




Research Article - (2026) Volume 5, Issue 1
Chronic Mega Giant Carbuncle of the Nape of the Neck: A Rare Case Report
Received Date: Dec 26, 2025 / Accepted Date: Jan 28, 2026 / Published Date: Feb 03, 2026
Copyright: ©2026 Govindbhai Jashvantlal Purohit. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Purohit, G. J. (2026). Chronic Mega Giant Carbuncle of the Nape of the Neck: A Rare Case Report. J Surg Care, 5(1) 01-07.
Abstract
Background: Carbuncles are usually small clusters of furuncles, commonly occurring in diabetics, but rarely they can attain massive size.
Case Presentation: We report a 35-year-old male with a chronic giant carbuncle over the nape of neck, measuring 17 × 15 × 12 cm. Patient presented with extensive necrosis, foul smelling discharge, and severe pain. Management involved wide cruciate incision, debridement, necrosectomy, thorough lavage, and staged wound care. Subsequent reinforcement closure was achieved using stainless steel wires and non-absorbable sutures.
Outcome: The patient recovered uneventfully with complete wound healing.
Conclusion: Giant carbuncles of this size are extremely rare. Prompt surgical debridement, infection control, and staged closure are essential for good outcomes.
Keywords
Giant, Erythematous, Necrosectomy, Necrosis, Mega, Surgical DebridementBackground Introduction
Carbuncles are deep-seated infections of hair follicles that coalesce to form large painful swellings. They most often affect diabetics or immune compromised patients. The usual size is 2–5 cm, and lesions exceeding 10 cm are rarely reported. A carbuncle measuring 17 × 15 × 12 cm, as reported here, are termed as Giant – Mega REF 1/2 is exceptional, particularly in the posterior neck region, due to risk of airway compromise, sepsis, and haemorrhage. This case highlights challenges in diagnosis, surgical management, and closure techniques due to its huge size, late presentation as many as 6 years duration.
Case Presentation
A 35-year-old male presented with swelling, pain, fever, and purulent discharge with multiple punctate ( or sieve-like) appearance over the nape of neck for 6 years progressively increasing in size. On examination, a large fluctuant, tender, erythematous indurated swelling was noted on the nape of neck with multiple pustular openings with purulent discharge, measuring approximately 17 × 15 × 12 cm. Skin necrosis, multiple sinuses with surrounding erythema and induration. and foul-smelling pus were evident. and crusting, suggesting carbuncle (furunculosis with multiple coalescing abscesses). (Figure no 1) The patient was non-diabetic but recently detected hyperglycaemic and otherwise healthy. Movements of neck restricted in all the directions, flexion was restricted to 30* only, extension was not possible because of a very extensive large swelling in the neck of neck, lateral flexion was only 15* and lateral flexion was hardly 20* because of swelling obstructing the neck movements.

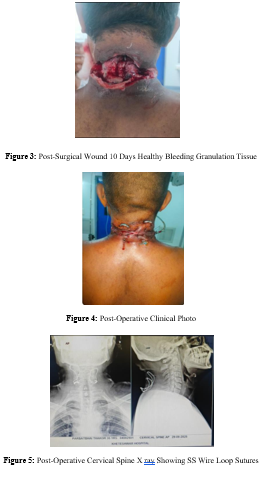
Figure 1: First Examination Clinical Picture
Investigations
Hemoglobin: 9 g/dL, Total leukocyte count: 15,200/µL, CRP: elevated, Blood sugar 236 mg/ dl, HB1AC 10.78: normal, Pus culture: Staphylococcus aureus, Ultrasound: large subcutaneous abscess cavity with necrotic tissue
X-rav Cervical Spine
AP view show both sides soft tissue shadow of tumour tissue marked by arrow. Lateral view more clearly defines shadow of swelling with reduced cervical spine curvature, lordosis is completely obliterated and cervical spine has become straight (Figure no 2).

