




Research Article - (2024) Volume 3, Issue 3
Assessment of Incidence and Associated Risk Factors of Awareness with Recall Under General Anesthesia in Non-Cardiac and Non-Obstetric Patients in Tikur Anbessa Specialized Hospital, Addis Ababa From May 2021 to October 2021, Addis Ababa, Ethiopia
Received Date: Sep 11, 2024 / Accepted Date: Dec 02, 2024 / Published Date: Dec 12, 2024
Copyright: ©Â©2024 Zemed Geleta Eshete, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Eshete, Z. G., Denberu, Y. D., Endris, S., Hulala, F. (2024). Assessment of Incidence and Associated Risk Factors of Awareness with Recall Under General Anesthesia in Non-Cardiac and Non-Obstetric Patients in Tikur Anbessa Specialized Hospital, Addis Ababa From May 2021 to October 2021, Addis Ababa, Ethiopia. J Surg Care, 3(3), 01-10.
Abstract
Introduction General anesthesia involves administering drugs to induce hypnosis, amnesia, and stress suppression during surgery. Anesthesia awareness, an unintended event where patients recall experiences during anesthesia, can lead to long-term psychological effects.
Objective This study evaluated the incidence and risk factors associated with awareness under general anesthesia among non-cardiac and non-obstetric patients at Tikur Anbesa Specialized Hospital (TASH), Addis Ababa, Ethiopia, from May to October 2021.
Methodology A prospective cross-sectional study was conducted at TASH using the modified Brice questionnaire and Aldrete score to assess intra-operative awareness and wakefulness. Systematic random sampling was used to select patients assessed in the Post- Anesthesia Care Unit (PACU) and ward. Data were analyzed using SPSS version 25, and logistic regression was used to determine variable associations (p < 0.05).
Results The study included 354 patients (response rate: 96.4%); 58.7% were male, and 41.5% were female, with a mean age of 39.3 years. The incidence of awareness with recall was 11.7%, while dreaming occurred in 9.1% of patients. Awareness was significantly associated with muscle relaxants (OR 2.793, 95% CI 1.872-1.948, p = 0.003). Dreaming was more common in females.
Conclusions The incidence of awareness was higher than in many global studies, with consistent risk factors, particularly the use of muscle relaxants. Dreaming was more common among females.
Recommendations Anesthesia providers should monitor intra-operative awareness, manage muscle relaxant dosages, and maintain anesthesia equipment, including gas and depth monitors
Introduction
Background
General anesthesia is the complex process of administering drugs to induce hypnosis, amnesia, and suppression of stress response to surgical stimuli and create a quiet surgical field. However, it is difficult to define the depth of anesthesia, especially in developing countries where invasive monitors are limited the main aim of anesthesia is to alleviate patients from stress/anxiety and pain, and maintain the physiologic state. However, depending on the intensity of surgical stimulation and different patient pathophysiology, there will be an imbalance between drug requirement and drug administration, which results in a variable depth of anesthesia. When a patient has been given less than the desired dose of a drug, the patient will develop intraoperative awareness the ability of memorizing or recalling events during a surgical procedure [1,2]. Awareness is one of the rare but potentially disastrous complications of surgery and anesthesia. It is characterized by explicit memorizing of events happening during anesthesia. Remembering of events of anesthesia and surgery are a common concern raised by most patients before undergoing anesthesia Awareness was recognized since the nineteenth century when the first general anesthesia with ether was started for tooth extractions after Gilbert Abbot remembered all events without postoperative pain [3,4]. Patients with awareness may experience different adverse events including nightmares, sleepiness, insomnia, anxiety, and even post-traumatic stress disorders (PTSD) [5-8].
