



Research Article - (2023) Volume 8, Issue 2
Association of Apolipoprotein B /Apolipoprotein A-I Ratio with Cardio Metabolic Risk Biomarkers in Type 2 Diabetes Mellitus
2Associate Professor and Head, Department of Biochemistry, Maharajgunj Medical Campus, Nepal
3Associate Professor, Department of Biochemistry, Maharajgunj Medical Campus, Institute of Medicine, Nepal
4Clinical Register, Department of Internal Medicine, Institute of Medicine Kathmandu, Nepal
5Lecturer, Department of Biochemistry, KIST Medical College and Teaching Hospital, Nepal
6Student, M.sc, Clinical Biochemistry, Maharajgunj Medical Campus Institute of Medicine, Nepal
7Clinical Biochemist, Care diagnostic laboratory, Nepal
Received Date: Apr 18, 2023 / Accepted Date: May 25, 2023 / Published Date: Jul 03, 2023
Copyright: ©Ã?©2023 Vijay Kumar Sharma, et, al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Makaju, H. S., Sharma, V. K., Yadav, B. K., Tuladhar, E. T., Bhandari, R., et, al. (2023). Association of Apolipoprotein B /Apolipoprotein A-I Ratio with Cardio Metabolic Risk Biomarkers in Type 2 Diabetes Mellitus. Cardio Open, 8(2), 30-39.
Abstract
Background: Individuals diagnosed with Type 2 Diabetes Mellitus and metabolic syndrome are at a heightened risk for cardiovascular disease. Apolipoprotein B (Apo B) is a reliable measure for assessing atherogenic particles, while Apolipoprotein A-I (ApoA-I) plays a key role in antiatherogenic high-density lipoproteins. Timely identification and evaluation of cardio metabolic risk factors can decrease the likelihood of developing CVD.
Objectives: This study aimed to evaluate the association of Apo B/Apo A-I ratio with cardiometabolic risk biomarkers in T2DM.
Materials and Methods: This cross-sectional study conducted at Tribhuvan University Teaching Hospital and involved 120 individuals diagnosed with Type 2 Diabetes Mellitus who visited the Medicine Outpatient Department, as well as 120 apparently healthy controls. Clinical and anthropometric characteristics were documented using a clinical profor- ma, and fasting blood samples were collected for the estimation of plasma glucose, Apolipoprotein B (ApoB), Apolipo- protein A-I (ApoA-I), traditional lipid profile analysis, and calculation of the Apolipoprotein B/Apolipoprotein A-I ratio.
Results: The mean values of cardiometabolic risk biomarkers and Apo B/Apo A-I ratio in patients with T2DM were significantly higher, whereas HDL-C was significantly lower than that of a control group (p≤0.001). The Apo B/Apo A-I ratio was strongly positively correlated with LDL-C, TC, Non-HDL-C, and Apo B (r=0.68-0.89, p<0.001) and modestly positively correlated with BMI, WC, TG, and VLDL-C (r=0.55-0.67, p<0.001). Additionally, there was a weak but sig- nificant positive correlation (r=0.18-0.35, p<0.05) with weight, systolic blood pressure, and fasting blood glucose. On the other hand, the Apo B/Apo A-I ratio showed a negative correlation with HDL-C and Apo A-I (r = -0.58, p<0.001).
Conclusion: The present study demonstrated that an elevated Apo B/Apo A-I ratio constituted a good association with several cardiometabolic biomarkers and supports that the Apo B/Apo A-I ratio as a potentially useful risk marker for predicting future cardiovascular disease in patients with type 2 diabetes mellitus.
Keywords
Type2 Diabetes Mellitus, Metabolic Syndrome, Apo B/Apo A-I Ratio, Cardiometabolic Risk Factor
Introduction
Type 2 Diabetes Mellitus (T2DM), the most prevalent category, caused by a combination of resistance to insulin action and inad- equate compensatory insulin secretion. In Nepal, the estimated pooled prevalence of T2DM was 8.4% in 2015, highlighting the significant burden of this disease in the country [1]. The num- ber of deaths accounted by Diabetes Mellitus were 1270 males, 1080 females in age group 30-69 years, 1370 males, and 1430 females in the age group above 70 yrs [2]. There was 451 mil- lion (age 18-99 years) people suffering from diabetes worldwide and expected to increase to 693 million by 2045 [3]. Individuals with T2DM have a twofold increased risk for cardiovascular dis- ease (CVD), which includes myocardial infarction, stroke, and peripheral vascular disease. The principal reasons for death in T2DM patients are CVD. Nearly 80% of the mortality in T2DM is because of CVD [4]. The cluster of cardio vascular (CV)/ metabolic syndrome (MetS) is a major factor responsible for in- creased CV risk in T2DM [5,6].
Cardiometabolic risk factors includes abdominal obesity, impaired fasting glucose level, hypertension and blood lipid disturbances like low levels of HDL, high fasting and postprandial levels of triglyceride -rich lipoproteins, and elevated levels of small dense LDL particles. All these cluster of cardiometabolic risk factors in- dicates the MetS. Cardiometabolic risk factor increases the threat of cardiovascular disease occurrence and mortality. Apolipopro- teins, a protein component of lipoproteins, are expressed mainly in the liver, partly in the intestine and other tissue.7 Apolipopro- tein in the lipoprotein are carriers of hydrophobic molecules like triglycerides and cholesterol esters in the plasma aqueous medi- um, ligands to the specific receptors on the cell surface of target organ and as coenzymes [7-9]. Apolipoprotein B (Apo B) is an essential structural component of very low-density lipoproteins (VLDL), intermediate-density lipoproteins (IDL), and low-den- sity lipoproteins (LDL). Each of these lipoproteins have Apo B apolipoprotein such that the measurement of Apo B level in plas- ma will represent the total atherogenic particles [10].
