
Advancements in Journal of Urology and Nephrology(AJUN)
ISSN: 2689-8616 | DOI: 10.33140/AJUN
Impact Factor: 1.0



Research Article - (2026) Volume 8, Issue 1
Comparative Analysis of Chronic Kidney Disease Diagnosis and Management in Spain and Portugal: A Cross-Sectional Survey of Healthcare Professionals
2Centro de Investigación Biomédica en Red para Bio-engeniería, Biomateriales y Nanomedicina, Instituto de Salud Carlos III, Spain
Received Date: Apr 20, 2026 / Accepted Date: May 27, 2026 / Published Date: Jun 01, 2026
Copyright: ©2026 Abel Mata-Lima, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Mata-Lima, A., Serrano-Olmedo, J. J. (2026). Comparative Analysis of Chronic Kidney Disease Diagnosis and Management in Spain and Portugal: A Cross-Sectional Survey of Healthcare Professionals. Adv J Uro Nephro, 8(1),01-05.
Abstract
Background: Chronic Kidney Disease (CKD) is a major global health burden, frequently underdiagnosed in early stages. Differences in healthcare systems may influence diagnostic and management pathways. This study compares CKD practices between Spain and Portugal.
Methods: A cross-sectional survey was conducted among primary care physicians and nephrology professionals in Spain and Portugal. Qualitative responses were analyzed thematically and complemented with descriptive statistics.
Results: Both countries reported substantial barriers to early CKD diagnosis. Training gaps were reported by 70% of respondents in Spain and 75% in Portugal, while communication barriers affected 65% and 70%, respectively. Late referral patterns were common in both settings. Portugal showed consistently higher perceived barriers across all domains.
Conclusions: CKD management challenges are shared across both countries but appear more pronounced in Portugal. Strengthening primary care training, improving digital integration, and implementing early detection strategies are critical to improving outcomes.
Keywords
Chronic Kidney Disease, Primary Care, Nephrology, Early Diagnosis, Health Systems, Spain; Portugal, Digital Health
Introduction
Chronic Kidney Disease (CKD) affects approximately 10–15% of the adult population worldwide and is associated with increased cardiovascular morbidity and mortality [1-3]. Early diagnosis and intervention are critical to slowing disease progression; however, CKD remains underdiagnosed, particularly in primary care settings [4-6].
Southern European countries, including Spain and Portugal, share similar healthcare models but differ in organization and resource allocation. Portugal has one of the highest rates of end-stage renal disease (ESRD) in Europe, suggesting potential inefficiencies in early detection and management [7-9].
CKD is a very important public health problem directly related to climate change and causing serious burden to the sustainability of environment and health system as well [10].
The most common renal replacement therapy (RRT), hemodialysis (HD) and peritoneal dialysis (PD) practices generate a considerable environmental footprint, and kidney health is particularly sensible to the effects of climate change [9-10].
Due to the way that the human increases the demand for food, fresh water, carburant, industry, and so forth during the last 50 years the world is facing a large and irreversible loss of diversity of ecosystem on the earth. There is the need to adopt a sustainable process in Renal Care based on CKD prevention and sustainable RRT [11-13].
The focus of this article is to collect and analyze the opinion of health care professionals (HCP) about measures that can be taken to implement effective CKD prevention. This study aims to provide a comparative analysis of CKD diagnosis and management practices between Spain and Portugal, identifying shared and country-specific barriers.
Materials and Methods
Between June and December 2024, we performed an online survey to collect the sensibility of primary care clinicians, renal nurses and nephrologists, concerning the major current challenges in kidney patients care: CKD prevention and Environmental sustainability practices.
The questionnaires were regarding key areas of CKD prevention and environmental sustainability practices during the dialysis processes, considering the CKD screening, the management of patients at risk, recommendations from kidney disease: improving global outcomes (KIDGO) and European Kidney Health Alliance (EKTA) about CKD prevention, the adoption of measures to reduce Carbon footprint, water usage, energy efficiency and consumption, waste management and recycling program.
Study Design
A cross-sectional survey was conducted among healthcare professionals, including:
• Primary care physicians
• Nephrologists
• Renal nurses
Ethical Considerations
The study was approved by the Ethics Committee of the Universidad Politécnica de Madrid, ensuring compliance with general data protection Rregulation (GDPR) regulations and ethical research standards.
Data Analysis
• Qualitative responses → thematic analysis
• Quantitative data → descriptive statistics (%)
• Comparative analysis between Spain and Portugal
Results
The survey was completed by 29 HCPs from renal care units and primary care center across Portugal and Spain. From the 29 full responses received, 14 were from HCPs from Portugal and 15 from Spanish healthcare professional.