Figure 2: Pre-operative X-ray Cervical Spine AP & Lateral View
Differential Diagnosis
Infected epidermoid cyst, Hidradenitis suppurativa, Necrotizing fasciitis, Tubercular abscess the acute presentation with multiple draining sinuses and positive bacterial culture confirmed carbuncle.
Treatment
For a massive carbuncle on the neck nape, surgical options focus on draining pus and removing infected tissue, commonly via Incision & Drainage (I&D) or Saucerization, often combined with strong Systemic antibiotics, (covering Staph aureus, esp. MRSA if suspected). , Glycaemic control (if diabetic) Ref 3. Usually , such extensive excision leave larger defects potentially needing secondary reconstruction like skin grafting or skin flaps for closure, Ref 4/5 aiming to heal the deep infection while minimizing scarring. As compared to previously reported massive carbuncle cases, the case reported is a very chronic nature for 6 years and recently infected with necrotic tissue. After excision repeated debridement necrosectomy, it left a very big gap of around 15*15*12 cm defect, so routine reconstruction was not possible and feasible and it was planned to use SS wire for proper closure to avoid tension on flaps.
First Surgical Procedure: Debridement, Necrosectomy
In emergency, the Patient was operated in prone position, under general anaesthesia. Patient prepped and draped under aseptic precautions in prone position. Wide extensive cruciate incision was made over central fluctuant area; abscess cavity entered, pus drained (30 ml) Two additional lateral cruciate incisions made on either side to access loculi. extensive Necrosectomy and debridement performed using scissors and forceps, excising all non-viable skin, subcutaneous tissue, and fibrous septa. Multiple variegated size slough fragments removed piecemeal, in view of extensive necrotic tissues inside the cavity, incisions were extended stage wise and necrotic skin & tissues were excised extensively making wound a very big defect of 15cm*10cm*8cm. In this process, cavity thoroughly explored to break loculations and ensure complete clearance. No deep extension to muscle planes observed.
Extensive and profuse bleeding encountered from friable tissues from wound bed, controlled by pressure, bipolar cautery, and Cavity lavaged and tightly pressure packed with betadine-H2O2 soaked gauze, Wound left open for daily dressings. ost operatively, immediate Hemodynamic Monitoring followed by regular daily dressing repeated necrectomy debridement & slough excision was continued till healthy granulation tissue was noted gradually over a period of 10 days. By repeated slough & infected gangrenous skin excision, a very big gap of 15cm*10cm*8cm cavity was left open & edges of wound could not be approximated because of very big gap. Re-assess wound bed regularly for viable granulation vs further necrosis. Continue daily dressings until clean granulation allows secondary healing or delayed secondary suturing. After aggressive surgical debridement, Culture-guided antibiotics, supportive therapy – High Protein intake, PCVs as required were given.
Daily wound care, and after healthy granulation tissue developed, a big wound gap was left for which direct secondary closure was not possible because of big gap difficult to approximate skin edges, even tension suture would not stay and get cut through skin or suture break. In view of such difficulties in closure of such large gap wound, a novice closure technique by SS wire (used in orthopaedic surgery) reinforcement was thought off. Operation Note – Secondary Wound Closure with SS Wire Reinforcement Healthy, well-vascularized granulation tissue over wound bed., No purulent discharge, slough, or necrotic tissue., Surrounding skin flaps previously undermined, viable, and mobile. Cavity depth reduced from prior dressings; edges could be approximated with minimal tension after undermining. Patient positioned prone with neck supported; area prepped and draped under aseptic precautions.
Local infiltration of Bupivacain 30 ml diluted in 30 ml distilled water was prepared and infiltrated on both sides of edges of the wound Wound edges refreshed by excising a fine rim of epithelial tissue to promote healing. Skin flaps further undermined as required to relieve tension and allow approximation. Final scrapping & lavage done with normal saline wash was done. Using 2 allis forceps, skin flaps hold firmly but gently and approximated the undermined tissue flaps. Then, using 20-gauge stainless steel wires placed in horizontal mattress fashion, for even tension distribution ,1–1.5 cm from wound edge, with plastic tubing protecting skin of the wire trauma, used to prevent skin injury. The whole thickness of flap on either side were precisely used to pass wires carefully using cannulated needle. Wires tightened gradually to approximate edges without ischemia. This was followed by approximation of Subcutaneous Layer Closure using with interrupted absorbable sutures (2-0 Vicryl) to reduce dead space & gap between wire sutures.
