
World Journal of Radiology and Imaging(WJRI)
ISSN: 2835-2440 | DOI: 10.33140/WJRI


Research Article - (2022) Volume 1, Issue 1
Dietary Calcium Intake and Associated Factors Among Pregnant Women in Loma District, South West Ethiopia, 2020
2School of Public Health, College of Medicine and Health Sciences, Wolaita Sodo University, Ethiopia
3School of Public Health, College of Medicine and Health Sciences, Wolaita Sodo University, Ethiopia
Received Date: Aug 04, 2022 / Accepted Date: Sep 25, 2022 / Published Date: Nov 01, 2022
Copyright: ©Copyright: Ã?©2022 Adisu Hailu, Coordinator. This is an openaccess article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Hailu, A. (2022). Dietary Calcium Intake And Associated Factors Among Pregnant Women In Loma District, South West Ethiopia, 2020. World J Radiolo Img 1(1), 28-37.
Abstract
Background: Low dietary calcium intakes could cause harmful effects to the pregnant woman by influencing pregnancy outcome. Adequate intake of dietary calcium during pregnancy reduces the risk of complications and aids in improved birth outcome. Many researchers focus on urban areas to address the issue and our study was focused on rural community. Hence the study is aimed at assessing dietary calcium intake in rural communities.
Objective: To assess the dietary calcium intakes and associated factors among pregnant women in Loma, south west Ethiopia from May to July, 2019
Methods: -A community based cross-sectional study was conducted in Loma district, Dawuro zone, southwest Ethiopia. Data were collected from 398 pregnant women after random selection from nine kebeles. Simple random sampling technique was employed to select study subjects. Socio-economic and demographic, and health related data was collected using structured, interviewer administered, and pre tested questionnaire. The 24 hr dietary recall was used for three different days with seven days interval as per the recommendation. When dietary data is collected, often it was converted into nutrients, especially the calcium intake by using Ethiopian food composition table. Collected data was checked for completeness, and entered in to Epi Data version 3.02 for data clearance and exported to SPSS version 20 for analysis. AOR with 95% C.I results of multivariate logistic regression was used to assess the statistical significance of associations between independent and dependent variables. The level of statistical significance was declared at p <0.05.
Result: The median calcium intake was 543mg per day. From 398 participants, 265(66.6%) were at risk of inadequate intake of calcium. Greater than half 249 (62.6%) respondents had practiced avoiding calcium rich food during their pregnancy. The finding of this study identified that nutritional counseling have strong statistical association with dietary calcium intake of mothers during pregnancy. The chance of dietary calcium intakes during pregnancy who were received nutritional counseling 2.4 times higher than those who were not received nutritional counseling (AOR=2.432 95% CI: 1.072-5.517).
Conclusion and recommendation: From the present study, it can be concluded that, majority of pregnant mothers 265(66.6%) had a poor dietary calcium intakes during their pregnancy. It is recommended that consumption of enough calcium and dairy products should be included and emphasized in the nutrition education component of maternal health programs.
Keywords
Dietary Calcium Intake, Pregnant Women, Loma District.
Introduction
Inadequate intakes of calcium are one of the most serious public health problem affecting mothers and their children in the world. WHO estimates that at least one woman dies every seven min- utes from complications of hypertensive disorders of pregnancy this is may be because of low intakes of dietary calcium [1]. Inadequate intakes of calcium during pregnancy cause hyperten- sive disorder which is a major health problem leading maternal and perinatal morbidity and mortality. However, an adequate calcium intake during pregnancy might prevent pregnancy in- duced hypertension, preterm birth, FGR, increasing maternal bone mass, and reduce fracture risks [2-3].
In resource-poor environments across the globe, low quality monotonous diets are the norm. When grain- or tuber-based staple foods dominate and diets lack vegetables, fruits and ani- mal-source foods, risk for a range of micronutrient (calcium) de- ficiencies is high. Mainly pregnant women is vulnerable group , but there is no sufficient information on micronutrient (calcium) deficiencies on such global public health problem among preg- nant women [4].
There is less evidence from developing countries generally and specifically where monotonous diets, relying mostly on a typical few plant-based staple foods confirm this association specifical- ly among pregnant women [5]. Maternal diets during pregnan- cy need to provide nutrients for the mother as well as for fetal growth and development. Prevention of Hypertensive disorders and preeclampsia are the advantages of dietary calcium intakes during pregnancy[6].Ensuring that appropriate dietary calcium is consumed is important for preventing pregnancy induced hy- pertension and helping to reduce the risk of osteoporosis with advancing age [7-8]. So evaluation of dietary calcium intake and associated factors among pregnant women in Loma Woreda, Dawuro, South West Ethiopia is very important.