Participant Characteristics
Table 1 shows the respondent characteristics
|
Variable |
Spain (%) |
Portugal (%) |
|
Primary Care Physicians |
60 |
62 |
|
Nephrologists |
40 |
38 |
|
>10 years experience |
55 |
58 |
|
Urban practice |
70 |
68 |
Table 1: Participant Characteristics
3.2 Key Barriers to CKD Diagnosis Table 2 shows the barriers facing during CKD management, and table 3 shows the comparison between the barriers revealed in both countries.
|
Barrier |
Spain (%) |
Portugal (%) |
|
Lack of training |
70 |
75 |
|
Communication issues |
65 |
70 |
|
Late referral |
55 |
60 |
|
Limited lab access |
50 |
55 |
Table 2: Key Barriers in CKD Management
|
Barrier |
Spain (%) |
Portugal (%) |
|
Training Gap |
70 |
75 |
|
Communication |
65 |
70 |
|
Late Referral |
55 |
60 |
|
Lab Access |
50 |
55 |
Table 3: Comparative Barriers (%)
Diagnostic Challenges
Respondents in both countries reported:
• Limited use of albuminuria testing
• Delayed access to laboratory results
• Insufficient decision-support tools Portuguese respondents more frequently emphasized lack of preparedness in primary care, consistent with qualitative findings.
Referral Patterns
Referral decisions were primarily based on:
• Decline in estimated glomerular filtration rate (eGFR)
• Elevated creatinine This indicates a late referral trend, associated with poorer clinical outcomes [14-16].
Communication Between Care Levels
Both countries reported:
• Fragmented Information and communication technlogy ICT systems
• Limited direct communication
• Reliance on patients for information transfer Portugal reported slightly greater communication challenges [17-20].
Improvement Strategies
Common recommendations included:
• Early screening programs
• Multidisciplinary care
• Patient education
• Integration of digital tools
Figure 1 shows the comparison of key barriers between Spain and Portugal, showing higher prevalence in Portugal across all domains [21-25].
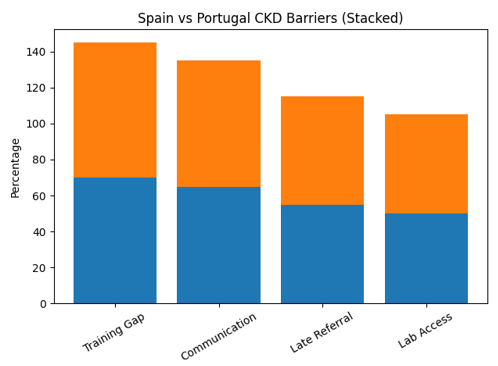
Figure 1. Comparative Barriers in CKD Management
Discussion
To answer the question about the challenges to coordinate the kidney patient management between several services the Spanish and Portuguese HCPs pointed to the same problem: the need of better training about kidney care for HCP in Primary Care. In addition, the Spanish and Portuguese HCPs, consider that the current tool available to support kidney disease prevention is the Patient education to be aware about their own lifestyle and medication.
Shared Challenges
Both Spain and Portugal demonstrate:
• Delayed CKD diagnosis
• Insufficient primary care training
• Poor coordination between care levels These findings align with global evidence on CKD care gaps [15].
Differences Between Countries Portugal shows:
• Higher perceived barriers
• Greater diagnostic delays Spain shows:
• Slightly better access to diagnostics
• But persistent structural fragmentation
Role of Digital Health
Integrated electronic health records and decision-support tools could:
• Improve early detection
• Enhance communication
• Reduce delays in referral [14,15,16].
Clinical Implications
Improving CKD care requires:
• Strengthening primary care
• Standardizing referral pathways
• Enhancing multidisciplinary collaboration [28-30].
Limitations
• Survey-based design
• Limited sample size
• Self-reported data
Conclusions
The results of this survey show that the implementation of prevention and sustainability policies can improve renal healthcare and patient outcomes.
Enhancing care to prevent the progression of disease, adopting telehealth, and focusing on exhaustive screening of patients and risk delaying or even avoiding advanced stages can reduce significant environmental impacts associated with CKD, including those from dialysis, hospital stays, and patient travel. The study highlights the need to evaluate environmental effects across full care pathways and calls for better prevention and the adoption of eco-friendly practices in nephrology units because respondents are not aware about the implemented measures to avoid or reduce environmental factors.
CKD diagnosis and management remain suboptimal in both Spain and Portugal. While challenges are shared, Portugal exhibits greater systemic barriers. Addressing these gaps requires coordinated efforts in training, digital integration, and early detection strategies.
Comparison of key barriers between Spain and Portugal, showing higher prevalence in Portugal across all domains.