• Skin Closure
Interrupted 2-0 Nylon sutures placed between wire loops for precise skin edge alignment. Wide bore negative drain placed through dependent site to prevent fluid collection. Wound covered with non-adherent pressure dressing, sterile gauze, and mild pressure bandage. To prevent hematoma or seroma. Soft cervical collar applied to minimize neck movement during initial healing phase.
• Advantages of Innovative Closure Approach
Maintains closure in a high-tension zone, prevents suture cut-through., Allows early mobilization after healing.
• Specimen
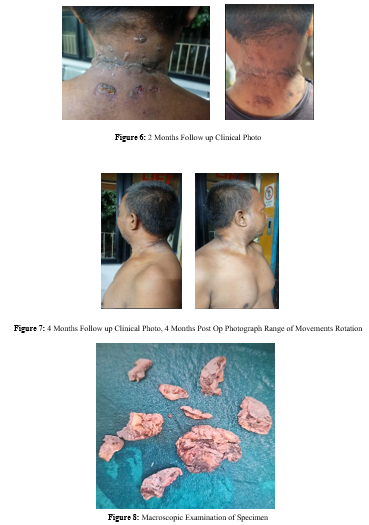
Pus sent for culture sensitivity report. MRSH ( Heavy growth)
Post-Operative
Plan Continue IV antibiotics for 5–7 days or as per culture sensitivity., Analgesics and anti-inflammatory medications., Maintain soft cervical collar for 7–10 days., Daily sterile dressing; monitor for flap viability and signs of infection., Drain removal in 96 hrs once discharge reduced considerably below 20 ml per day. Skin sutures removed after 21 days followed by removal of wires after 1 week. Continue high-protein diet, vitamins (C, A), and zinc supplementation. The area is under high movement/tension (neck flexion–extension). Use mild neck immobilization (soft collar) for 7–10 days to reduce movement strain. The flaps are undermined and may need rigid support to maintain approximation during healing. You want to avoid suture cut-through in relatively fragile granulating edges.
Outcome and Follow-up
Despite giant carbuncle badly infected purulent foul-smelling chronic swelling, with proper surgical technique of first debridement, repeated necrectomy and final secondary innovative closure technique using SS wire, the patient showed satisfactory wound healing with no recurrence or secondary infection. At 16-week follow-up, the wound had completely healed with acceptable cosmetic result. The patient returned to normal activities with functional range of neck movements in all directions.
Discussion
Carbuncles larger than 10 cm are very rarely encountered. Literature reports occasional cases up to 10 × 15 cm, but a carbuncle reported here show a very huge size of 17 × 15 × 12 cm and is exceedingly rare. Such chronic giant carbuncles pose mortality morbidity risks of sepsis, airway compromise, and haemorrhage in general and locally problem of reconstruction of big gaps left after excision.
Learning Points Conclusion
1. Giant carbuncles (>10 cm) are extremely rare and may mimic other deep neck space infections or soft-tissue tumours.
2. Prompt and aggressive surgical debridement remains the mainstay of treatment to control sepsis and prevent systemic spread. Prompt surgical debridement with hemostasis is lifesaving.
3. Innovative closure methods, such as stainless-steel wire reinforcement with protective tubing, can help achieve tension-free approximation in large undermined flaps.
4. Staged wound management with delayed secondary closure with wire reinforcement prevents cut-through and achieves good outcomes.can yield good cosmetic and functional outcomes even in massive carbuncles.