Apolipoprotein A-I (Apo A-I) is the major apolipoprotein asso- ciated with high density lipoprotein (HDL). Apo A-I is the main initiator and driver of reverse cholesterol transport. Apo A-I is also responsible for anti-oxidant and anti-inflammatory effects of the HDL. Thus Apo A-I exhibits several anti-atherogenic ef- fects [11]. Therefore, Apo B/Apo A-I ratio reflects the cholesterol balance of the potentially atherogenic and anti-atherogenic lipo- protein particles. Subsequently, its high value would indicate an increased trend to cholesterol deposition, endothelial dysfunction and consequently, higher risk of atherogenesis [12,13]. Several researchers have published their research regarding the benefit of Apo B/Apo A-I ratio in ruling out CVD risk; however, in Nepal the study on Apo B/Apo A-I ratio in patient with T2DM has not been reported till date. Therefore, this study is designed with the aim of investigating the association of Apo B/Apo A-I ratio with cardiometabolic risk variables in T2DM. Apo B/Apo A-I ratio can be a better marker for prediction of cardiovascular risk. As the principal cause of death in T2DM patients is CVD, knowing the Apo B/Apo A-I ratio we can reduce the cardiovascular risk.
Materials and Methods
The cross-sectional study was conducted at the Department of Biochemistry in Tribhuvan University Teaching Hospital, Kath- mandu. From July to December 2021, 120 individuals diag- nosed with type 2 diabetes mellitus visiting the Medicine OPD and 120 apparently healthy controls were included in the study after obtaining approval from the Institutional Review Commit- tee (IRC). All study participants were classified according to the NCEP ATP III criteria of Metabolic Syndrome. The control group consisted of individuals without diabetes mellitus, who had no general health complaints, were not taking any medica- tion, and provided written consent.
Anthropometry Measurements
Standardized stadiometer and scale were employed for measur- ing the height and weight respectively. The circumference mid- point between the lowest rib and the iliac crest was detailed as WC. Measurements were carried out with a standardized tape measure, and were rounded off to the nearest centimeter (cm). Blood pressure (BP) was measured by the Korotkov method at rest in a sitting position with a membrane sphygmomanometer as per ESC [14].
Laboratory Analysis
Fasting blood was sampled, after an overnight fast (8-12 hours) and serum samples were separated for analysis. Lipid profiles and fasting glucose were measured using fully automatic bio- chemistry analyzers (BT 1500 chemistry analyzer). The mea- surement of Apo A-I and Apo B was done using the immunotur- bidimetric method (Agappe Diagnostics). HBA1C was analyzed in EDTA samples using the Hb-vario HPLC analyzer. All lab- oratory analyses were conducted following standard operating procedures of the laboratory.
Calculation
Body mass index (BMI) was represented as the body weight (kg) divided by height squared (m2). The Apo B/Apo A-I ratio was calculated after measuring the Apolipoprotein B and Apolipo- protein A-I.
Statistical Analysis
Statistical analyses were done by SPSS 20.0version (Statistical Package for Social Science for windows version). Results are presented, as means {±standard deviation (SD) .The significance of differences between means was assessed using Student’s t test for data sets. Relationships between quantitative variables were analyzed using Spearman’s correlation coefficient. Results were considered as statistically significant or non-significant (NS) for p <0.05 or p>0.05, respectively.
Results
Demographic Distribution of Study Population
In this study 120 T2DM patient with mean age of 54.83 ± 9.578 years as cases and 120 apparently healthy participants with mean age of 54.63 ± 9.44 years as control were recruited. Among them, the numbers of male and female were 129 and 111 respectively Table 1. Most of T2DM patients and controls were from 46-55 years of age group. Similarly, the least number of cases and controls belong to age group of 35-45 years and of 66-75 years, respectively in Figure 1.
|
Gender |
Cases |
Controls |
|
Male |
64(53.3%) |
65(54.2%) |
|
Female |
56(46.7%) |
55(45.8%) |
|
Total |
120(100%) |
120(100%) |
Table 1: Demographic Distribution of Subjects
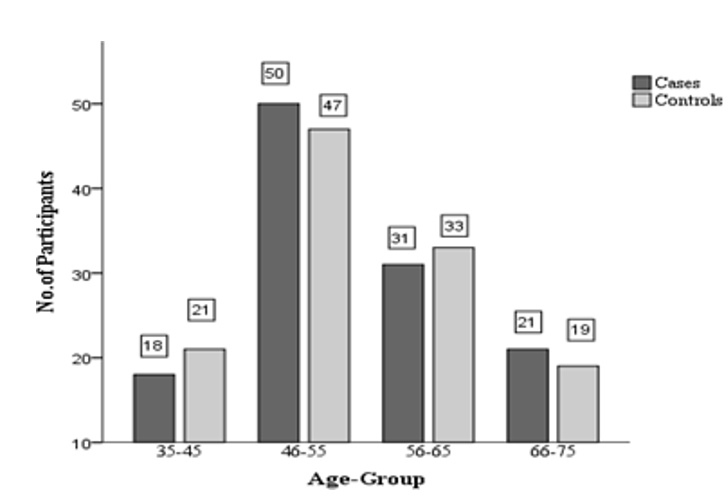
Figure 1: Age Wise Distribution of Cases and Controls
Anthropometric and Biochemical Characteristic of T2DM and Controls
While comparing the anthropometric and biochemical data be- tween T2DM patients and controls, the mean values of Weight, BMI, WC, SBP, DBP, FBG, HbA1C, TC, TG, LDL-C, VLDL-C, Non HDL-C, Apo B, Apo B/Apo A-I ratio were found to be sig- nificantly elevated in T2DM, but that of Apo A-I and HDL-C were higher in healthy controls. The mean value of HDL-C is statistically significant between cases and controls. The mean values of various Variables (with S.D), cases and controls, along with their corresponding p values are shown in Table 2.
