Jamaica Cancer Registry included cancer code, date of diagnosis, age at diagnosis, permanent residence, parish of birth, diagnosis, gender, smoking status, source of case and date of death. The codes used for the classification of the various types of cancers were cross-checked using the tenth edition of the International Statistical Classification of Diseases and Related Health Problems (ICD – 10) [7]. Population denominators were obtained from the 2011 census taken by the Statistical Institute of Jamaica, Kingston, Jamaica [8].
Statistical Analysis
The statistical packages which were used to analyze the collected data were SPSS and Microsoft excel. The data was initially stored in an excel database. The crude incidence rates (CIR) were determined as well as the age specific rates and the age standardized rates with the associated 95% confidence intervals. The CIR was calculated by dividing the total number of cases of cancer diagnosed in a specific population by the size of the population and then multiplying the result by 100,000 [1,2]. The direct method was used to determine the age standardized rates as described by Boyle and Parkin [9]. The WHO New World Standard Population produced by the National Cancer Institute of United States of America was used to calculate the age standardized rates [10].
Results
|
Age/yr |
Frequency |
||
|
Both Genders |
Male |
Female |
|
|
0 – 4 |
3 |
1 |
2 |
|
5 – 9 |
0 |
0 |
0 |
|
10 – 14 |
0 |
0 |
0 |
|
15 – 19 |
0 |
0 |
0 |
|
20 – 24 |
1 |
0 |
1 |
|
25 – 29 |
0 |
0 |
0 |
|
30 – 34 |
2 |
1 |
1 |
|
35 – 39 |
2 |
0 |
2 |
|
40 – 44 |
2 |
0 |
2 |
|
45 – 49 |
3 |
3 |
0 |
|
50 – 54 |
2 |
1 |
1 |
|
55 – 59 |
1 |
1 |
0 |
|
60 – 64 |
2 |
2 |
0 |
|
65 – 69 |
3 |
2 |
1 |
|
70 – 74 |
2 |
2 |
0 |
|
75 – 79 |
1 |
1 |
0 |
|
80 – 84 |
0 |
0 |
0 |
|
85 – 89 |
1 |
1 |
0 |
|
90 – 94 |
0 |
0 |
0 |
|
95+ |
0 |
0 |
0 |
|
TOTAL (N) |
25 |
15 |
10 |
Table 1. Frequency table showing grouped data of persons diagnosed with Cancer of Kidney in Jamaica 2008
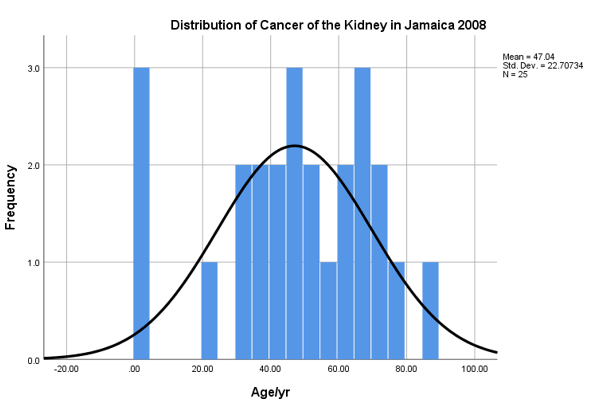
Figure 2: Histogram Showing Distribution of Cancer of the Kidney in Jamaica 2008
|
Age Group (yr) |
Number of cases |
Person-years |
Age Specific Rate |
|
0 – 4 |
3 |
209871 |
1.4 |
|
5 – 9 |
0 |
226380 |
0 |
|
10 – 14 |
0 |
266589 |
0 |
|
15 – 19 |
0 |
274660 |
0 |
|
20 – 24 |
1 |
250713 |
0.4 |
|
25 – 29 |
0 |
226119 |
0 |
|
30 – 34 |
2 |
185496 |
1.1 |
|
35 – 39 |
2 |
183756 |
1.1 |
|
40 – 44 |
2 |
173924 |
1.1 |
|
45 – 49 |
3 |
155389 |
1.9 |
|
50 – 54 |
2 |
137895 |
1.5 |
|
55 – 59 |
1 |
100798 |
1.0 |
|
60 – 64 |
2 |
88057 |
2.3 |
|
65 – 69 |
3 |
65164 |
4.6 |
|