Materials and Methods
Study Settings and study period
The study was conducted in Loma Woreda from May to July 2019 which is located 512 km away from Addis Ababa, the cap- ital city of Ethiopia, 292 km from Hawassa, the regional town SNNPR. The district structured in to 24 rural and 3 urban kebe- les. According to the report of CSA the estimated population of Loma Woreda was 108,965 out of which 53,502 were male & 55,463were female[9]. Maize, enset (false banana), and root crops are majorly consumed food items [10].
Study Design: Community based cross sectional study design was used.
Source Population: All pregnant women who are living at least for six months in Loma Woreda
Study Population: Randomly selected pregnant women were participated during the study period.
Inclusion criteria: - Pregnant women who are living at least for 6 months in Loma Woreda.
Exclusion criteria: Seriously ill pregnant women during the in- terview were not considered in study.
Sample size determination
The sample size was determined by using single proportion for- mula by taking assumptions of the prevalence of dietary calcium intake as 50% , 5% marginal error, 95% CI, a non-response rate of 10%. Therefore, sample size is: n= (zα/2)2 p (1-p)/d2 = (P = 50%) (1.96)2*0.5(1-0.5)/ (0.05)2n = 384 When adding 10% none response rate, the maximum sample size were (384*10%) = 422.
Sampling procedures
From the total of 27 kebeles of Loma Woreda, 9 kebeles was selected by simple random sampling method. A sample frame from selected kebeles was taken from kebele health posts. Sam- ple size for each selected kebeles was allocated proportionally. Study participants were selected by using simple random sam- pling technique. List of participating households from the se- lected kebeles was obtained from HEW. After obtaining a list of participant households, we have selected the required sam- ple size by using lottery methods. A pregnant woman in each 9 kebeles and the first household was selected by simple random sampling method.

Figure 1: Schematic presentation of sampling procedure for the dietary calcium intakes and associated factors among pregnant women in Loma Woreda.
Operational definitions
Above RDA: The amount calcium intake is above1000 mg per day.
Below RDA: The amount of calcium intake is less than 1000 mg per day.
Adequate Intake: The amount of calcium intake is equals to 1000 mg per day.
Positive Attitude: Pregnant women’s score is ≥ the mean score 25 in likert scale
Negative Attitude: Pregnant women’s score is< 25 in likert scale.
Adequate Knowledge: Pregnant women score is ≥ the average score 7 Poor knowledge: Pregnant women score is < average score 7
Data collection tool and procedure
Recruitment of data collectors
Eight diploma nurses were recruited to collect the data and one BSC nurse and one Health officer were supervising data collec- tion. The data collector and supervisor were trained for two con- secutive days on the objective, ethics, method and contents of question.
Quantified multiple pass 24 hr. Recall
The 24 hour dietary recall includes the type of food and bever- ages consumed inside and outside of the house along with the quantity of the foods. The 24-hour period starts with the first food eaten by the pregnant women in the morning until the last food item consumed before going to bed. The Quantified 24 hr recall was used for at least three different days which covers at least one week day and one weekend day so as to adequately represent the habitual intake .The FAO (2018) Quick guide to use 24 hr recall was followed.
Dietary Recall: Each interview involved, a stepwise series of questions, normal household utensils, food substitutes (play dough, flour, lentils, water) and pictures of most commonly con- sumed foods in the specific regions to improve the memory of the respondents and assist in completing the questionnaires. 24hr dietary recall was conducted using the multiple-pass tech- nique which include,
First pass:-Quick list of all foods, drinks, snacks consumed from midnight of one day until midnight the following day.
Second pass:-Detailed and more specific descriptions of all the foods and drinks consumed, including cooking methods and brand names (where possible). The interviewer also asked if the respondent has remembered any additional items that were con- sumed but which were forgotten in the first pass.
Third pass:-Estimating portion sizes
In order to accurately estimate the portion size of foods and drinks consumed, Calibrated locally available labeled cup, bowl, spoon, serving spoons, food weighing scale. Moreover, the data collectors carried different sizes of locally consumed fruits and vegetables such as bananas, avocado, shallot, tomato, potato, yum to facilitate the recall [21].
Pass four:-The interviewer reviewed the recall to ensure that all the items have been recorded correctly. Every respondent were probed for snacks, drinks and outdoor consumption of any kind of food after they complete recall. The interviews were conducted on all seven days of the week to capture changes in intakes across various days of the week. The dietary recall was repeated in randomly selected of the house- holds by interviewer and in a different nonconsecutive day than the first. The recall was repeated to adjust for the day to day variation we were include week day and weekends and to adjust within person variation of nutrient intakes of the study partici- pants we were increased days. All recall days were arranged on non-special occasion days like holidays or feasts.
