
Journal of ENT Surgery Research(JESR)

Case Report - (2023) Volume 1, Issue 1
Cavernous Sinus Thrombosis as A Primary Presentation of Sinusitis. A Case Report and Literature Review.
2Alexandria University Medical School, Egypt
Received Date: May 08, 2023 / Accepted Date: Jun 15, 2023 / Published Date: Jun 24, 2023
Copyright: ©©2023 Nouri Alnouri MD, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Alnouri, N., Sobeih, A., Zahran, M. (2023) Cavernous Sinus Thrombosis as A Primary Presentation of Sinusitis. A Case Report and Literature Review. J of ENT Surgery Research, 1(1), 01-04.
Abstract
Cavernous sinus thrombosis (CST) is a rare, life-threatening condition that arises from infections in the head and neck. In this article, we present a rare case of septic CST as a primary presentation of paranasal sinusitis.
Furthermore, the anatomy of the cavernous sinus, etiologies of CST, and how to approach CST will be highlighted. In addition, the role of anticoagulants is emphasized after reviewing the literature.
Introduction
Cavernous sinus thrombosis (CST) is considered a rare, serious condition that is usually complicated by infections in the head and neck. Generally, infections in the Danger Triangle of the face (the area from the upper lip to the bridge of the nose) are the most common etiology of CST, especially paranasal sinusitis. Otogenic and odontogenic are less common etiologies [1]. CST is recognized for its high mortality and morbidity rate [2]. Nevertheless, the prognosis has improved with the advent of antibiotics. Early diagnosis can be crucial for a favorable outcome. However, long-term complications remain common. This article presents a case of cavernous sinus thrombosis as a primary presentation of paranasal sinusitis.
Case Report
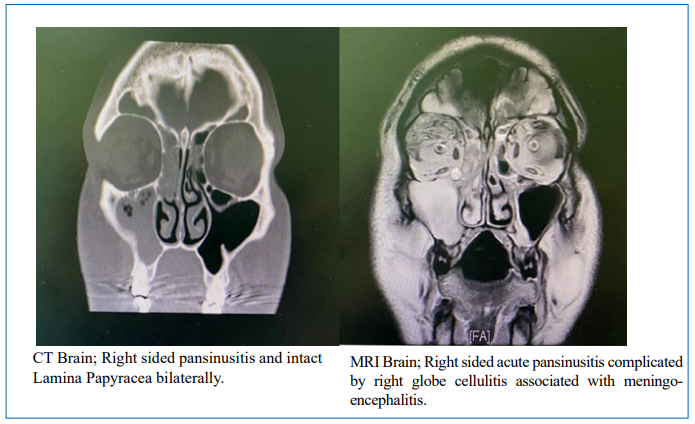
A 42-year-old gentleman, previously healthy, presented to the emergency department with a 1-day history of frontal headache associated with severe right eye pain, redness, and ptosis. On physical examination, he was conscious, alert, and fully oriented. Fever was documented at the time of the exam, while other vital signs were within normal range. He had severe right eye pain, periorbital swelling, and red conjunctiva. There was complete ptosis, proptosis, and restriction of right eye movement (3rd, 4th, and 6th cranial nerves partially affected). The facial sensation was intact, and meningeal signs were negative. Laboratory studies showed leukocytosis of 19.8x109 /L with a neutrophilic predominance of 75.3%, a hemoglobin level of 160 g/L, C- reactive protein (CRP) of 160 mg/L (reference range 0-8 mg/L), creatinine level of 117umol/L, sodium of 134 mmol/L and potassium of 4,42 mmol/L. Then, the patient was admitted for further evaluation, and empirical parenteral antibiotics (Ceftriaxone and Clindamycin) were initiated along with intravenous fluids and anticoagulant therapy (Subcutaneous Enoxaparin). Blood and urine cultures were obtained. CT Head was done and showed mucosal thickening of all visualized paranasal sinuses associated with an air-fluid level in both frontal and right maxillary sinuses.
Thus, the patient was diagnosed with septic CST as a result of acute rhinosinusitis. Subsequently, FESS was done to drain the sinuses. During navigation-guided surgery, bilateral middle meatal antrostomy, anterior and posterior ethmoidectomy, and removal of all air cells on the skull base were done. However, there were not any mucopurulent secretions. A middle meatal polyp biopsy was obtained and sent for histopathology. Later, the patient’s symptoms were resolved, and he completed a total of 3 weeks of antibiotics and anticoagulant therapy.
Discussion
Anatomy
The cavernous sinus is a paired sinus located on either side of the sella turcica of the sphenoid bone. It communicates with each other via anterior and posterior intercavernous sinuses. In addition to acting as a conduit for venous blood, Oculomotor nerve (CN III), Trochlear nerve (CN IV), Ophthalmic (V1), and maxillary (V2) branches of the trigeminal nerve travel through its lateral wall, and Abducens nerve (CN VI) and Internal carotid artery travels through its lumen. The cavernous sinus receives blood from the sphenoparietal sinuses, superior and inferior ophthalmic veins, and efferent hypophyseal veins. The cavernous sinus drains via the superior petrosal sinus to the sigmoid sinus and via the inferior petrosal sinus to the jugular bulb venous plexus to the basilar plexus. The cavernous sinus is valveless, which allows bidirectional blood flow.