|
Variables |
Cases (Mean ± S.D) N=120 |
Controls (Mean ± S.D) N=120 |
p value |
|
Age(yrs) |
54.83 ± 9.578 |
54.63 ± 9.44 |
0.874 |
|
Height (cm) |
155.50 ± 10.06 |
155.8917 ± 9.94 |
0.986 |
|
Weight (kg) |
61.96 ± 10.96 |
57.59 ± 8.587 |
0.010 |
|
BMI (kg/m2) |
25.43 ± 2.93 |
23.59 ± 1.70 |
<0.001 |
|
WC (cm) |
94.14 ± 9.41 |
84.15 ± 4.28 |
<0.001 |
|
SBP (mmHg) |
127.37 ± 8.71 |
120.58 ± 5.91 |
<0.001 |
|
DBP (mmHg) |
86.45 ± 7.31 |
79.87 ± 4.46 |
<0.001 |
|
FBG (mg/dL) |
151.28 ± 58.14 |
93.45 ± 12.62 |
<0.001 |
|
HbA1C (%) |
7.88 ± 1.51 |
5.45 ± 0.63 |
<0.001 |
|
TC (mg/dL) |
183.17 ± 39.58 |
148.15 ± 17.30 |
<0.001 |
|
TG (mg/dL) |
167.36 ± 76.33 |
113.35 ± 40.70 |
<0.001 |
|
HDL-C (mg/dL) |
36.78 ± 5.05 |
41.84 ± 4.21 |
<0.001 |
|
LDL-C (mg/dL) |
112.81 ± 36.28 |
83.88 ± 16.66 |
<0.001 |
|
VLDL-C (mg/dL) |
33.45 ± 15.23 |
22.67 ± 8.14 |
<0.001 |
|
Non HDL-C(mg/dL) |
146.39 ± 41.27 |
106.01 ± 18.60 |
<0.001 |
|
Apo B (mg/dL) |
107.50 ± 27.19 |
81.77 ± 16.13 |
<0.001 |
|
Apo A-I (mg/dL) |
104.64 ± 13.28 |
116.52 ±12.22 |
0.135 |
|
Apo B/Apo A-I |
1.04 ± 0.31 |
0.70 ± 0.15 |
<0.001 |
Table 2: Anthropometric and Biochemical Characteristic of Cases and Controls
Distribution of Study Population by Apo B/Apo A-I Ra- tio Level
Categorized Apo B /Apo A-I ratio was compared between case and control population. This ratio was found to be elevated in the diabetic population group compared to the age- and sex- matched control group Figure 2. In diabetic patients, 54 (45.0%) had desirable level while 66 (55.0%) had CHD risk level of Apo B/Apo A-I ratio.Whereas in control group,114 (95.0%) had ac- ceptable and 6 (5.0%) had CHD risk levels of ApoB/Apo A-I. The frequencies of participants in different categories are shown in Figure 3.

Figure 2: Box Plot Showing Comparison of Apo B/Apo A-I in T2DM Patients and Controls
Figure 3: Distribution of Apo B/Apo A-I Ratio Levels in Cases and Controls
Correlation of Apo B/Apo A-I Ratio with Others Car- diometabolic Risk Biomarkers in T2DM
Apo B/Apo A-I ratio was found to be significantly correlated with Weight, BMI, WC, SBP, FBG, TC, TG, HDL-C, LDL-C, VLDL-C, Non-HDL-C, Apo B, and Apo A-I ratio, whereas the correlation with Height and DBP was statistically insignificant.. There was a strong positive correlation between the Apo B/Apo A-I ratio and LDL-C, TC, Non-HDL-C, and Apo B (r=0.68-0.89, p<0.001). Similarly, modest positive correlation with BMI, WC, TG and VLDL-C (r=0.55-0.67, p<0.001) and a weak, yet sig- nificant, correlation (r=0.18-0.35 p<0.05) with weight, systolic blood pressure and FBG. In contrast, the ratio showed negative correlation with HDL-C and Apo A-I (r = -0.58, p<0.001). The correlation coefficients of Apo B/Apo A-I with these parameters, along with the respective p values are shown in Table 3.