70 – 74 |
2 |
51274 |
3.9 |
|
75 – 79 |
1 |
42760 |
2.3 |
|
80 – 84 |
0 |
30736 |
0 |
|
85 – 89 |
1 |
18457 |
5.4 |
|
90 – 94 |
0 |
6920 |
0 |
|
95+ |
0 |
3027 |
0 |
|
TOTAL (N) |
25 |
2697985 |
|
Table 2: Age-Specific Incidence Rates for Cancer of the Kidney in Jamaica 2008
|
Age Group (yr) |
Age-Specific Rate |
WHO Standard |
Population (%) |
|
0 – 4 |
1.4 |
8.860 |
0.12 |
|
5 – 9 |
0 |
8.690 |
0 |
|
10 – 14 |
0 |
8.600 |
0 |
|
15 – 19 |
0 |
8.470 |
0 |
|
20 – 24 |
0.4 |
8.220 |
0.03 |
|
25 – 29 |
0 |
7.930 |
0 |
|
30 – 34 |
1.1 |
7.610 |
0.084 |
|
35 – 39 |
1.1 |
7.150 |
0.079 |
|
40 – 44 |
1.1 |
6.590 |
0.072 |
|
45 – 49 |
1.9 |
6.040 |
0.11 |
|
50 – 54 |
1.5 |
5.370 |
0.081 |
|
55 – 59 |
1.0 |
4.550 |
0.046 |
|
60 – 64 |
2.3 |
3.720 |
0.086 |
|
65 – 69 |
4.6 |
2.960 |
0.14 |
|
70 – 74 |
3.9 |
2.210 |
0.086 |
|
75 – 79 |
2.3 |
1.520 |
0 |
|
80 – 84 |
0 |
0.910 |
0 |
|
85 – 89 |
5.4 |
0.440 |
0 |
|
90 – 94 |
0 |
0.150 |
0 |
|
95+ |
0 |
0.045 |
0 |
|
ASR |
|
|
0.9 |
Table 3: Determination of the Age-Standardized Incidence Rate (ASIR) for Cancer of the Kidney in Jamaica 2008
|
Age Class (yr) |
Age-specific rate per 100,000 (ai) |
World Standard Population (wi) |
Person-years (ni) |
ð´ ðÂÂ??ðÂÂ??ðÂÂ?¤2 × 100000 � ðÂÂ?? ðÂÂ??ðÂÂ?? ðÂÂ??=1 |
|
0 – 4 |
1.4 |
8860 |
209871 |
52.37 |
|
5 – 9 |
0 |
8690 |
226380 |
0 |
|
10 – 14 |
0 |
8600 |
266589 |
0 |
|
15 – 19 |
0 |
8470 |
274660 |
0 |
|
20 – 24 |
0.4 |
8220 |
250713 |
10780198.87 |
|
25 – 29 |
0 |
7930 |
226119 |
0 |
|
30 – 34 |
1.1 |
7610 |
185496 |
34342147.54 |
|
35 – 39 |
1.1 |
7150 |
183756 |
30602946.30 |
|
40 – 44 |
1.1 |
6590 |
173924 |
27466542.86 |
|
45 – 49 |
1.9 |
6040 |
155389 |
44607430.38 |
|
50 – 54 |
1.5 |
5370 |
137895 |
31368323.72 |
|
55 – 59 |
1.0 |
4550 |
100798 |
20538601.96 |
|
60 – 64 |
2.3 |
3720 |
88057 |
36145133.27 |
|
65 – 69 |
4.6 |
2960 |
65164 |
61849119.15 |
|
70 – 74 |
3.9 |
2210 |
51274 |
37149412.96 |
|
75 – 79 |
2.3 |
1520 |
42760 |
12427315.25 |
|
80 – 84 |
0 |
910 |
30736 |
0 |
|
85 – 89 |
5.4 |
440 |
18457 |
5664192.45 |
|
90 – 94 |
0 |
150 |
6920 |
0 |
|
95+ |
0 |
45 |
3027 |
0 |
|
TOTAL (N) |
|
100035 |
|
352941417.10 |
![]()
Table 4. Determination of the variance (σ2) for the Age-Standardized Incidence Rate for Cancer of the Kidney using the Poisson approximation in Jamaica 2008
|
Parish |
Cancer Cases |
Population Size |
Crude Incidence Rate |
|
Kingston and St. Andrew |
13 |
662426 |
2.0 |
|
St. Catherine |
6 |
516218 |
1.2 |
|
St. Thomas |
1 |
93902 |
1.1 |
|
Manchester |
2 |
189797 |
1.1 |
|
St. Mary |
1 |
113615 |
0.9 |
|
St. Elizabeth |
1 |
150205 |
0.7 |
|
St. Ann |
1 |