The awareness causes are not identified and it is multi-factorial. However, patient requirement for light anesthesia, increased anesthetic requirement, and machine malfunction or misuse resulting in an inadequate delivery of anesthesia, are among the commonest causes incriminated. It can also be classified according to their source like patient related, surgery-related related and anesthesia-related [9-11]. Sometimes, it is not uncommon for doctors and nurses to hear patients complaining about their experience to their close family and friends after surgery. The patient may feel pain, hear the sound of falling instruments, be unable to move extremities and feel anxiety during anesthesia. Intraoperative awareness is one of the perioperative adverse events that are neglected by anesthesia providers and surgeons during operations, particularly in low-resource settings. Though the magnitude of intraoperative awareness is low in the westerns, the incidence in the developing countries was higher and ranged from 1.07-13.3% [8,12-16]. In addition, no study deals on the impact of awareness, and the effects of anesthesia type on awareness, even on high-risk surgeries such as cesarean delivery and cardiac surgery.
The effect of perioperative awareness following anesthesia is a concerning issue for the patient and it may result in the development of post-operative insomnia, anxiety, nightmare post-traumatic stress disorder, and other chronic psychological sequelae [6,7]. Only one study in Ethiopia studies the magnitude and associated risk factors of awareness with recall [15]. Intra- operative anesthesia awareness is almost neglected in low-income countries, particularly in Africa. There was no similar study done in Addis Ababa so this study aimed to answer the questions about the incidence of awareness with recall under general anesthesia (GA), and its associated risk factors. Even though the incidence and impact of awareness are high in low-income countries, particularly in Africa, low attention has been given by both anesthesia providers and surgeons. There were very few studies conducted so far. Therefore, the result of this study will fill the information gap on the magnitude of intra-operative awareness and associated risk factors. The result of this study will also help to improve patient care during the perioperative period and possible guideline development. It will also serve as a baseline reference for future studies in the study areas. Finally, recommendations will be given for respective stakeholders to act accordingly.
Methods
Study Area and Period
The study was conducted at Tikur Anbesa Specialized Hospital (TASH) in Addis Ababa, Ethiopia's capital. As one of the largest hospitals in the country, TASH provides a range of surgical services across various departments, including Neurosurgery, Cardio-Thoracic Surgery, Pediatric Surgery, Urological Surgery, ENT, Orthopedic Surgery, Gastrointestinal Tract Surgery, and Obstetrics and Gynecology. Anesthesia services are managed by the Department of Anesthesiology, Critical Care, and Pain Medicine. The study was conducted from May to October 2021. TASH was selected due to its high case volume, variety of surgical procedures, and extensive range of cases.
Study Design
An institutional-based prospective cross-sectional study.
Inclusion Criteria
All adult patients above 18 years of age with normal mental status who had undergone general anesthesia during the study period at TASH were included.
Exclusion Criteria
Patients not ex-intubated after surgery, patients undergoing conscious sedation, and patients who refused to participate were excluded.
Sample Size and Sampling
Technique A sample size of 354 was determined using a single population proportion formula with a systematic random sampling technique.
Data Collection
Data were collected using structured questionnaires on demographics, patient, anesthesia, and surgery-related variables. The Brice questionnaire, translated to Amharic, and the Aldrete score were used.
Variables
Dependent
Awareness with recall.
Independent
Patient-related factors (e.g., age, sex), surgery-related factors (e.g., type of surgery), anesthesia-related factors (e.g., drug use).
Data Quality Assurance
Structured questionnaires, pre-tests, training, and supervision ensured data quality.
Data Analysis
Data were entered into SPSS version 25, cleaned, and analyzed using logistic regression to determine associations (significance at p < 0.05).
Ethical Considerations
Ethical clearance was obtained, and informed consent was taken from participants.
Dissemination of Results
Findings will be presented to the Department of Anesthesiology, with efforts made to publish in a scientific journal.
Results
Socio-Demographic Characteristics
The study population included 354 patients, who underwent surgery under general anesthesia during the study period from May to September 2021. Among these 13 patients were excluded due to incomplete data. Male 200 (58.7%) participants were greater than female 141 (41.3%). The minimum and maximum ages of the respondents were 19 and 89 with a mean of 39.3+ 15.2 (SD).