|
|
Apo B/Apo A-I Ratio |
|
|
Variables |
Correlation Coefficient ® |
p value |
|
Height (cm) |
-0.039 |
.670 |
|
Weight (kg) |
0.357 |
<0.001 |
|
BMI (kg/m2) |
0.614 |
<0.001 |
|
WC (cm) |
0.669 |
<0.001 |
|
SBP (mmHg) |
0.187 |
0.040 |
|
DBP (mmHg) |
0.171 |
0.062 |
|
FBG (mg/dL) |
0.294 |
0.001 |
|
TC (mg/dL) |
0.861 |
<0.001 |
|
TG (mg/dL) |
0.553 |
<0.001 |
|
HDL-C (mg/dL) |
-0.557 |
<0.001 |
|
LDL-C (mg/dL) |
0.766 |
<0.001 |
|
VLDL-C (mg/dL) |
0.553 |
<0.001 |
|
Non HDL-C (mg/dL) |
0.894 |
<0.001 |
|
Apo B (mg/dL) |
0.898 |
<0.001 |
|
Apo A-I |
-0.580 |
<0.001 |
Table 3: Correlation of Apo B/Apo A-I with Various Cardiometabolic Risk Biomarkers
Anthropometric and Biochemical Characteristics of T2DM with and without Metabolic Syndrome
Comparing the anthropometric and biochemical parameters between the diabetic with MetS and without MetS, the mean values of Weight, BMI, WC, FBG, HbA1C, TC, TG,HDL-C, LDL-C, VLDL-C, Non-HDL-C, Apo B, Apo B/Apo A-I ratio were significantly difference. However, the mean values of age, height, SBP, DBP and Apo A-I were statistically insignificant (p > 0.05). The mean values of different variables (with S.D), of both MetS and Non- MetS, along with their corresponding p values are shown in Table 4
|
Variables |
MetS (Mean ± S.D) N=93 |
Non-MetS (Mean ± S.D) N=27 |
p value |
|
Age(yrs) |
54.89 ± 8.93 |
54.63 ± 11.72 |
0.078 |
|
Height (cm) |
155.92 ± 10.25 |
154.07 ± 9.41 |
0.352 |
|
Weight (kg) |
64.56 ±10.60 |
53.00±6.71 |
0.010 |
|
BMI (kg/m2) |
26.35±2.58 |
22.26±1.50 |
0.006 |
|
WC (cm) |
97.34±7.90 |
83.11±4.69 |
0.001 |
|
SBP (mmHg) |
128.76±8.617 |
122.77±7.63 |
0.880 |
|
DBP (mmHg) |
87.63±7.28 |
82.22±5.60 |
0.284 |
|
FBG (mg/dL) |
163.75±57.63 |
108.33±35.36 |
0.001 |
|
HbA1C (%) |
8.24±1.48 |
6.64±0.81 |
<0.001 |
|
TC (mg/dL) |
194.26±37.55 |
144.96±15.01 |
<0.001 |
|
TG (mg/dL) |
184.52±76.78 |
108.25±33.52 |
<0.001 |
|
HDL-C (mg/dL) |
35.43±4.54 |
41.44±3.84 |
0.045 |
|
LDL-C (mg/dL) |
121.80±35.84 |
81.85±14.05 |
<0.001 |
|
VLDL-C (mg/dL) |
36.88±15.31 |
21.65±6.70 |
<0.001 |
|
Non HDL-C (mg/dL) |
158.83±38.07 |
103.51±14.36 |
<0.001 |
|
Apo B (mg/dL) |
115.22±25.03 |
80.88±14.78 |
0.018 |
|
Apo A-I (mg/dL) |
101.36±11.75 |
115.92±12.17 |
0.992 |
|
Apo B/Apo A-I |
1.1428±0.27 |
0.7015±0.13 |
0.002 |
Table 4: Anthropometric and Biochemical Characteristic of Diabetes with Metabolic Syndrome and without Metabolic Syndrome
Predictive Significance of Apo B/Apo A-I Ratio for Dia- betes Mellitus with Metabolic Syndrome
To study the potential of Apo B/Apo A-I ratio to predict the dia- betic metabolic syndrome, ROC curve was plotted. At the cut-off value of Apo B/Apo A-I ratio of 0.86, the sensitivity and spec- ificity were 89.2% and 85.2%, respectively. Increasing the cut- off to 0.90 the sensitivity dropped to 82.8% and the specificity increased to 92.6 %. The ROC Curve showed an area under the curve value of 0.938 (95% CI: 0.897- 0.980, P<0.001) Figure 4.

Figure 4: ROC Curve Plot of Apo B/Apo A-I Ratio for Diabetic with Metabolic Syndrome
Discussion
Present study was conducted to find the association of Apo B/ Apo A-I ratio with various cardiometabolic risk biomarkers like height, weight, BMI, waist circumference systolic and diastolic blood pressure, total cholesterol, triglycerides, HDL-C, LDL-C, VLDL-C, Non-HDL-C, Apo B, Apo A-I in T2DM. Majority of the diabetic patients (68.4%) were aged 46-65 years. This result is similar with the global estimates of diabetes where the major- ity of diabetic patients in developing countries are between 40 and 60 years [15]. The NCEP ATP-III definition of MetS was used here for describing the diabetic patients with or without metabolic syndrome [16]. Regarding the anthropometric mea- sures, the mean differences between diabetic and healthy con- trols were significant in the context of BMI, WC, systolic and diastolic blood pressure. However, the significant mean differ- ences were noted for diabetic with metabolic syndrome in BMI (p = 0.006) and WC (p = 0.001) compared to diabetic without metabolic syndrome. Thus, WC and BMI anthropometric mark- ers need to be rigorously monitored to delay or prevent MetS and consequently the greater risk of CVD.
In addition to blood sugar and HbA1c, lipid profiles (TC, TG, HDL-C, LDL-C, VLDL-C and Non- HDL-C) were significantly deranged in T2DM compared to healthy controls. Our pattern of lipid profile derangement was similar to previous studies done on diabetics, showing increased levels of TC, TG, and LDL-C and decreased levels of HDL-C [17-20]. In this study, Apo B/ Apo A-I ratio was elevated in diabetic patients and diabetes with metabolic syndrome, putting this group and subgroup in CHD risk level. Increased Apo B/Apo A-I ratio level was also significantly increased in diabetic patients, which is in agree- ment with results of Gao l et al [21]. Jun JE et al. publicized that an increased Apo B/Apo A-I ratio was significantly linked with carotid atherosclerosis in low LDL-C level T2DM patient [22]. Increased Apo B/Apo A-I ratio is associated with increased CVD risk in young people. Several large studies realized that the ApoB/ApoA-I ratio was potently predictive of MI risk. The AM- ORIS (Apolipoprotein-related Mortality Risk) study showed that ApoA-ApoB, the ApoB/ApoA-I ratio and I were stronger predictors of fatal MI risk than TC or TG [23].