172362 |
0.6 |
|
Clarendon |
0 |
245103 |
0 |
|
Portland |
0 |
81744 |
0 |
|
Westmoreland |
0 |
144103 |
0 |
|
St. James |
0 |
183811 |
0 |
|
Trelawny |
0 |
75164 |
0 |
|
Hanover |
0 |
69533 |
0 |
Table 5: Comparing the Crude Incidence Rate of Cancer of the Kidney for all Parishes in Jamaica 2008
|
Age /yr |
Frequency |
|
0 – 4 |
0 |
|
5 – 9 |
0 |
|
10 – 14 |
0 |
|
15 – 19 |
0 |
|
20 – 24 |
1 |
|
25 – 29 |
0 |
|
30 – 34 |
0 |
|
35 – 39 |
1 |
|
40 – 44 |
0 |
|
45 – 49 |
1 |
|
50 – 54 |
2 |
|
55 – 59 |
2 |
|
60 – 64 |
3 |
|
65 – 69 |
0 |
|
70 – 74 |
0 |
|
75 – 79 |
1 |
|
80 – 84 |
0 |
|
85 – 89 |
1 |
|
90 – 94 |
0 |
|
95+ |
0 |
|
TOTAL (N) |
12 |
Table 6: Frequency Table Showing Grouped Data of Men Diagnosed with Cancer of the Penis in Jamaica 2008
|
Parish |
Cancer Cases |
Population Size |
Crude Incidence Rate |
|
Kingston and St. Andrew |
7 |
319211 |
2.2 |
|
St. Catherine |
3 |
250358 |
1.2 |
|
Manchester |
1 |
95403 |
1.0 |
|
Clarendon |
1 |
123791 |
0.8 |
|
St. Mary |
0 |
57029 |
0 |
|
St. Elizabeth |
0 |
76530 |
0 |
|
St. Ann |
0 |
86662 |
0 |
|
St. Thomas |
0 |
46959 |
0 |
|
Portland |
0 |
41294 |
0 |
|
Westmoreland |
0 |
73681 |
0 |
|
St. James |
0 |
90450 |
0 |
|
Trelawny |
0 |
38102 |
0 |
|
Hanover |
0 |
35063 |
0 |
Table 7: Comparing the Crude Incidence Rate of Cancer of the Penis for all Parishes in Jamaica 2008
Discussion
From table 1 it can be deduced that in Jamaica in 2008 the highest frequency of cancer of the kidney occurred in males compared to females. In males the highest frequency occurred within the age group 45 years to 49 years. In females the highest frequency occurred in the age group 35 years to 44 years. The table also shows that onset of renal cell carcinoma (RCC) is as early as 0 to 4 years for both genders. The histogram in figure 2 shows the age distribution of cancer of the kidney in Jamaica in 2008. The distribution was negatively skewed having a value of -0.576 and the mean age that cancer of the kidney was diagnosed was (47.04 ± 4.54) years. Kidney cancer is the 15th most common cancer worldwide with higher incidence in developed countries [11]. The risk of kidney cancer increases with advancing age, male gender and smoking [12]. None of the individuals diagnosed in Jamaica in 2008 were smokers. The crude incidence rate (CIR) is an estimate of the probability that a person will develop cancer. In Jamaica in 2008 the CIR for males was 1.1 and for females it was 0.7 hence (male/female ratio, 1.57). Barahman et al. stated that RCC is higher in men than women (male/female ratio, 1.5) and the mortality rate is higher in men than women [13].