The calcium intake was calculated by using food composition table of Ethiopia[22]. After calculating the intake of dietary Cal- cium per day the values was compared with WHO Recommend- ed Dietary Allowances of Calcium for pregnant women as there is a lack of national standards.
The standard Questionnaire
Data was collected by using structured questionnaire which is adopted after reviewing literatures of similar studies based on the objective of this study. An interactive, multiple-pass 24hr di- etary recall questionnaire adapted and validated for use in devel- oping countries [30] was used to collect data on dietary intake. The knowledge and attitude of pregnant was categorized on two and five-level which includes the responses for given negative and positive statement as correct and incorrect and strongly dis- agree, disagree, neither agree nor disagree ,strongly agree, agree and (1,2,3,4,5) of likert scale. Data quality assurance Before data collection, the study questionnaire was checked us- ing a pretest of 5% of invited pregnant women from households. Before estimating portion size we were standardizes measuring tools, and we were observed locally available measuring tools in study area then measure the common foods from 10(ten) house- hold by digital food scale used to measure the gram amount of food consumed and of ingredients used in food preparation and finally took the average amount. Drinking cups glasses, spoons and ladles were labeled in to three categories based on their size (large, medium and small).
The questionnaire was prepared initially in English and then translated into Amharic Language, then retranslated back to English by another person who has good command of English, Amharic language to check for its consistency. The data collec- tors and supervisors were trained two days particularly in the proper filling of multiple pass 24 hour recalls. Information on 24-hour recall is collected using an open-ended format. Quan- titative information on food intake, as described using portion size, allows for the calculation of calcium intakes of a 24-hour recall form. Estimation of portion size is facilitated by the use of measurement aids such as standard household measurement tools [11]. To calculate calcium intakes, the estimated portion size or the amount of food intake was multiplied by the values of nutrient content in foods as found in the Ethiopian food com- position tables[22].
Data management and analysis plan
Data was checked for completeness and consistency, edited manually, coded and then entered in to Epi Data version 3.02 for data clearance and exported into SPSS version 20 for analysis. Descriptive statistics was used to calculate frequencies and per- centages of study participants with regard to different variables. Variables with a p-value less than 0.25 in the bi variable logistic regression analysis were candidate for multivariable analysis. AOR with 95% C.I. of p<0.05 in multivariable logistic regres- sion was considered as statistically significant.
Ethical clearance was obtained from Ethical Review Committee (ERC) of Wolaita Sodo University, department of Human Nutri- tion and support letter was to Loma Woreda Health office.
Results
Socio-demographic and Economic Characteristics of Participants
Three hundred and ninety eight (398) subjects were participat- ed in the study with response rate of 94%. The median age of study subjects was 30 years. Concerning educational level, 176 (44.2%) of the respondents were illiterate and 365(91.7%) of pregnant women’s earned less than 1000 ETB per month month- ly income. Two hundred twenty seven (57%) of the respondents had nutritional information during their pregnancy.
Table 1: Socio-demographic and economic factors among pregnant women in Loma woreda, south west, Ethiopia (n= 398)
|
Characteristics |
Numbers (%) |
|
Age group of subject |
|
|
15-24 |
56(14.1) |
|
25-34 |
254(63.8) |
|
35-44 |
88(22.1) |
|
Monthly income in ETB |
|
|
<1000ETB |
365(91.7) |
|
1000-2000ETB |
17(4.3) |
|
>2000ETB |
16(4) |
|
Marital Status |
|
|
Married |
357(89.7) |
|
Single |
2(0.5) |
|
Divorced |
11(2.8) |
|
Widowed |
28(2) |
|
Occupational status |
|
|
Farmer |
87(21.9) |
|
Housewife |
281(70.6) |
|
Civil servant |
22(5.5) |
|
Merchants |
8(2.2) |
|
Household size |
|
|
<4 |
191(48) |
|
>=4 |
207(52) |
|
Education |
|
|
Illiterate |
176(44.2) |
|
Primary |
106(26.6) |
|
Secondary & above |
116(29.2) |
|
Market Availability |
|
|
Yes |
118(29.6) |
|
No |
280(70.4) |
Calcium Intakes
Out of 398 study participants responded for the questions to assess their dietary calcium intakes, 66.6% of them had inad- equate calcium intakes in which, greater than half 249 (62.6%) respondents had practiced avoiding calcium rich food during their pregnancy. Out of those who avoided food during their pregnancy, due to it makes the baby big, culture and it makes delivery difficult. About 44.7% pregnant women of this study were agreed on satisfactory birth out comes can be achieved through nutrition knowledge and practice of pregnant women. The median intake was 543 mg/day. The Proportion of pregnant women with low calcium intakes (less than 1000 mg per day) was 265(66.6%).