Figure 1: Sex Distribution of a Study Participant in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2021
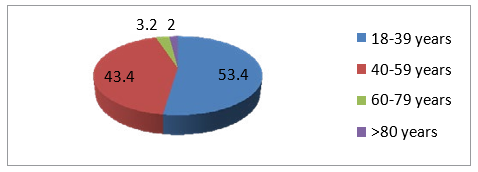
Figure 2: Age Distribution of a Study Participant in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2021
Risk Factors
In this study majority of patients were ASA I 176 (51.6%), and the rest were ASA II 137 (40.2%), ASA III 20 (5.9%), and ASA IV 8 (2.3%). Among the respondents, 99 (29) were found to have a chronic illness, 57 (16.7%) were taking alcohol, 16 (4.7) patients were smokers, 19 (5.6%) had a history of chronic pain and three patients had a history of awareness in previous surgeries.
|
Variables |
|
Frequency |
Percent |
|
ASA status |
ASA I |
176 |
51.6 |
|
|
ASA II |
137 |
40.2 |
|
|
ASA III |
20 |
5.9 |
|
|
ASA IV |
8 |
2.3 |
|
Alcohol |
Yes No |
57 284 |
16.7 83.3 |
|
Smoking |
Yes |
16 |
4.7 |
|
|
No |
325 |
95.3 |
|
Chronic pain |
Yes No |
19 322 |
5.6 94.4 |
|
Medical illness |
Yes No |
99 242 |
29 71 |
|
Previous history of awareness |
Yes No |
3 339 |
0.9 99.1 |
Table 1: Frequency and Percentage of Risk Factors in The Study Participants in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2021(N=341)
Anesthesia-Related Factors and Surgical Procedures
Both normal (218, 63.9%) and modified rapid sequence induction (RSI) (123, 36.1%) were used during intubation. Thiopental 176 (51.6%), propofol 143 (41.9%), ketamine 9 (2.6%), and ketofol 8 (2.3%) were used as induction of anesthesia. Volatile anesthetics (halothane 87.7%), and isoflurane 12.3%) were used as a maintenance of anesthesia and supplemented with opioids (morphine 71.8%, fentanyl 15.8%, and pethidine 10.9%). Of the patients, 16.1% were received premedication, usually dexamethasone (3.2%), followed by diazepam (2.6%), metoclopramide (2.1%), and lidocaine (1.8). Muscle relaxants (78.3%) were used for both induction and maintenance in 276 (78.3%) of patients. Different adjuvant drugs, like lidocaine 25 (7.3%), dexamethasone 17 (5.0%), Mgso4 14 (4.1%), fentanyl 7 (2.1%), diazepam 5 (1.5%), and paracetamol 5 (1.5%), were used. Most of the respondents were elective 231 (67.7%) while the rest 110 (32.3%) were emergency.
|
Procedures |
Elective |
|
Emergence |
|
Total |
|
|
Frequency |
Percent |
Frequency |
Percent |
|
|
|
|
|
|
||
|
Neurosurgery |
34 |
14.4 |
12 |
11.4 |
46 |
|
Thoracic surgery |
33 |
14.0 |
4 |
3.8 |
37 |
|
ENT surgery |
25 |
10.6 |
|
|
25 |
|
Endocrine surgery |
10 |
4.2 |
|
|
10 |
|
Abdominal surgery |
50 |
21.3 |
34 |
32.4 |
84 |
|
Gynecologic surgery |
18 |
7.6 |
11 |
10.5 |
29 |
|
Urology surgery |
29 |
12.3 |
4 |
3.8 |
33 |
|
Orthopedics surgery |
23 |
9.7 |
17 |
16.2 |
40 |
|
Vascular surgery |
14 |
5.9 |
16 |
15.2 |
30 |
|
Trauma surgery |
|
|
7 |
6.7 |
7 |
|
Total |
236 |
100 |
105 |
1oo |
341 |
Table 2: Frequency and Percentage of Surgical Procedures Performed in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2021(N=341)
Prevalence of Awareness
Among 341 respondents, 278 (81.5%) were assuming that the surgery was done under complete sleeping conditions; whereas 63 (18.5%) were not.