Other potential risk factors include ethnicity, hypertension and obesity [14-16]. According to Hao et al., kidney cancer has been found to be associated with occupational exposure to trichloro- ethylene [17]. In table 2 the age specific incidence rates show that as age increases the probability of developing cancer of the kid- ney increases. This can be observed as in the age group 30 years to 34 years the age specific incidence rate is 1.1 however in the age group 65 years to 69 years it is now 4.6 and in the age group 85 years to 89 years the age specific incidence rate is now 5.4 per 100000 persons. Table 3 shows how the age standardized in- cidence rate (ASIR) of cancer of the kidney was determined for Jamaica in 2008. The ASIR was determined to be 0.9 (95% CI, 0.53 – 1.27). Table 4 shows how the variance and hence the 95% confidence interval was determined. Hao et al. determined the global ASIR of kidney cancer in 2021 to be 4.52 per 100,000 per- sons (95% UI, 4.26 – 4.75) [17]. Hao et al. in 2021 found that in the Caribbean the ASIR was 3.06 per 100,000 persons (95% UI, 2.69 – 3.44) and that in Central Sub-Saharan Africa to be 0.95 per 100,000 persons (95% UI, 0.58 – 1.48) [17]. Hence the ASIR in 2008 for cancer of the kidney resembled that of Central Sub-Saha- ran Africa in 2021. In Jamaica in 2008 the ASIR for cancer of the kidney in males was 1.3 (95% CI, 0.67 – 1.93) and that of females was 0.8 (95% CI, 0.31 – 1.29). If the ASIR is used to compare both genders, the following would result, (male/female ratio, 1.63). The CIR was used to determine the parish where an individual is likely to develop cancer of the kidney in 2008. Kingston and St. Andrew were treated as one as they are so interwoven. Table 5 shows the results. The highest probability of developing cancer of the kidney was Kingston and St. Andrew (2.0), then St. Catherine (1.2), St. Thomas (1.1), Manchester (1.1), St. Mary (0.9), St. Elizabeth (0.7) and St. Ann (0.6). Table 6 is a frequency table which shows that the highest frequency of cancer of the penis in 2008 occurred in the age group 50 years to 64 years. Table 6 also shows that onset of penile cancer occurred in the 20 years to 24 years in 2008. The mean age at which penile cancer was diagnosed was (55.92 ± 4.69) years in Jamaica 2008. Sousa et al. determined that the mean age at which penile cancer was diagnosed in Brazil was (66 ± 17.10) years [18]. Akers and Holden stated that penile cancer is primarily a disease of the elderly [19]. The main risk factors for develop- ing penile cancer are phimosis, chronic inflammation of the glans penis and foreskin, ultraviolet A phototherapy, phototherapy with the use of psolarenes, smoking, human papillomavirus infection, low socioeconomic status, early age of sexual initiation and high number of sexual partners [20-28]. Larke et al. stated that men cir- cumcised in childhood or adolescence are at substantially reduced risk of developing penile cancer [26]. In 2008 the CIR of penile cancer in Jamaica was 0.9 and the ASIR was 1.5 (95% CI, 0.95 – 2.05). However, in 2020 the ASIR for penile cancer worldwide was estimated to be 0.8 per 100000 men [29].
Hence in 2008 the ASIR of penile cancer in Jamaica was almost twice that of the world in 2020. The CIR was also used to determine the probability of developing penile cancer in the various parishes in Jamaica. This is illustrated in table 7. The highest probability of developing cancer of the penis was in Kingston and St. Andrew (2.2), then St. Catherine (1.2), Manchester (1.0) and Clarendon (0.8).