Figure 2: Distribution of dietary calcium intakes among pregnant women in Loma woreda, South west Ethiopia, 2019 (n=398).
Meal consumption pattern of pregnant women
Three hundred eighty three (96.2%) of the respondents had not practiced the habit of eating snacks between meals during their pregnancy. Majority of the pregnant mothers do not consume their snacks.
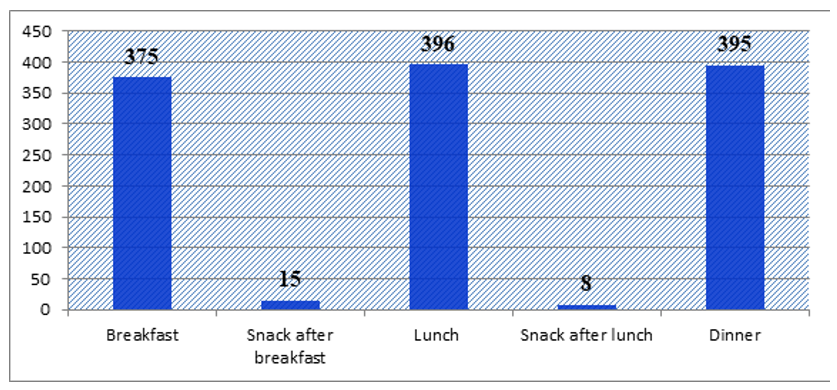
Figure 3: Meal pattern of pregnant women of Loma, south west Ethiopia, 2019(n=398)
Group of Foods consumed by pregnant women
Plant based foods such as cereal, roots and tubers and also green leafy vegetables were the most consumed. Flesh foods and milk products were the least consumed food groups.
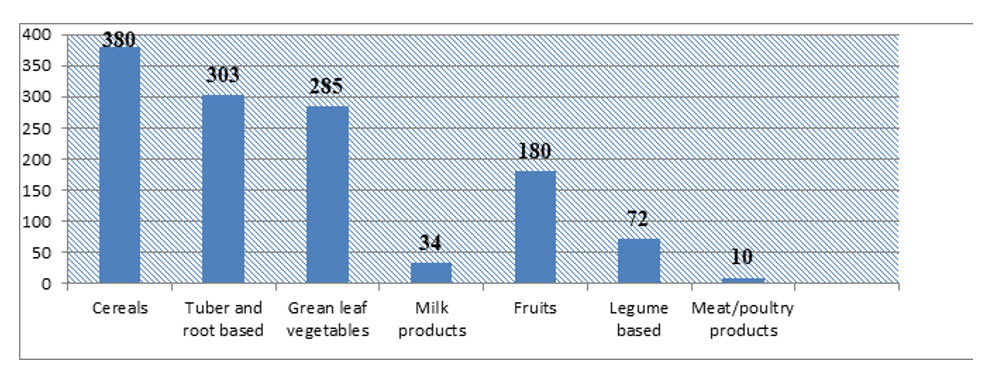
Figure 4: Proportion of food group consumed by pregnant women of Loma district, south west Ethiopia, 2019(n=398)
Dietary Diversity Score of pregnant women
Out of 398 study participants responded for the questions to assess their dietary diversity, 241(61%) of them had inadequate dietary diversities. Different evidence showed that in developed countries, dietary diversity is strongly associated with nutrient adequacy [20].
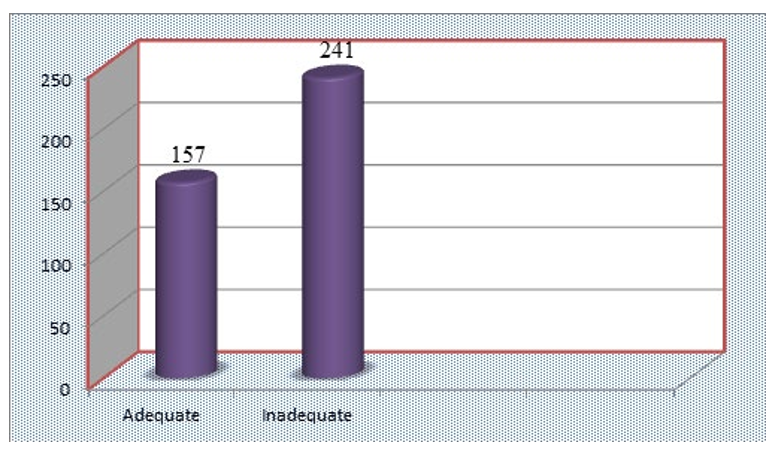
Figure 5: Dietary diversity score of pregnant women of Loma district, southwest Ethiopia, 2019 (n=398)
Factors associated with calcium intake
Age, level of education, distance from health facility, occupa- tion, household size, nutritional counseling, regular milk con- sumption, importance of calcium, culture and facility visit were the factors associated with dietary intake of calcium.