|
Variables |
Frequency |
Percent (%) |
|
The last thing the patient remember |
|
|
|
Feeling mask on face |
84 |
24.6 |
|
Being with family |
74 |
21.7 |
|
Being in the pre-op area |
57 |
16.7 |
|
Seeing the operating room |
54 |
15.8 |
|
Burning or stinging in the IV line |
27 |
7.9 |
|
Hearing voices |
25 |
7.3 |
|
Smell of gas |
16 |
4.7 |
|
The first thing you remember after waking up |
|
|
|
Hearing of voice |
143 |
41.9 |
|
Nothing |
47 |
13.8 |
|
Feeling breathing tube |
42 |
12.3 |
|
Feeling mask on the face |
32 |
9.4 |
|
Feeling pain |
30 |
8.8 |
|
Being in the recovery room |
19 |
5.6 |
|
Seeing the operating room |
14 |
4.1 |
|
Being with family |
14 |
4.1 |
|
Total |
341 |
100 |
Table 3: Frequency and Percentage of The Last Thing Patients Remember and The First Thing Remember After Waking Up Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2021(N=341)
Forty cases (11.7%) were identified with awareness and 33 (9.7%) patients reported dreaming. Among 40 cases who had awareness, 70% had auditory perception, 10% experienced anxiety/stress, 10 % felt pain, 5% sensed surgical events, and the remaining experienced unable to move or breathe and sensation of the breathing tube. Most patients claimed pain 141 (41.3%) and anxiety122 (35.8%) as their worst experience during operations. Among patients with dreaming, 8 patients experienced horrifying sounds and events while others reported being with family, going to the toilet, being bitten by ants, collecting crops from the farm area, being surrounded by old people, and 4 patients with unspecified dreams.
|
Events |
|
Frequency |
Percentage |
|
Nothing |
|
301 |
88.3 |
|
Hearing voices |
|
28 |
8.2 |
|
Sensing surgical events |
|
2 |
0.6 |
|
Unable to move or breath |
|
1 |
0.3 |
|
Anxiety or stress |
|
4 |
1.2 |
|
Feeling pain |
|
4 |
1.2 |
|
Sensation of breathing tube |
|
1 |
0.3 |
|
Dreaming |
Yes |
33 |
9.7 |
|
|
No |
308 |
90.3 |
|
Worst thing about the operation |
Anxiety |
122 |
35.8 |
|
|
Pain |
141 |
41.3 |
|
Recovery process |
21 |
6.15 |
|
|
Unable to carry |
12 |
3.52 |
|
|
out usual activities |
|
|
|
|
Others |
45 |
13.23 |
Table 4: Frequency and Percentage of Intra-Operative Events Reported Among Patients Who Had Awareness with Recall Under General Anesthesia in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2021(N=341)
Factors Associated with Awareness
Binary logistic regression was performed to assess the association of each independent variable with the dependent variable and the factors that showed a p-value of 0.25 and less were added to multivariate regression model to detect the statistically significance variable. On binary logistic regression, factors such as ASA status, history of chronic pain, use of premedication, use of muscle relaxant, smoking history, and orthopedics surgery were entered to multivariate analysis. On multi-variant logistic regression only uses of muscle relaxants and history of chronic pain were significantly associated. Other variables like age, sex, history of previous awareness, alcohol intake, smoking, premedication use, type of surgery, type of operation, use of inhalations, and opioids did not have a statistically significant association on this study. Awareness was associated with the use of muscle relaxant (OR2.793 (1.872-1.948), p-value 0.003). Patient with muscle relaxant were 2.8 times higher chance of developing awareness when compared to non-relaxed patients. Dreaming was associated with a female gender (OR 2.375, CI 1.038-5.433, and P value 0.036) in this study.
