


Research Article - (2024) Volume 9, Issue 2
Assessment of Food Safety Knowledge, Attitude And Hygiene Practices Amongst Food Vendors on the University of Cape Coast Campus and It's Surrounding Communities
2Department of Technical and Vocational Education, College of Education, University of Cape Coast, Ghana
3Department of Technical and Vocational Education, College of Education, University of Cape Coast, Ghana
4Department of Biochemistry, University of Cape Coast, Ghana
Received Date: Feb 01, 2024 / Accepted Date: Mar 04, 2024 / Published Date: Mar 20, 2024
Copyright: ©©2024 Emmanuel Ankomah-Appiah, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Ankomah-Appiah, E., Elizabeth, K., Darko, S. O., Abrokwah, F. (2024), Assessment of Food Safety Knowledge, Atti-tude And Hygiene Practices Amongst Food Vendors on the University of Cape Coast Campus and It's Surrounding Communities. Adv Nutr Food Sci, 9(2), 01-09.
Abstract
The primary objective of this research was to evaluate the knowledge, attitudes, and hygiene practices related to food safety among vendors at the University of Cape Coast. A descriptive survey methodology was employed, utilizing purpo- sive sampling to select eighty-four (84) food vendors in the vicinity of the University. Data were gathered through metic- ulously designed and self-constructed questionnaires. Descriptive statistical tools, such as frequencies and percentages, were applied for data analysis. The findings indicated that the vendors generally exhibited positive attitudes towards safe food handling, as evidenced by their affirmative responses to practices like handwashing with soap to prevent con- tamination, and thorough washing of utensils used for raw meat before repurposing them for other foods. The vendors' knowledge on food safety was assessed as above average, with an 85% rating. Additionally, the study revealed a high level of awareness and knowledge among the vendors regarding hygienic practices in food vending. Based on these in- sights, it is recommended to intensify educational efforts on food safety practices, particularly targeting the minority who may not adhere to ideal standards. This is crucial as insufficient knowledge can hinder the adoption of appropriate food safety practices.
Keywords
Food Safety, Consumer Knowledge, Attitude, Hygiene Practices.
Background
Street food sales significantly impact the economies of developing countries. Rapid urbanization has led to an increase in eating outside the home, thus elevating the importance of food establishments. The food industry, offering employment and affordable meals, is crucial for economic growth. Despite its importance, concerns about street food's cleanliness, quality, and safety persist, often linked to foodborne illnesses due to vendors' lack of basic food safety knowledge. Research over the years shows street food vendors often lack proper food safety supervision, with issues like unsanitary conditions and poor-quality food being common.
The CDC emphasizes the importance of food hygiene practices in preventing contamination during food preparation and serving. Street food has been identified as a significant source of foodborne illnesses in developing countries, with eating out increasing the risk Food safety, a key scientific discipline, involves practices to maintain food quality and prevent contamination and illness. The WHO reports that millions suffer from food poisoning annually in developing countries due to poor food safety practices [1].
In Malaysia, street food is linked to a high incidence of foodborne illnesses . Studies in Brazil and China reveal poor hygiene and safety awareness among street food vendors. Conversely, over 60% of South African vendors are aware of food safety, while less than half of Ethiopian vendors practice effective food cleanliness. The economic impact of foodborne illnesses in developing countries is substantial .
In Ghana, food handlers' inadequate hygiene practices contribute to the spread of harmful bacteria, affecting public health and leading to significant child mortality. Despite some understanding of food hygiene, there's a gap in connecting poor hygiene to the spread of diseases. The prevalence of foodborne illnesses in African children and the impact on public health, economic productivity, and trade are underscored. The situation analysis emphasizes the need for improved food safety systems in the region to protect consumers, enhance food security, and facilitate international trade opportunities. Furthermore, a specific study conducted in Konongo, Ghana, focused on assessing food hygiene practices among food vendors in educational institutions (10). The study found that while some vendors adhered to good food hygiene practices, there were concerns regarding the capacity of regulatory bodies, the need for training programs for vendors, and the role of educational institutions in ensuring adherence to food hygiene practices. The FAO's five key food safety principles - cleanliness, separating raw and cooked food, thorough preparation, cooking at safe temperatures, and using safe water and materials - are recommended as essential guidelines to address food safety issues in the region. Overall, there is the need for improved food safety systems, training programs for food vendors, and regulatory capacity building to ensure adherence to food hygiene practices and protect public health in Africa, particularly in countries like Ghana. It also emphasizes the importance of aligning with international food safety principles and guidelines to address food safety challenges effectively (FAO,2018; Fellows & Hilmi, 2011; WHO, 2015).