Pathogenesis
Infections in the head and neck, especially from within the Danger triangle, can spread to the cavernous sinus by its valveless venous system. In addition, embolized bacteria in the cavernous sinus can provoke thrombosis, which acts as a trap and perfect media for bacterial growth [1, 3].
Etiology
CST can be either septic or aseptic. Generally, septic CST arises from infections in the Danger Triangle of the face (the area from the upper lip to the bridge of the nose). Notably, paranasal sinusitis (especially sphenoiditis and ethmoiditis) remains one of the most typical causes. The reason behind this fact is that sinusitis is less apparent than other facial infections. Therefore, facial infections can be recognized early and treated with antibiotics to avoid complications [1]. Otogenic and odontogenic are less common etiologies. Other causes of aseptic CST include maxillofacial surgery or trauma, pregnancy, oral contraceptives, dehydration, and hypercoagulable state are considered risk factors for CST. The causative organisms of CST are diverse. In most cases, bac- terial infections are responsible for thrombosis in the cavernous sinus. Staphylococcus aureus accounts for approximately two- thirds of cases [3]. Other less commonly typical organisms in- clude Pneumococcus, Haemophilus, Pseudomonas, Bacteroides, Corynebacterium, and Aspergillus [4].
Clinical features and presentation
In general, cases of CST present with headache, fever, signs of meningeal irritation (nuchal rigidity), and confusion. Fever is the most common sign of septic CST, which can often be documented as a “picket fence” pattern suggestive of septic thrombophlebitis. Other features of septic CST include tachycardia, hypotension, and coma.
Ophthalmic findings include ophthalmoplegia, periorbital ede- ma, ptosis, proptosis, and chemosis. These signs and symptoms are caused by venous congestion within orbital veins because of decreased blood flow by a thrombus in the cavernous sinuses [1]. Initially, symptoms start in one eye and progress to the other eye over time as cavernous sinuses are interconnected. Impaired ocular motility (especially eye abduction) remains a common ophthalmic complication. This can be explained as the abdu- cent nerve (VI CN) passing through the cavernous sinus lumen. Moreover, abnormal pupillary reflexes and Horner syndrome can present due to the involvement of the Oculomotor nerve (III CN) and sympathetic nerve plexus.
Hypoesthesia or hyperesthesia in areas supplied by Ophthalmic (V1), and maxillary (V2) branches of the trigeminal nerve, are reported in some cases [1].
Some patients may present with purulent nasal discharge, postnasal discharge, and facial tenderness as a picture of acute sinusitis.
Differential Diagnosis
Clinical features play a significant role in distinguishing CST from other differential diagnoses. Acute orbital conditions and cavernous sinus syndrome can resemble CST. Orbital cellulitis is one of the conditions that can mimic CST. Likewise, CST orbital cellulitis can be a complication of sinusitis. However, visual disturbance and unilateral course are evident in orbital cellulitis [5].
Rhinocerebral mucormycosis is an aggressive fungal infection of the paranasal sinuses and brain that can be a complication of septic CST. Therefore, early recognition and prompt management must avoid serious complications.
Other non-infectious conditions include superior orbital fissure syndrome, orbital apex syndrome, and Tolosa Hunt syndrome. Cavernous sinus syndrome is a differential diagnosis of CST and is commonly caused by tumors that locally compress the sinus. Moreover, internal carotid artery aneurysms and carotid- cavernous fistula can cause CST symptoms. Nevertheless, the absence of septic signs and meningism is a differentiation of septic CST.
Diagnosis
Along with clinical features, lab investigation and radiological imaging are essential to establish the diagnosis. Leukocytosis is reported in almost all cases of septic CST [1]. Elevated Procalcitonin (PCT) is also found in septic CST which is caused by bacterial infections. Blood culture can be supportive in recognizing the causative pathogen and targeting it with antibiotics accordingly. Moreover, C-reactive protein (CRP), Erythrocyte Sedimentation Rate (ESR), and D-dimer should be routinely evaluated. In addition, a CSF study is essential to rule out meningitis.
Radiological imaging plays a significant role in the diagnosis. Enhanced computed tomography (CT) or magnetic resonance imaging (MRI) is the optimal modality to confirm the diagnosis of CST [6]. A review of the literature shows that some authors favor MR imaging over CT for the diagnosis of CST due to false negative results in CT imaging until the late course of the disease and because enhanced MR imaging has superior quality [1, 2, 7]. In contrast, other authors prefer enhanced CT as the initial im- aging technique [8]. Nevertheless, negative CT findings cannot rule out CST if there is high clinical suspicion.