In this study, Apo B/Apo A-I ratio has shown good association with cardiometabolic risk markers, the positive correlation with various variables of the study was observed except for HDL-C and Apo A-I. This study showed that, LDL, TC and TG were positively correlated with Apo- B and Apo- B was negatively correlated with HDL-C are in keeping with Kumar S et al, and Katulanda GW et al and also with non HDL cholesterol like Adaja T et al and Jiang R et al who showed that there was a positive correlation of Apo B between TC, LDL-C, Non HDL-C [24-27]. In contrast to Adaja T et al this study showed the cor- relation of Apo B with BMI and TG [26].
The combined effect of Apo B and Apo A-I is realized in the Apo B/Apo A-I ratio, which showed a highly significant correlation with cardiometabolic risk biomarkers. Recent studies have used the Apo B/Apo A-I ratio is associated with cardiometabolic risk biomerkers [28]. The findings were consistent with Sahadevan DC et al described a relation between the Apo B/Apo AI ratio and cardiometabolic risk factors in patients with MetS and pa- tients without MetS, and the study reported a higher Apo B/Apo A-I ratio in the MetS subjects than the control subjects [28]. Apo B/Apo A-I ratio was positively associated with various car- diometabolic risk factors including TG, WC, systolic and dia- stolic blood pressure, and fasting plasma glucose, The number of MetS components may have a relationship with Apo B/Apo A-I ratio [12,29]. To the best our knowledge, our study is the first to demonstrate a significant association of the Apo B/Apo A-I ratio with various cardiometabolic risk biomarkers (Weight, BMI, WC, SBP, FBG, TC, TG, HDL-C, LDL-C, VLDL-C, Non HDL-C, Apo B, HDL-C and Apo A-I) in T2DM in Nepalese population.
There is substantial evidence from epidemiological studies sup- porting a high Apo B/Apo A-I ratio as a promising risk marker of future cardiovascular events better than any of the cholesterol indexes [30-33]. Moreover, several earlier cross-sectional stud- ies have demonstrated that the Apo B/Apo A-I ratio was sig- nificantly associated with MetS and its components independent of conventional risk factors [12,34-36]. Apo B/Apo A-I ratio is significantly associated with the major aspects of dyslipidemia, as well as insulin resistance, and the metabolic syndrome, mak- ing it an supreme marker for increased cardiovascular risk aside from the conventional lipid markers [13].
Schmidt et al, prospective study, comprising 391 adult males who were followed up for 6.6 years, it was perceived that the Apo B/Apo A-I ratio showed an association with atherosclero- sis in the femoral artery and increased cardiovascular risk [37]. The three large cohort studies had demonstrated a consistent outcome that both Apo B and Apo A-I were unbiased and equal predictive values, and Apo B/Apo A-I ratio was the strongest and most precise indicator for cardiovascular disease that was superior to the cholesterol ratios [30,38,39]. Therefore, Apo B/ Apo A-I ratio demonstrates better ascendency over the choles- terol ratios in terms of predictive ability.
ROC analysis was performed in our study to assess the cut-off diagnostic value of Apo-B/Apo-A-1 ratio for diabetic patients with metabolic syndrome. The optimal cut-off value of Apo-B/ Apo-A-1 ratio for diabetic mellitus with metabolic syndrome detection was 0.86 with a sensitivity of 89.2% and a specificity of 85.2%. Adequate cut-off for the prediction of diabetes with MetS is not well established but few studies have determined the appropriate cut-off values of the Apo B/Apo A-I ratio for the detection of MetS in individuals. Pistavos et al suggested a ratio of 0.73 as an optimal cut-off for predicting metabolic syndrome, with a sensitivity of 74% and a specificity of 67% in Greek pop- ulation [40]. Jung et al. reported the sex-specific optimal Apo B/Apo A-I ratio cut-off values in a Korean population, 0.65 in men and 0.62 in women [36]. Besides, Jing et al. suggested an optimal Apo B/Apo A-I ratio cut-off value of 0.85 in men and 0.80 in women in a Chinese population [35]. Correspondingly, The INTERHEART and AMORIS studies advised that an Apo B/Apo A-I ratio of 0.90 for men and 0.80 for women were in- dicative of a high CVD risk, and values of less than 0.70 in men and 0.60 in women were considered to indicate low CVD risk if no other risk factors were present [23,41]. These differences of Apo B/Apo A-I ratio cut off could be due to the genetic poly- morphisms, geographical variation, ethnicity, diet and difference in sample size. Medical evidence for Apo B/Apo A-I ratio in the prediction of diabetic with metabolic syndrome is insufficient. Thus, additional studies are necessitated to further strengthen the advantage of this parameter.
Apolipoprotein consider as a chief of all for predicting risk of CVD [42]. CVD is the chief cause of mortality and morbidity in diabetic patient and the NCEP III has termed diabetes a cor-onary heart disease risk correspondent [43,44]. The Apo B/Apo A-I ratios has many benefits that exceed their use compared with normal lipid parameters and their ratios in predicting CVD. As Apo B/Apo A-I ratio reflects the balance of atherogenic and ath- eroprotective particles as they represent the amount of vehicles to carry cholesterol. So elevated the level, the greater the tenden- cy of cholesterol deposition, and consequently the higher risk of CVD [45]. Another important feature, the concentration of apo- lipoproteins are not affected by meals and are slightly influenced by biological variables, unlike the ordinary lipid parameters, which fluctuate widely depending on food intake. Therefore, apolipoproteins measure does not require fasting blood samples [23,46-48]. Consistently, in clinical practice, apolipoproteins B and apolipoprotein A-I may be measured directly in plasma us- ing internationally standardized method without noticeable in- terference with high triglyceride levels [8,46].