Limitations
In 2008 and earlier there were two major cancer treatment centers in Jamaica for the public. These were Kingston Public hospital in Kingston and Cornwall Regional hospital in St. James. The machines they had at that time were cobalt machines. Hence many cases would be referred to Kingston Public hospital from other parishes or to Cornwall Regional hospital. This would depend on the proximity and the accessibility, meaning the length of the waiting list. Staff at the Jamaica Cancer Registry only gets data from hospitals and private sources in Kingston and St. Andrew Jamaica. Hence some patients from the western end of the island such as the parishes of St. James, Westmoreland, Trelawny and Hanover would not be recorded based upon the present practice. Hence these would contribute to errors in the data from parishes in those regions of the island. In Kingston at that period there was the Radiation Oncology Centre of Jamaica which was established in 2001. This is a private center for the treatment of cancer. Hence the limitation here would be your socioeconomic status. There would also be persons who would seek alternative ways to treat their cancer.
Conclusion
In mitigating cancer of the kidney and cancer of the penis, the public should be educated regarding the potential risk factors. In the case of cancer of the kidney these include advancing age, male gender, smoking, hypertension, obesity, ethnicity and exposure to trichloroethylene. When cancer of the penis is considered the risk factors include phimosis, chronic inflammation of the glans penis and foreskin, ultraviolet A phototherapy, smoking, human papil- lomavirus infection, early age of sexual initiation, high number of sexual partners etc. Circumcision in childhood or adolescent should be promoted as it can drastically reduce the risk of penile cancer. Screening of these cancers should be facilitated by various health administrators and various regions (parishes) targeted since this will reduce the financial burden associated with these cancers.
Data Availability Statement
Due to ethical concerns, supporting data cannot be made openly available. Further information about the data and conditions for access are available from Mrs. Dawn McNaughton, Registrar, Jamaica Cancer Registry, Pathology Department, University Hospital of the West Indies, Mona.
Ethical Approval
Ethical approval was not requested because data was treated anonymously. This was based on section 37 of the Jamaica Data Protection Act 2020. In this context, Laten Andre Mclish is the data processor (researcher) and the Jamaica Cancer Registry located in the Pathology department of the University hospital of the West Indies is the data controller.
Acknowledgement
I wish to express posthumous thanks to Professor Barrie Hanchard who provided access to the Jamaica Cancer Registry located in the Pathology Department of the University Hospital of the West Indies.
Synopsis
This study investigated the distribution of cancer of the kidney and cancer of the penis in Jamaica in 2008.
References
- Gibson, T. N., Blake, G., Hanchard, B., Waugh, N., & McNaughton, D. (2008). Age-specific incidence of cancer in Kingston and St Andrew, Jamaica, 1998–2002. West Indian Med J, 57(2), 81-89.
- Gibson TN, Hanchard B, McNaughton D. Age – Specific Incidence of Cancer in Kingston and St. Andrew, Jamaica, 2003 – 2007. West Indian Med J 2010; 59(5): 456 – 64.
- https://www.my-island-jamaica.com/jamaica_parishes.html
- Bras G. Cancer incidence in Jamaica, Kingston and St.Andrew 1958 – 1963. In: Doll R, Payne P, Waterhouse J, eds. Cancer incidence in five Continents, Vol 1 Berlin: Springer Verlag; 1966: 84 – 9.
- Brooks, S. E., & Wolff, C. (1991). Age-specific incidence of cancer in Kingston and St. Andrew, Jamaica. Part I: 1978- 1982. The West Indian Medical Journal, 40(3), 127-128.
- Jensen, O. M. (Ed.). (1991). Cancer registration: principles and methods (Vol. 95). IARC.
- The International Statistical Classification of Diseases andRelated Health Problems (ICD – 10), 10th edition.
- Statistical Institute of Jamaica http://statinja.gov.jm/Census/PopCensus/Populationbyfiveyearsagegroups.aspx
- Boyle, P., & Parkin, D. M. (1991). Statistical methods for registries. Cancer registration: principles and methods, 95, 126-158.
- National Cancer Institute Surveillance, Epidemiology and End Results (SEER) Program https://www.seer.cancer.gov/ stdpopulations/world.who.html
- Stewart, B., & Wild, C. P. (Eds.). (2014). World cancer report. Lyon, France. IARC Press.
- Rossi, S. H., Klatte, T., Usher-Smith, J., & Stewart, G. D. (2018). Epidemiology and screening for renal cancer. World journal of urology, 36(9), 1341-1353.