Acknowledgements
We would like to extend our gratitude to the Portuguese and Spanish societies and associations of nephrology, as well as the nephrology nurses’ associations, nephrologists' associations, public and private nephrology units, and primary care centers who generously helped distribute the survey among healthcare professionals. We are also grateful to the healthcare professionals who took the time to complete the questionnaires.
Conflict of Interest Statement / Disclosure Statement
The author(s) declared that there is no potential conflict of interest concerning the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Despite the participant having to answer the first and mandatory question about consent to participate, we get the Ethical approval from Ethic Committee of Universidad Politécnica de Madrid. (See the supplemental Material).
Funding
The authors did not receive financial support for the research, authorship, and /or publication of this article.
Consent for publication / Informed consent
Consent was asked of all participants before starting to answer the questionnaire.
Author contributions
Abel Mata-Lima conceived and conducted the study. José Javier Serrano-Olmedo reviewed and edited the manuscript and approved the final version of the manuscript. Abel Mata-Lima conceptualized and developed the questionnaires and wrote the first draft of the manuscript. Abel Mata-Lima and José Javier Serrano-Olmedo undertook the survey review, distribution, and diffusion. J.J. Serrano provided project guidance and ethical approval management. Abel Mata-Lima and José Javier Serrano-Olmedo undertook the questionnaire and manuscript review and informed the interpretation of findings. All authors contributed significantly to the study design. Material preparation, data collection, and analysis were performed by all authors. All authors commented on previous versions of the manuscript, read and approved the final manuscript;
Abel Mata-Lima verifies the data used in these analyses. All authors confirm they ad full access to all the data in the study and accept responsibility to submit for publication.
Supplementary Material
The ethical approval – confidential
This article contains the following online survey questionnaires:
https://docs.google.com/forms/d/13b1kcaEBciRJHJzPjZGSF17v Q3fR3MCfbp1MEVKEBnU/edit?pli=1
https://docs.google.com/forms/d/1Owc81qpVVaPSsJBCEGonW9 UDC2Plu4DOyzR2zNSjCh0/edit
https://docs.google.com/forms/d/1auW31D99gzAgAcbC-fO7AIQvndz61TQUNzTeW_l_zbA/edit
References
- Webster, A. C., Nagler, E. V., Morton, R. L., & Masson, P. (2017). Chronic kidney disease. The lancet, 389(10075), 1238-1252.
- Levin, A., Stevens, P. E., Bilous, R. W., Coresh, J., DeFrancisco, A. L., De Jong, P. E., ... & Winearls, C. G. (2013). Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney international supplements, 3(1), 1-150.
- Kramer, A., Boenink, R., Noordzij, M., Bosdriesz, J. R., Stel,V. S., Beltrán, P., ... & Jager, K. J. (2020). The ERA-EDTA registry annual report 2017: a summary. Clinical kidney journal, 13(4), 693-709.
- McPherson, L., Plantinga, L. C., Howards, P. P., Kramer, M., & Patzer, R. E. (2025). Effect of pre–end-stage kidney disease nephrology care on the association between neighborhood poverty and referral for kidney transplantation among patients with end-stage kidney disease. Journal of Clinical Epidemiology, 185, 111878.
- Mills, K. T., Xu, Y., Zhang, W., Bundy, J. D., Chen, C. S., Kelly, T. N., ... & He, J. (2015). A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney international, 88(5), 950-957.
- Abdel-Kader, K., Greer, R. C., Boulware, L. E., & Unruh, M.L. (2014). Primary care physicians’ familiarity, beliefs, and perceived barriers to practice guidelines in non-diabetic CKD: a survey study. BMC nephrology, 15(1), 64.
- Fishbane, S., Agoritsas, S., Bellucci, A., Halinski, C., Shah,H. H., Sakhiya, V., & Balsam, L. (2017). Augmented nurse care management in CKD stages 4 to 5: a randomized trial. American Journal of Kidney Diseases, 70(4), 498-505.
- Jager, K. J., Kovesdy, C., Langham, R., Rosenberg, M., Jha, V., & Zoccali, C. (2019). A single number for advocacy and communication—worldwide more than 850 million individuals have kidney diseases. Nephrology Dialysis Transplantation, 34(11), 1803-1805.
- Kovesdy, C. P. (2022). Epidemiology of chronic kidney disease: an update 2022. Kidney international supplements, 12(1), 7-11.
- Yeo, S. C., Ooi, X. Y., & Tan, T. S. M. (2022). Sustainable kidney care delivery and climate change–a call to action. Globalization and health, 18(1), 75.
- Li, P. K. T., Garcia-Garcia, G., Lui, S. F., Andreoli, S., Fung,W. W. S., Hradsky, A., ... & Kalantar-Zadeh, K. (2020). Kidney health for everyone everywhere: from prevention to detection and equitable access to care. Canadian Journal of Kidney Health and Disease, 7, 2054358120910569.