CT scan and MRI can reveal direct and indirect radiological signs of CST. A filling defect within the cavernous sinus is the main direct sign. Indirect signs include dilatation of the superior ophthalmic vein, exophthalmos, and soft tissue edema due to venous flow obstruction [2]. Other findings include narrowing or obstruction of the intercavernous segment of the internal carotid artery.
Treatment
Septic CST is a life-threatening condition with high mortality and morbidity. Therefore, parenteral antibiotics should be administered promptly if there is any clinical suspicion. Based on the most common causative pathogens, third-generation cephalosporin or a combination of penicillin and Clindamycin or Metronidazole are recommended to cover Staphylococcus aureus, Streptococcus species, gram-negative organisms, and anaerobic species. Antibiotics should be given for an extended period (at least two weeks. Antifungal therapy should be strongly considered with immunocompromised patients.
Elimination of the underlying infection is the mainstay of the treatment. In the case of paranasal sinusitis, Functional Endoscopic Sinus Surgery (FESS) should be done to explore and drain the source of infection.
In the English literature, the role of anticoagulation therapy in septic CST is still a matter of debate [9]. Therefore, retrospective studies were done to evaluate the benefit of anticoagulants for patients with CST. It was found that the mortality rate with anticoagulated patients was less [10]. In comparison, others found that morbidity was less in anticoagulated patients [11].
Moreover, a recent review showed full recovery and less mortality in patients treated with anticoagulants, yet no difference in morbidity [12]. In addition, Bhatia and Van der Poel recommended using anticoagulants as an adjunct to antibiotics in the absence of contraindications [1, 2].
Corticosteroids might be administered due to their beneficial effect in reducing inflammation and edema. However, corticosteroids are indicated to prevent adrenal crisis in the case of pituitary insufficiency.
Conclusion
CST is a complication of head and neck infections, especially pa- ranasal sinusitis. Fortunately, this fatal condition became rare in the era of antibiotics and advanced and obtainable radiological technologies. Nevertheless, prompt antibiotic therapy and elim- ination of the primary source of infection once there is clinical suspicion. Early recognition can significantly reduce the rate of morbidity and mortality.
Consent
Informed consent was taken from the patient before and after surgery.
Conflict of interest
The authors declare that there are no conflicts of interest regarding the publication of this article.
References
- Bhatia, K., & Jones, N. S. (2002). Septic cavernous sinus thrombosis secondary to sinusitis: are anticoagulants indi- cated? A review of the literature. The Journal of Laryngolo- gy & Otology, 116(9), 667-676.
- van der Poel, N. A., Mourits, M. P., de Win, M. M., Coutinho, J. M., & Dikkers, F. G. (2018). Prognosis of septic cavernous sinus thrombosis remarkably improved: a case series of 12 patients and literature review. European Archives of Oto-Rhino-Laryngology, 275, 2387-2395.
- Plewa, M. C., Tadi, P., & Gupta, M. (2022). Cavernous sinus thrombosis. In StatPearls [Internet]. StatPearls Publishing.
- Matthew, T. J. H., & Hussein, A. (2018). Atypical cavernous sinus thrombosis: a diagnosis challenge and dilemma. Cureus, 10(12).
- Mallick, A., Pathak, S. D., Shankar, S., & Sati, A. (2015).Early cavernous sinus thrombosis following unilateral pansinusitis in a child. Case Reports, 2015, bcr2014208441.
- Bhatia, H., Kaur, R., & Bedi, R. (2020). MR imaging of cavernous sinus thrombosis. European Journal of Radiology Open, 7, 100226.
- Eustis, H. S., Mafee, M. F., Walton, C., & Mondonca, J. (1998). MR imaging and CT of orbital infections and complications in acute rhinosinusitis. Radiologic Clinics of North America, 36(6), 1165-1183.
- Schuknecht, B., Simmen, D., Yüksel, C., & Valavanis, A. (1998). Tributary venosinus occlusion and septic cavernous sinus thrombosis: CT and MR findings. American journal of neuroradiology, 19(4), 617-626.
- Dolapsakis, C., Kranidioti, E., Katsila, S., & Samarkos,M. (2019). Cavernous sinus thrombosis due to ipsilateral sphenoid sinusitis. BMJ Case Reports CP, 12(1), e227302.
- Southwick, F. S., Richardson Jr, E. P., & Swartz, M. N. (1986). Septic thrombosis of the dural venous sinuses. Medicine, 65(2), 82-106.
- Levine, S. R., Twyman, R. E., & Gilman, S. (1988). The role of anticoagulation in cavernous sinus thrombosis. Neurology, 38(4), 517-517.
- Weerasinghe, D., & Lueck, C. J. (2016). Septic cavernous sinus thrombosis: case report and review of the literature. Neuro-ophthalmology, 40(6), 263-276.