- Bahadoram, S., Davoodi, M., Hassanzadeh, S., Bahadoram, M., Barahman, M., & Mafakher, L. (2022). Renal cell carcinoma: an overview of the epidemiology, diagnosis and treatment. Giornale Italianodi Nefrologia, 3, 1 – 16.
- Gansler, T., Fedewa, S., Amin, M. B., Lin, C. C., & Jemal,(2018). Trends in reporting histological subtyping of renal cell carcinoma: association with cancer type. Hum Pathol, 74, 99 – 108.
- Kim, C. S., Han, K-D., Choi, H. S., Bae, E. H., Ma, S. K.,& Kim, S. W. (2020). Association of hypertension and blood pressure with kidney cancer risk: a nationwide population- based cohort study. Hypertension, 75(6), 1439 -1446.
- Johansson, M., Carreras-Torres, R., & Scelo, G., et al. (2019). The influence of obesity- related factors in the etiology of renal cell carcinoma-A mendelian randomized study. PLoS medicine, 16(1), e_1002724.
- Hao, Z., Meng-Yang, L., Li-Sha, L., Qiao, H., Peng-Cheng,L., Hang-Hang, L., Jiao, H., Dan-Qi, W., Yong-Bo, W., Yuan-Yuan, Z., Ren-Peng, Y., Yi-Tong, L., Hang, Z., Tong-Zu, L., Yu, F., & Xian-Tao, Z. (2024). Global burden of benignprostate hyperplasia, urinary tract infections, urolithiasis, bladder cancer, kidney cancer and prostate cancer from 1990 to 2021. Military Medical Research, 11(64), 1 – 18.
- de Sousa, I. D. B., Vidal, F. C. B., Branco Vidal, J. P. C., de Mello G. C. F., do Desterro Soares Brandão Nascimen, M., & Brito, L. M. O. (2015). Prevalence of human papillomavirus in penile malignant tumors: viral genotyping and clinical aspects. BMC Urol, 15(1), 13.
- Akers, C., & Holden, F. (2020). An overview of the diagnoses and treatments for penile cancer. British Journal of Nursing, 29(9), S6-S14.
- Thomas, A., Necchi, A., Muneer, A., Tobias-Machado, M., Tran, A. T. H., Van Rompuy, A. S., ... & Albersen, M. (2021). Penile cancer. Nature Reviews Disease Primers, 7(1), 11.
- Christodoulidou, M., Sahdev, V., Houssein, S., & Muneer, A. (2015). Epidemiology of penile cancer. Current problems in cancer, 39(3), 126-136.
- Douglawi, A., & Masterson, T. A. (2019). Penile cancer epidemiology and risk factors: a contemporary review. Current opinion in urology, 29(2), 145-149.
- Pow-Sang, M. R., Ferreira, U., Pow-Sang, J. M., Nardi, A. C., & Destefano, V. (2010). Epidemiology and natural history of penile cancer. Urology, 76(2), S2-S6.
- Colberg, C., van der Horst, C., Jünemann, K. P., & Naumann,C. M. (2018). Epidemiology of penile cancer. Der Urologe. Ausg. A, 57(4), 408-412.
- Anderson, S., Breen, K. J., Davis, N. F., Deady, S., & Sweeney,P. (2022). Penile cancer in Ireland–a national review. the surgeon, 20(3), 187-193.
- Larke, N. L., Thomas, S. L., dos Santos Silva, I., & Weiss, H.(2011). Male circumcision and penile cancer: a systematic review and meta-analysis. Cancer causes & control, 22(8), 1097-1110.
- Ahmed, M. E., Khalil, M. I., Kamel, M. H., Karnes, R. J., & Spiess, P. E. (2021). Progress on management of penile cancer in 2020. Current treatment options in oncology, 22(1), 4
- Giona, S. (2022). The epidemiology of penile cancer. In N. Barber & A. Ali (Eds.), Urologic Cancers. Exon Publications.
- Fu, L., Tian, T., Yao, K., Chen, X. F., Luo, G., Gao, Y., ...& Zou, H. (2022). Global pattern and trends in penile cancer incidence: population-based study. JMIR public health and surveillance, 8(7), e34874.