- Garcia Sanchez, J. J., Barraclough, K. A., Cases, A., Pecoits-Filho, R., Germond-Duret, C., Zoccali, C., ... & Eckelman,M. J. (2025). Using chronic kidney disease as a model framework to estimate healthcare-related environmental impact. Advances in Therapy, 42(1), 348-361.
- Barraclough, K. A., & McAlister, S. (2022). Assessing the carbon footprint of hemodialysis: a first step toward environmentally sustainable kidney care. Journal of the American Society of Nephrology, 33(9), 1635-1637.
- Apel, C., Hornig, C., Maddux, F. W., Ketchersid, T., Yeung, J., & Guinsburg, A. (2021). Informed decision-making in delivery of dialysis: combining clinical outcomes with sustainability. Clinical Kidney Journal, 14(Supplement_4), i98-i113.
- Herrington, W. G., Judge, P. K., Grams, M. E., & Wanner,C. (2026). Chronic kidney disease. The Lancet, 407(10523), 90-104.
- Crewsa, D. C., & Bellod, A. K. (2019). Burden, Access, and Disparities in Kidney. Blood Purif, 48, 32-39.
- Herrington, W. G., Judge, P. K., Grams, M. E., & Wanner,C. (2026). Chronic kidney disease. The Lancet, 407(10523), 90-104.
- Levey, A. S., Schoolwerth, A. C., Burrows, N. R., Williams,D. E., Stith, K. R., & McClellan, W. (2009). Comprehensive public health strategies for preventing the development, progression, and complications of CKD: report of an expert panel convened by the Centers for Disease Control and Prevention. American Journal of Kidney Diseases, 53(3), 522-535.
- Garcia Sanchez, J. J., Barraclough, K. A., Cases, A., Pecoits-Filho, R., Germond-Duret, C., Zoccali, C., ... & Eckelman,M. J. (2025). Using chronic kidney disease as a model framework to estimate healthcare-related environmental impact. Advances in Therapy, 42(1), 348-361.
- Fackrell, K., Church, H., Crane, K., Recio-Saucedo, A., Blatch-Jones, A., & Meadmore, K. (2024). Online survey exploring researcher experiences of research funding processes in the UK: the effort and burden of applying for funding and fulfilling reporting requirements. BMJ open, 14(3), e079581.
- Satterwhite, S., Nguyen, M. L. T., Honcharov, V., McDermott,A. M., & Sarkar, U. (2024). “Good care is slow enough to be able to pay attention”: primary care time scarcity and patient safety. Journal of General Internal Medicine, 39(9), 1575.
- Hutton, L., & Henderson, T. (2015). " I didn't sign up for this!": informed consent in social network research. In Proceedings of the International AAAI Conference on Web and Social Media (Vol. 9, No. 1, pp. 178-187).
- Saunders, M. N., & Townsend, K. (2016). Reporting and justifying the number of interview participants in organization and workplace research. British journal of management, 27(4), 836-852.
- Indrayan, A., & Mishra, A. (2021). The importance of small samples in medical research. Journal of Postgraduate Medicine, 67(4), 219-223.
- Faber, J., & Fonseca, L. M. (2014). How sample size influences research outcomes. Dental press journal of orthodontics, 19, 27-29.
- Parker, R. A., & Cook, J. A. (2023). The importance of clinical importance when determining the target difference in sample size calculations. Trials, 24(1), 495.
- Boulware, L. E., Jaar, B. G., Tarver-Carr, M. E., Brancati, F. L., & Powe, N. R. (2003). Screening for proteinuria in US adults: a cost-effectiveness analysis. Jama, 290(23), 3101-3114.
- Komenda, P., Ferguson, T. W., Macdonald, K., Rigatto, C., Koolage, C., Sood, M. M., & Tangri, N. (2014). Cost-effectiveness of primary screening for CKD: a systematic review. American Journal of Kidney Diseases, 63(5), 789-797.
- LI, P. K. T., Chow, K. M., Matsuo, S., Yang, C. W., Jha, V.,Becker, G., ... & Tsukamoto, Y. (2011). Asian chronic kidney disease best practice recommendations: positional statements for early detection of chronic kidney disease from Asian Forum for Chronic Kidney Disease Initiatives (AFCKDI). Nephrology, 16(7), 633.
- LI, P. K. T., Chow, K. M., Matsuo, S., Yang, C. W., Jha, V.,Becker, G., ... & Tsukamoto, Y. (2011). Asian chronic kidney disease best practice recommendations: positional statements for early detection of chronic kidney disease from Asian Forum for Chronic Kidney Disease Initiatives (AFCKDI). Nephrology, 16(7), 633.