|
Variables |
Frequency (%) |
Bi-variant |
|
Multivariate |
|
|
Age |
|
Crude OR |
P value |
Adjusted OR |
Pvalue |
|
18-39 |
177(51.9) |
0.510 (0.051- |
0.568 |
1.447(0.177-11.83) |
0.731 |
|
40-59 |
148 (43.4) |
5,142) |
0.957 |
1.212(0.145-10.09) |
0.859 |
|
60-79 |
14(3.2) |
0.939 (0.095- |
|
|
|
|
>80 |
2 |
9.332) |
|
|
|
|
Sex |
|
|
|
|
|
|
Male |
200 (58.7) |
0.974(0.442- |
0.948 |
0.948(0.486-1.848) |
0.875 |
|
Female |
141(41.3) |
2.149) |
|
|
|
|
ASA status |
|
|
|
|
|
|
ASA I |
176(51.6) |
5.421(0.62447.61 |
0.125 |
0.3(0.056-1.611) |
0.160 |
|
ASA II |
137(40.2) |
7) |
0.390 |
0.454(0.085-2.423) |
0.333 |
|
ASA III |
20(5.9) |
2.391(0.327- |
0.957 |
0.750(0.108-5.216) |
0.771 |
|
ASA IV |
8(2.3) |
17.485) |
|
|
|
|
|
|
0.941(0.107- |
|
|
|
|
|
|
8.272) |
|
|
|
|
Alcohol |
|
|
|
|
|
|
Yes |
57(16.7) |
0.710(0.275- |
0.479 |
1.286(0.559-2.957) |
0.554 |
|
No |
284(83.3) |
1.833) |
|
|
|
|
Smoking |
|
|
|
|
|
|
Yes |
16(4.7) |
0.481(0.133- |
0.265 |
2.676(0.819-8.738) |
0.103 |
|
No |
325(95.3) |
1.745) |
|
|
|
|
chronic pain |
|
|
|
|
|
|
Yes |
19(5.6) |
0.349(0.098- |
0.105 |
2.929(0.995-8.621) |
0.042 |
|
No |
322(94.4) |
1.248) |
|
|
|
|
Premedication |
|
|
|
|
|
|
Yes |
55(16.1) |
0.673(0.260- |
0.415 |
1.351(0.586-3.114) |
0.480 |
|
No |
286(83.9) |
1.743) |
|
|
|
|
Difficult |
|
|
|
|
|
|
intubation |
2(0.6) |
0.317(0.071- |
0.131 |
2.359(0.621-8.964) |
0.207 |
|
Yes |
339(99.4) |
1.407) |
|
|
|
|
No |
|
|
|
|
|
|
Muscle relaxant |
|
|
|
|
|
|
Yes |
267(78.3) |
3.447(1.517- |
0.003 |
2.793(1.872-1.948) |
0.003 |
|
No |
74(21.7) |
7.831) |
|
|
|
|
Urgency of |
|
|
|
|
|
|
surgery |
105(30.8) |
1.680(0.645- |
0.288 |
0.835(0.400-1.743) |
0.835 |
|
Emergency |
236(69.2) |
4.375) |
|
|
|
|
Elective |
|
|
|
|
|
|
Type of |
|
|
|
|
|
|
operations |
46(13.5) |
0.356(0.037- |
0.374 |
5.026(0.585- |
0.141 |
|
Neurosurgery |
37(10.9) |
3.469) |
0.485 |
43.179) |
0.190 |
|
Thoracic |
25(7.3) |
0.438(0.043- |
0.882 |
4.375(0.482- |
0.479 |
|
ENT |
10(2.9) |
4.430) |
0.587 |
39.727) |
0.439 |
|
Endocrine |
84(24.6) |
0.818(0.059- |
0.576 |
2.435(0.207- |
0.307 |
|
Abdomen |
29(8.5) |
11.599) |
0.685 |
28.584) |
0.561 |
|
Gynecology |
33(9.4) |
0.433(0.021- |
0.560 |
3.111(.176-54.967) |
0.299 |
|
Urology |
40(11.7) |
8.892) |
0.168 |
3.027(0.362- |
0.094 |
|
Orthopedics |
30(9.1) |
0.533(0.059- |
0.220 |
25.316) |
0.145 |
|
Vascular |
7(2.1) |
4.816) |
|
2.074(0.178- |
|
|
Trauma |
|
0.587(0.045- |
|
24.228) |
|
|
|
|
7.677) |
|
4.667(0.255- |
|
|
|
|
0.391(0.017- |
|
85.551) |
|
|
|
|
9.169) |
|
6.222(0.734- |
|
|
|
|
0.208(0.022- |
|
52.712) |
|
|
|
|
1.936) |
|
5.185(0.568- |
|
|
|
|
0.234(0.023- |
|
47.321) |
|
|
|
|
2.384) |
|
|
|
Table 5: Bi-Variant and Multi-Variable Logistic Regression Among Patients Who Develop Awareness with Recall Under General Anesthesia in Tikur Anbessa Specialized Hospital Addis Ababa, Ethiopia, 2021 (N=341)