Multivariate analysis showed that there was statistically signifi- cant association between occupation and dietary calcium intakes of mothers during pregnancy. Women who were being civil ser- vant (AOR 0.052 95% CI 0.01 - 0.269) were less likely to have calcium intakes than farmers. The chance of dietary calcium intakes during pregnancy among mothers who were received nutritional counseling 2 times more likely than those who were not received nutritional counseling(AOR=2.432 95% CI: 1.072- 5.517).
Relative to the pregnant women who were agreed on calcium importance had significantly 3 times more likely to had good di- etary calcium intakes during their pregnancy (AOR=3.256, 95% CI;1.241-8.547) than women who were not agreed on calcium importance.
Table 2: Dietary calcium intake and socio-demographic characteristics in pregnant women in Loma woreda southern Ethi- opia 2019 (Bivariate analysis)
|
Calcium intakes |
|||||
|
|
< Median value |
>= Median value |
p-value |
||
|
Variables |
N |
% |
N |
% |
|
|
Age |
|||||
|
15-24 |
29 |
7 |
27 |
7 |
0.023 |
|
25-34 |
125 |
31 |
129 |
32 |
|
|
35-44 |
47 |
12 |
41 |
10 |
|
|
Education |
|||||
|
No education |
94 |
24 |
82 |
21 |
<0.001 |
|
Primary |
67 |
17 |
39 |
10 |
|
|
Secondary and above |
40 |
10 |
76 |
19 |
|
|
Distance from health facility |
|||||
|
<=10km |
94 |
24 |
112 |
28 |
0.001 |
|
>=11km |
107 |
27 |
85 |
21 |
|
|
Visit to PHCU |
|||||
|
Yes |
106 |
27 |
163 |
41 |
0.001 |
|
No |
95 |
24 |
34 |
8 |
|
|
Nutritional counseling received |
|||||
|
Yes |
78 |
20 |
149 |
37 |
<0.001 |
|
No |
123 |
31 |
48 |
12 |
|
|
Regular consumption of milk and milk products is good for pregnant women |
|||||
|
Agree |
46 |
12 |
119 |
30 |
<0.001 |
|
Disagree |
155 |
39 |
78 |
19 |
|
|
Regular intake of green leafy vegetables is good for pregnant women |
|||||
|
Agree |
74 |
18 |
127 |
32 |
<0.001 |
|
Disagree |
127 |
32 |
70 |
18 |
|
|
Satisfactory birth out comes can be achieved through nutrition knowledge and practice |
|||||
|
Agree |
54 |
13 |
124 |
31 |
<0.001 |
|
Disagree |
147 |
37 |
73 |
18 |
|
|
Calcium is important for the pregnant women and growing fetus |
|||||
|
Agree |
28 |
7 |
83 |
21 |
<0.001 |
|
Disagree |
173 |
43 |
114 |
29 |
|
|
My culture encourages me to take milk and dairy products, green leafy vegetables during pregnancy. |
|||||
|
Agree |
64 |
16 |
85 |
21 |
0.014 |
|
Disagree |
137 |
34 |
112 |
28 |
|
|
Awareness on recommended dietary intake during pregnancy reached rural areas. |
|||||
|
Agree |
137 |
34 |
104 |
27 |
<0.001 |
|
Disagree |
64 |
16 |
93 |
23 |
|
|
Dietary calcium intakes during pregnancy is bad |
|||||
|
Agree |
168 |
42 |
118 |
30 |
<0.001 |
|
Disagree |
33 |
8 |
79 |
20 |
|
|
Kind of services |
|||||
|
No visit |
95 |
24 |
34 |
9 |
<0.001 |
|
ANC visit |
95 |
24 |
148 |
36 |
|
|
Other visit |
11 |
3 |
15 |
4 |
|
|
Family size |
|||||
|
<4 |
90 |
23 |
101 |
25 |
0.083 |
|
>=4 |
111 |
28 |
96 |
24 |
|
|
Knowledge on dietary calcium intakes |
|||||
|
Adequate |
101 |
25 |
69 |
17 |
0.036 |
|
Poor |
100 |
25 |
128 |
33 |
|
|
Attitude towards dietary calcium intakes |
|||||
|
Positive attitude |
103 |
26 |
75 |
19 |
0.043 |
|
Negative Attitude |
98 |
25 |
122 |
30 |
|
|
Dietary diversity score |
|
|
|
|
|
|
Adequate |
61 |
15 |
96 |
24 |
0.105 |
|
Inadequate |
136 |
35 |
105 |
26 |
|
|
Market Availability |
|||||
|
Yes |
70 |
18 |
48 |
12 |
0.303 |
|
No |
131 |
33 |
149 |
37 |
|
Table 3 : Dietary calcium intake and associated factors in pregnant women in Loma woreda, south west Ethiopia, 2019
(multivariate logistic regression).