Limitation
• This study was performed using a cross-sectional design and did not control for potential biases from physical activity, diet, drinking and smoking history.
• This study did not assess long-term outcomes with respect to the occurrence of CVD and the levels of lipid parameters.
• The study would not show the relation of Apo B /Apo A-I ra- tio with different biomarkers of inflammation which are also re- sponsible for the CVD.
Conclusion
In conclusion, the present study demonstrated that an elevated Apo B/Apo A-I ratio constituted a good association with car- diometabolic biomarkers and supports that the Apo B/Apo A-I ratio as a promising marker of future cardiovascular disease. WC and BMI anthropometric markers can also be rigorously monitored to delay or prevent MetS and consequently the great- er risk of CVD.
Recommendation
Apo B/Apo A-I ratio associated with biomarkers of cardiometa- bolic risk can be used as potential marker for diagnosis of meta- bolic syndrome. Metabolic syndrome is major worldwide public health challenge meanwhile it is associated two- to three-fold risk of CVD. As Apo B/Apo A-I ratio reflects the balance of ath- erogenic and atheroprotective particles, so elevated the level, the greater the tendency of cholesterol deposition, and consequent- ly the higher the risk of CVD. Due to dual function of Apo B/ Apo A-I ratio, it is recommended to incorporate in routine test. Methods for determining Apo B and Apo A-I are international- ly standardized and automated, analyses are cheap, and more importantly, can be performed on non-fasting samples. Further examination of the association of Apo B/Apo A-I between the number of MetS criteria and pro and inti-inflammatory mark- ers, in a large cohort studies may provide a better assessment for CVD. In addition, a prospective and well-controlled study would be needed to elucidate the associations of Apo B/Apo A-I ratio with diabetes and CVD risk. Similarly, prospective follow-up studies are required to evaluate medical interventions and lipid goal attainment in relation to mortality in diabetes pa- tients with MetS.
Authors Contribution
Hari Sharan Makaju, Vijay Kumar Sharma, Binod Kumar Ya- dav, Eans Tara Tuladhar and Roshan Bhandari conceived the design of the study.
Hari Sharan Makaju, Aseem Bhattarai, Anant Neupane and Ra- bina Ramtel performed the acquisition of data.
Hari Sharan Makaju, Binod Kumar Yadav, Vijay Kumar Shar- ma, Aseem Bhattarai and Eans Tara Tuladhar analyzed and in- terpreted the data.
Hari Sharan Makaju, Rabina Ramtel, Alisha Sapkota, Anant Neupane, Raju Kumar Dubey and Aapekshya Niraula Drafted the manuscript.
Hari Sharan Makaju, Vijay Kumar Sharma, Mithileshwor Raut, Aseem Bhattarai and Roshan Bhandari performed the critical re- vision for important intellectual content.
All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibili- ty for its accuracy and integrity.
Acknowledgement
We thank all the volunteers participating in this study. Our spe- cial thanks go to all the faculty members and laboratory staff of department of Clinical Biochemistry, Tribhuvan University Teaching Hospital Kathmandu for supporting and Nepal Health Research Council (NHRC) for providing PG Thesis Grant to ac- complish this study.
Funding Statement
The study has been partially financial support was done by NHRC as a PG thesis grant.
Approval of the Study
This study has been approved for Master’s level thesis by De- partment of Biochemistry, Institute of Medicine
Ethical Approval
The study has given ethical clearance by the institutional review committee, Institute of Medicine and the letter has been submit- ted along with the manuscript submission.
References
- Gyawali, B., Sharma, R., Neupane, D., Mishra, S. R., van Teijlingen, E., & Kallestrup, P. (2015). Prevalence of type 2 diabetes in Nepal: a systematic review and meta-analysis from 2000 to 2014. Global health action, 8(1), 29088.
- World Health Organization. (2017). Global diffusion of eHealth: making universal health coverage achievable: re- port of the third global survey on eHealth. World Health Organization.
- Cho, N. H., Shaw, J. E., Karuranga, S., Huang, Y., da Ro- cha Fernandes, J. D., Ohlrogge, A. W., & Malanda, B. I. D.F. (2018). IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes re- search and clinical practice, 138, 271-281.
- Morrish, N. J., Wang, S. L., Stevens, L. K., Fuller, J. H., Keen, H., & WHO Multinational Study Group. (2001). Mortality and causes of death in the WHO Multinational Study of Vascular Disease in Diabetes. Diabetologia, 44,S14-S21.
- DeFronzo, R. A. (2009). From the triumvirate to the omi- nous octet: a new paradigm for the treatment of type 2 dia- betes mellitus. Diabetes, 58(4), 773-795.
- DeFronzo, R. A. (2010). Insulin resistance, lipotoxicity, type 2 diabetes and atherosclerosis: the missing links. The Claude Bernard Lecture 2009. Diabetologia, 53(7), 1270-1287.
- Nobécourt, E., Tabet, F., Lambert, G., Puranik, R., Bao, S., Yan, L., ... & Rye, K. A. (2010). Nonenzymatic glycation impairs the antiinflammatory properties of apolipoprotein AI. Arteriosclerosis, thrombosis, and vascular biology, 30(4), 766-772.
- Marcovina, S., & Packard, C. J. (2006). Measurement and meaning of apolipoprotein AI and apolipoprotein B plasma levels. Journal of internal medicine, 259(5), 437-446.