Discussions
Awareness during surgery is a rare but potentially devastating event that occurs in the perioperative period. This study examines the incidence of awareness and its associated risk factors through an institutional-based cross-sectional approach. The study found that the incidence of awareness with recall under general anesthesia was 11.7%. This rate is higher than that reported in most Western studies, which range from 0.0068% to 1% [17-21]. It also exceeds the rates observed in studies from Nigeria (4.6%), Brazil (2.5%), England (1.0%), India (0.78%), and Ethiopia (8.2% at Debre Tabor) [5,13,20,22]. However, it is lower than a study from Sudan, which reported an incidence of 13.3% [16]. The variation may be due to factors such as the lack of anesthesia depth monitoring, absence of anesthetic gas monitors, anesthesia techniques used, and inappropriate drug dosages.
The incidence of awareness was assessed using the Modified Brice questionnaire, which revealed that 70% of respondents reported hearing voices, 10% experienced anxiety or stress, 10% felt pain, 5% recalled hearing events during surgery, and some patients reported sensations such as the inability to move or breathe, or feeling the breathing tube. These findings align with other studies, such as those from the US, which showed 48% of patients with auditory perceptions, 36% with anxiety, and 28% with pain, and from China, which reported similar experiences [13,20]. Another Brazilian study reported auditory memories (48%), sensations of not breathing (48%), and pain (28%) [8]. A study from Debre Tabor, Ethiopia, also found comparable results, with 4.9% hearing voices, 2.6% feeling pain, and 1.8% experiencing anxiety and stress [15]. These studies suggest no significant differences in the signs and symptoms of awareness. Multivariate logistic regression analysis showed a significant association between the use of muscle relaxants and awareness (OR 2.793, 95% CI 1.872-1.948, p = 0.003). A meta-analysis by Nunes et al. found that 0.18% of patients receiving muscle relaxants developed awareness, highlighting the link between neuromuscular blocking agents and increased intra-operative awareness and implicit memory [10]. Additionally, a closed claims analysis by the American Society of Anesthesiologists identified muscle relaxants as a cause of awareness due to awake paralysis from labeling errors and incorrect drug administration in 18 out of 79 aware patients [21]. Silva and Squeff also demonstrated an association between awareness and the use of general anesthesia with muscle relaxants [8]. Hypnosis was achieved using volatile anesthetics or intravenous anesthesia, but factors such as low minimum alveolar concentration (MAC), lack of intravenous supplements, infrequent machine maintenance, and expired CO2 absorbent could contribute to awareness.