|
S/no |
Variables |
N (%) |
Daily dietary calcium intake ≥ median value |
||
|
OR |
95%CI |
p-value |
|||
|
1 |
Occupation of the respondents |
||||
|
Civil servants |
22(5.5) |
1 |
1 |
|
|
|
Housewives |
281(70.4 |
0.207 |
0.066-0.654 |
0.007 |
|
|
Farmers |
87(21.8) |
0.052 |
0.01-0.269 |
0.001 |
|
|
Merchants |
8(2.3) |
0.023 |
0.002-0.279 |
0.003 |
|
|
2 |
Family size |
||||
|
>4 |
207(52.1) |
0.285 |
0.111- 0.733 |
0.009 |
|
|
<=4 |
191(47.9) |
1 |
1 |
|
|
|
3 |
Attitude towards dietary calcium intake |
||||
|
Negative atti- tude |
201(50.4) |
0.003 |
0.001-0.016 |
0.001 |
|
|
Positive atti- tude |
197(49.6) |
1 |
1 |
|
|
|
4 |
Nutritional counseling received |
||||
|
No |
171 (43.1) |
2.432 |
1.072-5.517 |
0.034 |
|
|
Yes |
227 (56.9) |
1 |
1 |
|
|
|
5 |
Calcium is important for the pregnant women and growing fetus |
||||
|
Disagree |
287(72.2) |
3.256 |
1.241-8.547 |
0.016 |
|
|
Agree |
111(27.8) |
1 |
1 |
|
|
|
6 |
Regular consumption of milk and milk products is good for pregnant women |
||||
|
Agree |
165(41.4) |
1 |
|
|
|
|
Disagree |
233(58.6) |
2.806 |
1.124-7.005 |
0.027 |
|
|
7 |
Age |
||||
|
15-24 |
56(14) |
0.876 |
0.297-2.582 |
|
|
|
25-34 |
254(63.7) |
0.126 |
0.027-0.581 |
0.008 |
|
|
35-44 |
88(22.3) |
1 |
|
|
|
In multivariate logistic regression, occupation AOR=0.052(0.01- 0.269), family size, AOR=0.285 (0.111- 0.733), attitude towards calcium intakes AOR= 0.003 (0.001-0.016), nutritional coun- seling AOR=2.432 (1.072-5.517), knowledge on calcium AOR 3.256 (1.241-8.547), regular consumption of milk AOR=2.806 (1.124-7.005) and age of respondents AOR = 0.126 (0.027- 0.581) are associated factors with dietary calcium intakes among pregnant women.
Discussion
The study was inspected the dietary calcium intakes and associ- ated factors among pregnant women. Low dietary Calcium in- take was widespread among pregnant women. Findings of this cross-sectional study indicate that a high proportion of pregnant women in study area do not consume enough calcium as well as calcium-rich food products; and meeting adequate intake of this nutrient is not possible through the current dietary patterns in the majority of the studied population. Dietary calcium intake was associated with age, occupation of respondents, family size, nutritional counseling, attitude towards dietary calcium intake and knowledge on calcium importance and regular consumption of milk.
Dietary Calcium Intake
The study presented that the average calcium intake in pregnant women in our study area was low (543mg/day) compared to WHO recommendation. This result clearly reflects the low con- sumption of calcium-rich products and culture of the communi- ty. The finding was correlated with survey conducted in china and Iran mean intakes were 633.2 ± 492.4 and 644 ± 255 respec- tively in 2015[13]. Likewise, low calcium intakes (561mg/day) were observed in Benin 2014 [14].Researcher’s also reported similar finding on the pregnant women in the study conducted in Sidama Zone, Southern Ethiopia. As it was observed with the other micronutrients, calcium intake was also lower than the rec- ommendation in both of the study groups. Its intake was much lower (below half of the requirement) during their pregnancy [15].
In differently, higher dietary calcium intakes 1,256.9 mg/day were observed in Thailand 2018[16]. Consequently to low av- erage calcium intakes, the occurrence of adequate calcium in- take in pregnant women in the current study is low. 33.4% of pregnant women have adequate calcium intake. This result is comparable in Nigeria the prevalence of calcium intake is 40% [10]. In contrast, higher prevalence of adequate calcium intake in America and Canada, and Europe, with their mean daily cal- cium intake as 1176, and 1141 mg/day respectively [6, 17].The discrepancy of the two studies may be due to the fact that the differences between the study participants, in that the present study was conducted on rural communities ( pregnant mothers) which can be lower than rural mothers in terms of educational, economic status and more access to nutrition information during pregnancy.