- Lima, L. M., Carvalho, M. D. G., & Sousa, M. O. (2007). Apo B/apo AI ratio and cardiovascular risk prediction. Ar- quivos brasileiros de cardiologia, 88, e187-e190.
- Kaneva, A. M., Potolitsyna, N. N., Bojko, E. R., & Odland,J. Ø. (2015). The apolipoprotein B/apolipoprotein AI ra- tio as a potential marker of plasma atherogenicity. Disease markers, 2015.
- Lu, M., Lu, Q., Zhang, Y., & Tian, G. (2011). ApoB/apoA1 is an effective predictor of coronary heart disease risk in overweight and obesity. Journal of biomedical research, 25(4), 266-273.
- Zhong, L., Li, Q., Jiang, Y., Cheng, D., Liu, Z., Wang, B.,... & Qing, H. (2010). The ApoB/ApoA1 ratio is associated with metabolic syndrome and its components in a Chinese population. Inflammation, 33, 353-358.
- Sierra-Johnson, J., Romero-Corral, A., Somers, V. K., Lo- pez-Jimenez, F., Walldius, G., Hamsten, A., ... & Fisher, R.M. (2007). ApoB/apoA-I ratio: an independent predictor of insulin resistance in US non-diabetic subjects. European heart journal, 28(21), 2637-2643.
- Mancia, G., De Backer, G., Dominiczak, A., Fagard, R., Germano, G., Grassi, G., ... & Williams, B. (2007). 2007 ESH-ESC guidelines for the management of arterial hyper- tension-The task force for the management of arterial hy- pertension of the European society of hypertension (ESH) and of the European society of cardiology (ESC). Blood pressure, 16(3), 135-232.
- Shaw, J. E., Sicree, R. A., & Zimmet, P. Z. (2010). Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes research and clinical practice, 87(1), 4-14.
- Rojas, E., Castro, A., Manzano, A., Suárez, M. K., Lameda, V., Carrasquero, R., ... & Bermúdez, V. (2020). Diagnostic criteria and management of metabolic syndrome: Evolution overtime. Gaceta Médica de Caracas, 128(4), 480-504.
- Hachem, S. B., & Mooradian, A. D. (2006). Familial dyslip- idaemias. Drugs, 66(15), 1949-1969.
- Jialal, I., & Singh, G. (2019). Management of diabetic dys- lipidemia: An update. World journal of diabetes, 10(5), 280.
- Wu, L., & Parhofer, K. G. (2014). Diabetic dyslipidemia. Metabolism, 63(12), 1469-1479.
- Goldberg, I. J. (2001). Diabetic dyslipidemia: causes and consequences. The journal of clinical endocrinology & me- tabolism, 86(3), 965-971.
- Gao, L., Zhang, Y., Wang, X., & Dong, H. (2021). Associ- ation of apolipoproteins A1 and B with type 2 diabetes and fasting blood glucose: a cross-sectional study. BMC endo- crine disorders, 21, 1-11.
- Jun, J. E., Choi, Y. J., Lee, Y. H., Kim, D. J., Park, S. W.,Huh, B. W., ... & Huh, K. B. (2018). ApoB/ApoA-I ratio is independently associated with carotid atherosclerosis in type 2 diabetes mellitus with well-controlled LDL choles- terol levels. The Korean journal of internal medicine, 33(1), 138.
- Walldius, G., Jungner, I., Holme, I., Aastveit, A. H., Ko- lar, W., & Steiner, E. (2001). High apolipoprotein B, low apolipoprotein AI, and improvement in the prediction of fatal myocardial infarction (AMORIS study): a prospective study. The Lancet, 358(9298), 2026-2033.
- Kumar, S., Sharma, N., Bhandiwad, C., Singh, C. P., Sin- ghal, V., & Chakranarayan, A. (2019). A Study of Correla- tion between Apolipoprotein B and Dyslipidemia in Type 2 Diabetes Patients and its Relation with Proteinuria-A Tertia- ry Care Hospital Based Study. The Journal of the Associa- tion of Physicians of India, 67(7), 30-33.
- Katulanda, G. W., Katulanda, P., Adler, A. I., Peiris, S. R., Draisey, I., Wijeratne, S., ... & Shine, B. (2010). Apolipo- proteins in diabetes dyslipidaemia in South Asians with young adult-onset diabetes: distribution, associations and patterns. Annals of clinical biochemistry, 47(1), 29-34.
- Adaja, T. M., Ojo, M. A. O., & Ayina, C. N. A. (2019). Rela-tionship of Apolipoprotein B-100 and Lipid Profile Param- eters among Diabetic Patients in a Tertiary Hospital in Ni- geria. Current Trends in Disease and Health Vol. 2, 75-84.
- Jiang, R., Schulze, M. B., Li, T., Rifai, N., Stampfer, M. J., Rimm, E. B., & Hu, F. B. (2004). Non-HDL cholesterol and apolipoprotein B predict cardiovascular disease events among men with type 2 diabetes. Diabetes care, 27(8), 1991-1997.
- Sahadevan, D. C., Singh, A., Karunanand, B., Thakkar, H., & Gautam, A. K. (2020). APO B/APO A1 Ratio and its Cor- relation with Cardiometabolic Risk Factors and Oxidative Stress in Subjects with Metabolic Syndrome. International Journal of Scientific Research, 9(2).
- Wallenfeldt, K., Bokemark, L., Wikstrand, J., Hulthe, J., & Fagerberg, B. (2004). Apolipoprotein B/apolipoprotein AI in relation to the metabolic syndrome and change in carotid artery intima-media thickness during 3 years in middle-aged men. Stroke, 35(10), 2248-2252.