While many studies consider ASA physical status an independent risk factor for awareness, this study did not find a significant association. This discrepancy may be due to the small sample size or the low number of patients with higher ASA status in this study. In contrast, other studies have shown a positive correlation between awareness and higher ASA status, such as a study from China indicating a link with ASA III and IV status [20,23]. Factors like the type of surgery, difficult intubation, and previous awareness history were not associated with awareness in this study, potentially due to the limited sample size. However, bi-variant and multivariate analysis showed that dreaming was significantly associated with female sex (OR 2.375, CI 1.038-5.433, p = 0.036). The incidence of dreaming in this study (6%) aligns with a multi¬center US study but is slightly higher than another study reporting 3.3% [13,24,25]. Conversely, the incidence here was lower than in another US study that reported a 22% incidence of dreaming [21].
Conclusion
According to this study, the incidence of intraoperative awareness with recall under general anesthesia was 11.7%. Under the findings of this study, we conclude that the incidence of awareness with recall under general anesthesia is higher than in most global studies. However, the risk factors and symptoms of awareness were comparable with most literature. The use of muscle relaxants was identified as a risk factor in this study. When the incidence of dreaming was 9.3%, being female is a risk factor for dreaming.
Strengths and Limitations of The Study
Having a comparable finding of this study with most studies across the globe was one of the strengths of this study. Patients were interviewed a minimum of two times and the response rate was also good. It will also serve as a baseline for further studies in the future. The limitation of this study includes being done in a single center; low sample size, absence of anesthesia depth monitors, and lack of gas analyzer.
Recommendation
Awareness has a great impact on the patient's life and peri-operative satisfaction. So that the study has recommended the anesthesia provider give much emphasis on intra-operative awareness, be vigilant on the dosage of relaxants, hypnotics, and inhalational, prevention and pain management, follow the patient in the postoperative period, and check anesthesia equipment and machine every day for every patient. We also recommend to have anesthesia depth monitors and gases sensors to monitor inhalational anesthetics in the gases supply. Finally, the area also needs further multicenter studies to draw conclusion to the national level.
Acknowledgment
Above all, I would like to praise the almighty God who gave me patience and strength to overcome all the difficulties I faced in my journey in the past years. I would like to thank Addis Ababa University College of Health Science, Department of Anesthesiology, critical care and pain medicine for giving me this golden opportunity to do this research. My gratitude also goes to my advisors Dr. Semira E. and Dr. Faiza H., and all my teachers for giving me the knowledge, skills, and experience during my residency training. Finally, I would like to thank Dr. Yidersal Demsie for his invaluable contribution for the success of my thesis.
References
- Heggy, E. R., Abbas, S. M., Abd El Mawla, A. G., Adolf, M., & Fetouh, A. (2020). Intraoperative awareness during general anesthesia: Experience in 200 patients in “185’s hospital for emergency surgeries and burn”.(an observational questionnaire-based study). Open Access Macedonian Journal of Medical Sciences, 8(B), 429-434.
- Khan, M. F., Samad, K., Shamim, F., & Ullah, H. (2008). Awareness during anesthesia--an update. Middle East Journal of Anesthesiology, 19(4), 723.
- Deis, A. S., Schnetz, M. P., Ibinson, J. W., & Vogt, K. M. (2020). Retrospective analysis of cases of intraoperative awareness in a large multi-hospital health system reported in the early postoperative period. BMC anesthesiology, 20, 1-7.
- Hutter, C., & Tomlin, P. J. (1978). Awareness during anaesthesia. British Journal of Anaesthesia, 50(3), 307a-307a.
- Tamire, T., Demelash, H., Yetneberk, T., & Kibret, S. (2019). Magnitude and associated factors of awareness with recall under general anesthesia in Amhara regional state referral hospitals, 2018. Anesthesiology Research and Practice, 2019(1), 7043279.
- Lee, J., Park, C., & Kim, S. (2019). Awareness during general anesthesia despite simultaneous bispectral index and end-tidal anesthetic gas concentration monitoring. Yeungnam University Journal of Medicine, 36(1), 50-53.
- Bischoff, P., & Rundshagen, I. (2011). MEDIZIN— Übersichtsarbeit: Unerwünschte Wachheit während der Narkose. Deutsches Arzteblatt-Arztliche Mitteilungen-Ausgabe B, 108(1).