The different results underlined differences in dietary consump- tions. In developing country especially in our study area dietary calcium intakes among pregnant women are very low for the reason that diets are mainly on cereal and legumes based [18, 8, 19]. In addition the culture of community were prohibited to consume calcium rich food products for pregnant women mainly milk and milk products because of this food groups fattening the fetus and difficulty happen during delivery time. Whereas, in developed country, calcium intake is high due to production and usual consumption of dairy products. Definitely, consumption of calcium-rich foods is low in the study population [19].
Meaningful that hypertensive conditions and its difficulties during gestation are prevalent in developing countries and the positive role of adequate calcium intake in reducing the risk of hypertensive disorders, the common inadequate calcium intake through pregnancy in developing countries requires adequate in- terventions [7].
Factors Associated with Dietary Calcium Intake in Pregnant Women
Women who were being civil servants (AOR 0.052 95% CI 0.01-0.269) were less likely to have calcium intakes than farm- ers. This result is supported by the study conducted in Kenya in which employee was associated with dietary calcium intakes (AOR= 1.08 95% CI 0.88 - 2.45). Also in this study women’s dietary attitude had shown negative relationship with dietary calcium intake of mothers during pregnancy (AOR=0.003 95% CI 0.001-0.016). This finding is also in agreement with the study conducted in America in which the most significant predictor for good dietary practice was women’s attitude towards dietary intake of calcium (AOR=2.32, 1.56-3.43). The present study also demonstrated that there was strong statistical association between regular consumption of milk and milk products and dietary calcium intake during pregnancy (AOR=3.256 95% CI 1.241-8.547). This result is supported by the study conducted in Thailand in which consumption of milk products was signifi- cantly associated with dietary calcium intakes (3.9 95% CI: 2.0- 5.9)[16].
The finding of this study identified that nutritional counseling have strong statistical association with dietary calcium intake of mothers during pregnancy AOR=2.432 95% CI: 1.072-5.517).
This result is supported by the study conducted in Thailand in which nutrition information was the predictor factor for dietary calcium intakes in the study area (AOR= 0.985, 95% CI: 0.775 - 1.250). Pregnant women in urban areas, women with those whose household size is less than four were significantly less likely to have higher calcium intakes compared to rural wom- en, with those whose household’s size was four or less(AOR 0.285 95% CI 0.111- 0.733). This result is supported by the study conducted in Benin in which house hold size was signifi- cantly associated with dietary calcium intakes (AOR 1.330 95% CI 1.092 - 1.618)[19].
Conclusion
From the present study, it can be concluded that, majority of pregnant mothers (66.6%) had a poor dietary calcium intakes during pregnancy. They lacked the basic and the essential foods to consume vegetables, fruits, egg, milk and others which are the basic sources of most of calcium. Moreover, unhealthy dietary intake was observed among them. The current study also showed that, the most significant predicting factors for dietary calcium intakes in this study were women’s nutrition knowledge, regu- lar consumption of milk, importance of calcium, age and family size. Study results show that dietary calcium intakes of pregnant women in the study area were not adequate. The results suggest that pregnant women need nutrition counseling regarding calci- um rich food intake practices during pregnancy.
List Of Abbreviations
AI = Adequate Intake
AOR=Adjusted Odd Ratio
Ca = Calcium
COR= Crude Odd Ratio
CSA=Central Statics Agency
FAO= Food and Agriculture Organization
FNB=Food and Nutrition Book
RDA= Recommended Daily Allowance
SNNPR= Southern Nation Nationalities Peoples Region
WHO= World Health Organization
Declaration
By my signature below, I declare and confirm that this manu- script of research is our work. We have followed all ethical prin- ciples of research in the preparation, data collection, processing, analysis and completion of this thesis. All scholar materials that are included have been given recognition through citation. We affirm that we have cited and referenced all sources used in this document. Every serious effort has been made to avoid any pla- giarism in the preparation of this manuscript. I really declare that this thesis is not submitted to any other institution anywhere for the publication.
Consent form
I Adisu Hailu Tofu give my consent for information about myself/my relative to be published in Nutrition & Metabolism of BMC with manuscript ID- number - NUAM-D-20-00426,co- authors - Yibeltal Kassa and Damene Darota, I understand that the information will be published without my /my relative’s as the name attached, but that full anonymity cannot be guaranteed.
I understand that the text and any pictures or videos published in the article will be freely available on the internet and may be seen by the general public. The pictures, videos and text may also appear on other websites or in print, may be translated into other languages or used for commercial purposes. I have been offered the opportunity to read the manuscript.
Competing interets
The authors declare that they have no competing interest.