- McQueen, M. J., Hawken, S., Wang, X., Ounpuu, S., Snid-erman, A., Probstfield, J., ... & Yusuf, S. (2008). Lipids, li- poproteins, and apolipoproteins as risk markers of myocar- dial infarction in 52 countries (the INTERHEART study): a case-control study. The lancet, 372(9634), 224-233.
- Assessment, R. E. L. I. A. B. L. E. (2009). Major lipids, apo- lipoproteins, and risk of vascular disease. Jama, 302(18), 1993-2000.
- Sierra-Johnson, J., Fisher, R. M., Romero-Corral, A., Somers, V. K., Lopez-Jimenez, F., Öhrvik, J., ... & Hamsten,A. (2009). Concentration of apolipoprotein B is comparablewith the apolipoprotein B/apolipoprotein AI ratio and better than routine clinical lipid measurements in predicting cor- onary heart disease mortality: findings from a multi-ethnic US population. European heart journal, 30(6), 710-717.
- Schianca, G. C., Pedrazzoli, R., Onolfo, S., Colli, E., Cor- netti, E., Bergamasco, L., ... & Bartoli, E. (2011). ApoB/ apoA-I ratio is better than LDL-C in detecting cardiovascu- lar risk. Nutrition, Metabolism and Cardiovascular Diseas- es, 21(6), 406-411.
- Belfki, H., Ali, S. B., Bougatef, S., Ahmed, D. B., Haddad,N., Jmal, A., ... & Romdhane, H. B. (2011). The Apolipo- protein B/Apolipoprotein A 1 ratio in relation to metabolic syndrome and its components in a sample of the Tunisian population. Experimental and molecular pathology, 91(2), 622-625.
- Jing, F., Mao, Y., Guo, J., Zhang, Z., Li, Y., Ye, Z., ... &Chen, K. (2014). The value of Apolipoprotein B/Apoli- poprotein A1 ratio for metabolic syndrome diagnosis in a Chinese population: a cross-sectional study. Lipids in health and disease, 13(1), 1-7.
- Jung, C. H., Hwang, J. Y., Yu, J. H., Shin, M. S., Bae, S. J.,Park, J. Y., ... & Lee, W. J. (2012). The value of apolipopro- tein B/A1 ratio in the diagnosis of metabolic syndrome in a Korean population. Clinical endocrinology, 77(5), 699-706.
- Schmidt, C., Fagerberg, B., Wikstrand, J., & Hulthe, J. (2006). apoB/apoA–I ratio is related to femoral artery plaques and is predictive for future cardiovascular events in healthy men. Atherosclerosis, 189(1), 178-185.
- Walldius, G., Jungner, I., Aastveit, A. H., Holme, I., Furb- erg, C. D., & Sniderman, A. D. (2004). The apoB/apoA-I ratio is better than the cholesterol ratios to estimate the bal- ance between plasma proatherogenic and antiatherogenic li- poproteins and to predict coronary risk. Clinical Chemistry and Laboratory Medicine (CCLM), 42(12), 1355-1363.
- Canouï-Poitrine, F., Luc, G., Bard, J. M., Ferrieres, J., Yar- nell, J., Arveiler, D., ... & Empana, J. P. (2010). Relative contribution of lipids and apolipoproteins to incident coro- nary heart disease and ischemic stroke: the PRIME Study. Cerebrovascular Diseases, 30(3), 252-259.
- Pitsavos, C., Panagiotakos, D. B., Skoumas, J., Papadim- itriou, L., & Stefanadis, C. (2008). Risk stratification of apolipoprotein B, apolipoprotein A1, and apolipoprotein B/ AI ratio on the prevalence of the metabolic syndrome: the ATTICA study. Angiology, 59(3), 335-341.
- Yusuf, S., Hawken, S., Ôunpuu, S., Dans, T., Avezum, A., Lanas, F., ... & Lisheng, L. (2004). Effect of potentially modifiable risk factors associated with myocardial infarc- tion in 52 countries (the INTERHEART study): case-con- trol study. The lancet, 364(9438), 937-952.
- Patel, V. I., Patel, K. P., Makadia, M. G., Shah, A. D., Chaud- hari, K. S., & Nilayangode, H. N. (2017). Levels of apoli- poprotein A1, B100 and lipoprotein (a) in controlled and uncontrolled diabetic patients and in non-diabetic healthy people. Journal of clinical and diagnostic research: JCDR, 11(2), BC01.
- American Diabetes Association. (2010). Standards of medi- cal care in diabetes—2010. Diabetes care, 33(Suppl 1), S11.
- American Association of Clinical Endocrinologists. (2007).State of diabetes complications in America. Jacksonville, Fla., American Association of Clinical Endocrinologists.
- Walldius, G., & Jungner, I. (2006). The apoB/apo-I ratio: a strong, new risk factor for cardiovascular disease and a target for lipid-lowering therapy–a review of the evidence. Journal of internal medicine, 259(5), 493-519.
- Tietz, N. (1987). Fundamentals of Clinical Chemistry 3rd ed, 544.
- Tamang, H. K., Timilsina, U., Singh, K. P., Shrestha, S.,Raman, R. K., Panta, P., ... & Dahal, C. (2014). Apo B/Apo AI ratio is statistically a better predictor of cardiovascular disease (CVD) than conventional lipid profile: a study from Kathmandu Valley, Nepal. Journal of clinical and diagnos- tic research: JCDR, 8(2), 34.
- Shilpasree, A. S., Sahukar, S., Murthy, J., & Kumar, K. (2013). A study of serum apolipoprotein A1, apolipoprotein B and lipid profile in stroke. Journal of clinical and diagnos- tic research: JCDR, 7(7), 1303.