- Silva, D., & Squeff, N. (2014). Awareness brazil-incidence of intraoperative awakening in a prospective study of 1259 cases. Journal of Anesthesia and Critical Care: Open Access, 1, 00019.
- Ghoneim, M. (2009). Etiology and risk factors of intraoperative awareness. Consciousness, awareness, and anesthesia, 90-113.
- Nunes, R. R., Porto, V. C., Miranda, V. T., Andrade, N. Q. D., & Carneiro, L. M. M. (2012). Risk factor for intraoperative awareness. Revista brasileira de anestesiologia, 62, 369-374.
- Ghoneim, M. M. (2007). Incidence of and risk factors for awareness during anaesthesia. Best Practice & Research Clinical Anaesthesiology, 21(3), 327-343.
- Sebel, P. S., Bowdle, T. A., Ghoneim, M. M., Rampil, I.J., Padilla, R. E., Gan, T. J., & Domino, K. B. (2004). The incidence of awareness during anesthesia: a multicenter United States study. Anesthesia & Analgesia, 99(3), 833-839.
- Ugwu, E. O. (2012). Awareness Under General Anaesthesia: Incidence, Risk Factors And Causes In Nigerian Patients. Faculty of Anaesthesia.
- Mohummed, A. A. B., & Mohammed, N. M. (2017). Incidence the, Intraoperative of, wad rin. Estimation of the Incidence of Intraoperative Awareness and Recall in Wad. (101671502):18–23.
- Mashour, G. A., Kent, C., Picton, P., Ramachandran, S. K.,Tremper, K. K., Turner, C. R., ... & Avidan, M. S. (2013). Assessment of intraoperative awareness with explicit recall: a comparison of 2 methods. Survey of Anesthesiology, 57(4), 192-193.
- Lekprasert, V., Frost, E. A., & Pausawasdi, S. (2008). Intraoperative awareness: major factor or non-existent. Middle East J. Anesthesiol, 19, 1201-1218.
- Pollard, R. J., Coyle, J. P., Gilbert, R. L., & Beck, J. E. (2007). Intraoperative awareness in a regional medical system: a review of 3 years’ data. The Journal of the American Society of Anesthesiologists, 106(2), 269-274.
- Xu, L., Wu, A. S., & Yue, Y. (2009). The incidence of intraoperative awareness during general anesthesia in China: a multiâ?center observational study. Acta Anaesthesiologica Scandinavica, 53(7), 873-882.
- Errando, C. L., Sigl, J. C., Robles, M., Calabuig, E., García, J., Arocas, F., ... & García-Aguado, R. (2008). Awareness with recall during general anaesthesia: a prospective observational evaluation of 4001 patients. British journal of anaesthesia, 101(2), 178-185.
- Pandit, J. J., Cook, T. M., Jonker, W. R., & O'Sullivan, E. (2013). A national survey of anaesthetists (NAP5 Baseline) to estimate an annual incidence of accidental awareness during general anaesthesia in the UK. British journal of anaesthesia, 110(4), 501-509.
- Singla, D., & Mangla, M. (2017). Incidence of awareness with recall under general anesthesia in rural India: an observational study. Anesthesia Essays and Researches, 11(2), 489-494.
- Ranta, S. O. V., Laurila, R., Saario, J., Ali-Melkkila, T., & Hynynen, M. (1998). Awareness with recall during general anesthesia: incidence and risk factors. Anesthesia & Analgesia, 86(5), 1084-1089.
- Chung, H. S. (2014). Awareness and recall during general anesthesia. Korean Journal of Anesthesiology, 66(5), 339-345.
- Scott, D. L. (1972). Awareness during general anaesthesia.Canadian Anaesthetists’ Society Journal, 19, 173-183.
- Samuelsson, P. (2008). Awareness and dreaming during anaesthesia: Incidence and importance (Doctoral dissertation, Linköping University Electronic Press).