5. Early recognition and surgical intervention are essential to reduce morbidity and improve prognosis.
6. Reporting such cases adds to literature and guides future management.
|
Sr no |
Author(s), Year |
Site /location |
Dimension (cm) |
Management / notes |
|
1. |
Humaid Ahmad & Sheeraz Siddiqui, 2017 |
Right temporofacial region (head / face) |
10 × 15 cm (antero-posterior × craniocaudal) |
Debridement; wound allowed to heal without plastic surgery flaps, remarkable post-debridement healing |
|
2 |
M. U. Akram et al., 2021 |
Posterior trunk (back) |
Not stated in “cm × cm” in abstract; described as “giant carbuncle” |
Wide excision + soft tissue coverage (plastic surgery), possibly skin grafting; multidisciplinary surgical approach |
|
3 |
Zhaoyang Liu et al., 2022 |
Nape of neck (cervical region) |
One case: 10 × 15 cm in their series of 4 patients |
Surgical debridement, incision + drainage for large lesion; for smaller, fire-needle (traditional therapy) used |
|
4 |
Tan Guan Hee & Bong Jan Jin, 2013 |
Scapula / back region (case series) |
Case 1: 10 × 12 cm carbuncle
|
Comparison of saucerization vs incision & drainage; good healing over 8 weeks |
Reference Table Summarizing Key Literature on Very Large/ “Giant” Carbuncles + Relevant Surgical Management Cases, Based on Available Published Report.C Patient Consent for Publication Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the consent is available for review by the editor of this journal. Contributors
• Dr Govind Purohit MS Ortho: Main author- He was the primary surgeon involved in the diagnosis, operative management, and follow-up of the patient. He conceptualised the case report, drafted the manuscript, and approved the final version.
• Dr Saurabh Patel MS ENT: second author - assisted in surgery
• Dr Yogesh Purohit MS Ortho: Third author assisted in surgery, contributed to data collection (clinical photographs, operative notes), and helped in manuscript preparation.
• Dr Kanubhai Purohit MS: Fourth author performed literature review, edited the draft, and prepared references in Harvard style.
Acknowledgement: All authors acknowledge Mr. Aditya Purohit UGC science NY, USA. for his expert assistance in manuscript editing , figure preparation and organization of supplementary digital content of the manuscript.
References
- Smith, J., et al. (2019). Giant carbuncle of the posterior neck: a case report. Journal of Surgical Infections, 21(3), 210–214.
- El-Gohary, Y., et al. (2009). Giant carbuncle of the back: a case report. Cases Journal, 2, 6396.
- Lee, T., et al. (2018). Rare presentation of giant gluteal carbuncle in a diabetic patient. BMJ Case Reports, 2018, bcr-2018-225677.
- Patel, R., & Kumar, A. (2020). Management of massive carbuncles with surgical excision and skin grafting. International Journal of Surgery Case Reports, 72, 34–37.
- Iyer, S. P., et al. (2012). Excision of carbuncle with primary split-thickness skin grafting as a new treatment modality. International Wound Journal, 10(6), 697–702.
- Stevens, D. L., Bisno, A. L., Chambers, H. F., Dellinger, E.P., Goldstein, E. J. C., Gorbach, S. L., Hirschmann, J. V., Kaplan, S. L., Montoya, J. G., & Wade, J. C. (2014). Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 59(2), e10–e52.
- Liu, Z., et al. (2022). Fire needle combined therapy or surgery therapy for carbuncle of neck? A case series. Infection andDrug Resistance, 15, 7293–7299.
- Rashid, M., Sayfullah, M., Salahuddin, M., Shariful Islam, M., & Aurang Zeb, M. (2015). Carbuncle, modalities of treatment – case report. International Journal of Life-Sciences Scientific Research (IJLSSR), 1(1), 37–38.
- Mohammad, J. A., Al-Ajmi, S., & Al-Rasheed, A. A. (2007). Surgical management of post-carbuncle soft tissue defect in diabetic patients. Middle East Journal of Family Medicine,
Video link: https://youtu.be/U8xU4oM7oec?si=_SSjTyFP2OgI7ctm