Acknowledgement
We would like to acknowledge Wolaita Sodo University; Col- lege of Medicine and Health Science for the approval of the ethical clearance. Our gratitude goes high school leaders, data collectors and students who participated in this study.
Data Availability
Data are available with the corresponding author in SPSS based.
Ethical concerns
Ethical clearance was taken from Ethical Review Committee of College of Medicine and health sciences of Wolaita Sodo Uni- versity. Furthermore, letter of permission was obtained from Dawuro zone Health department. Consent was obtained from the study subjects whose age was 15 and above years after they were informed about objectives and procedures of the study and their right to refuse participation any time they want shall as- sured. No data will be shared to anyone to secure confidentiality.
References
- Tranquilli AL, D.G., Magee L, Roberts J, Sibai BM, Steyn W, Zeeman GG, Brown MA, The classification, diagnosis and management of the hypertensive disorders of pregnan- cy. A revised statement from the ISSHP, 2014. 4: p. 97-104
- Agriculture, U.S.D.o., Survey of Food Intakes by Individu- als and Diet and Health Knowledge Survey. USDA’s 2009:p. 3
- Tesfaye A G, T.B.L., Sena B K, Pregnancy Induced Hyper- tension and Associated Factors among Pregnant Women Receiving Antenatal Care Service at Jimma Town Public Health Facilities, South West Ethiopia. J Gynecol Women’s Health, 2018. 10(3).4. Gynecologists, A.C.o.O.a., Hyper- tension in Pregnancy. Report of the ACOG 2013.
- Lee SE, T.S., Merialdi M, Caulfield LE Dietary intakes of women during pregnancy in low- and middle-income coun- tries. Public Health Nutr, 2012. 16(18): p. 14.
- Bolland MJ, L.W., Tai V, et al, Calcium intake and risk of fracture. systematic review. BMJ., 2015. 351(h4580).
- Reid IR, B.S., Bolland MJ, Calcium supplements: benefits and risks. J Intern Med, 2015. 278(4): p. 354–368.
- Sukchan, P., Liabsuetrakul, T., Chongsuvivatwong, V., Songwathana, P., Sornsrivichai, V. and Kuning, M., In- adequacy of Nutrients Intake among Pregnant Women in the Deep South of Thailand. BMC Public Health, 2010. 10(572): p. 1471-2458.
- Agency, E.C.S., Federal Democratic Republic of Ethiopia Central Statistical Agency Population Projection of Ethio- pia for All Regions At Wereda Level. 2014-2017.
- Profile, L.W.H.O.P., 2019.
- FAO, Dietary Assessment: A resource guide to method selection and application in low resource settings. Rome. 2018.
- (EHNRI), E.H.a.N.R.U., Food
- Liu FL, Z.Y., Parés GV, Reidy KC, Zhao WZ, Zhao A, Chen C, Ning CY, Zheng YD, Wang PY., Nutrient Intakes of Pregnant Women and their Associated Factors in Eight Cities of China. Chin Med J 2015(128): p. 9.
- Kumar, A., Devi, S.G., Batra, S., Singh, C. and Shuk- la, D.K. , Calcium Supplementation for the Prevention of Pre-Eclampsia. International Journal of Gynaecology and Obstetrics, 2009. 104:p. 4.
- Yewelsew.Y, A.B., KMichael.H, Inadequate intake of di- etary Zinc and calcium among pregnant women from sub- ssistence householda in Sidamo, southern Ethiopia. Public Health Nutrition, 2007. 11(4): p. 8.
- Chotboon, C., Soontrapa, S., Buppasiri, P., Muktabhant, B., Kongwattanakul, K., & Thinkhamrop, J, Adequacy of cal- cium intake during pregnancy in a tertiary care center in Thiland. International journal of women’s health, 2018. 10:p. 5..
- Ariyo, O.O., Omolola. et al, Adequacy of nutrients intakes among pregnant Women in Ibadan, Nigeria. Journal of Ap- plied and Environmental Sciences, 2010. 6: p. 4.
- organization, W.h., Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D and Fluoride. National Academy Press, Washington, DC, 2009.
- WHO World Health Organization, G., World Health Report micronutrient 2010.
- Martin-Prevel Y, A.M., Allemand P, Wiesmann D, Ballard TJ, Deitchler M, et al., Development of a dichotomous indi- cator for population-level assessment of the dietary diversi- ty of women of reproductive age. 2017
- Composition Table for use in Ethiopia. Part IV. EHNRI/ Food Agriculture Organization, 1995-1997.
- Gibson RSF, E.L., An interactive 24-hour recall for assess- ing the adequacy of iron and zinc intakes in developing countries. HarvestPlus, 2008.
- (EHNRI), E.H.a.N.R.U., Food