Vendors' knowledge, attitude, and practices significantly impact food safety, with improper practices increasing the risk of foodborne illnesses [2] . Hence, enhancing vendors' practices is crucial for reducing this risk. The reviewed evidence in the study provides insights into the knowledge, attitudes, and practices of street food vendors and consumers regarding food safety in various countries, particularly in Malaysia, South Africa, Ethiopia, and China .The findings reveal a disparity in food safety awareness and practices among street food vendors, with poor hygiene and safety awareness reported in several countries. The study emphasizes the substantial economic impact of foodborne illnesses in developing countries. Moreover, the studies shed light on the need for improved food safety knowledge and attitudes among street food vendors. For instance, the study in China highlights the poor food handling practices and unsanitary conditions of street food vendors, indicating the necessity for enhanced food safety training and improved operating conditions. Similarly, the study in Vietnam identifies factors associated with food safety compliance among street food vendors, emphasizing the significance of education, training, and business capital in promoting better food safety practices. Furthermore, the study in Ethiopia underscores the importance of ongoing training for street food vendors to enhance their food safety practices. The study reveals that factors such as age, income, educational status, vending experience, and food safety training significantly influence food safety practices among street food vendors.
The implications of these findings are significant. It’s underscored the critical need for targeted interventions to improve food safety awareness and practices among street food vendors. This may involve prioritizing vendor training, implementing policies to enhance operating conditions and facilities, and promoting ongoing education and training on food safety practices. Additionally, the study emphasizes the importance of tailored interventions based on specific factors influencing food safety practices, such as education, training, and business capital. Overall, the implications of these studies highlight the urgency of addressing food safety challenges in street food vending, particularly for public institutions in developing countries. By implementing targeted interventions and policies, there is potential to improve food safety practices among street food vendors, ultimately reducing the incidence of foodborne illnesses and promoting public health.
Methodology
This cross-sectional study used a questionnaire-based survey to raise awareness among the population of food vending shops at the University of Cape Coast. This research was carried out in August 2022. The study population included 84 participants who prepare and sell food at Science Market, behind Atlantic Hall, and in the Amamoma and Ayensu community markets. The participants were drawn at random from a population of people over the age of 18. Participants in the study included students, shopkeepers, street vendors, housewives, and others who worked with food in some capacity. Individuals with limited education were asked questions, and their responses were recorded.
The Survey Questionnaire
The questionnaire took about 30 minutes to complete for each respondent. The 40-questionnaire comprised three main categories such as "practise", "attitude" and "food safety knowledge". The demographic section included the respondents' gender, age, occupation, education, and socioeconomic status. Questions based on practice were emphasised to determine standard food handling methods in daily routine. Similarly, attitude questions assessed hygienic approaches. The safety knowledge section assessed awareness of food handling and consumption, which can lead to foodborne diseases.
Data Processing and Analysis
The field data were analysed using a descriptive statistical technique. To ensure quality, the data were coded and analysed using Statistical Package for Service Solution (SPSS) programme version 25. The data was carefully cleaned to remove any outliers or extreme values that could have impacted the validity of the conclusion.
Knowledge, Attitude and Hazard Analysis Critical Control Point (HACCP) Practice Model
To better understand or explain how human behaviour or actions are guided, as well as the relationship between food handlers' knowledge of food safety and practice, several models from the behavioural sciences have been projected [3]. However, the HACCP practice model developed by Ko served as the foundation for this study (2013). This has been noted as a model frequently used to explain the relationship between knowledge, attitude, and practice as shown in figure.1.The model describes the interrelationship between knowledge, attitude, and HACCP practices among food handlers in food service establishments and presupposes that there is a strong relationship between knowledge, attitude, and HACCP practices. The knowledge, attitude, and practice (KAP) model is predicated on the notion that a person's knowledge influences their behaviour or practice and that simply providing information will directly lead to a change in attitude and, subsequently, a behaviour change. Rennie came up with the idea (1995). The model's underlying premise is that practice can be altered and that as one's knowledge grows, so will one's attitude, making one more likely to exhibit the desired behaviour. As a result, an individual's attitudes and practices improve as their level of knowledge increases. It has been noted that the knowledge, attitude, and practise model (KAP) is based on four correlations between the model's key variables, such as knowledge, attitude, and behaviour. The four relationships cited by [4]. There are four different types of relationships: ones in which knowledge and attitude influence each other simultaneously, ones in which knowledge and attitude independently influence behaviour, and ones in which knowledge shared both directly and indirectly influence behaviour. Knowledge can influence attitude but not directly behaviour in these relationships.
In all of the relationships mentioned, attitude was discovered to be a mediating variable between knowledge and behaviour. The food handlers' knowledge, attitudes, and HACCP practices are all related in some way, according to the food safety knowledge, attitude, and practice model. The model shows a strong relationship between HACCP practice and knowledge, attitude, and practice related to food safety. As a result, attitude is now recognised as a critical component in addition to knowledge and practice in reducing the risk of foodborne illnesses. In this way, the attitudes of food handlers toward food safety practices mediate the relationship between knowledge and HACCP practices.
The variables had positive interactions with one another, (Chang et al., 2005)found. The model's assumption that knowledge is the main factor in behavioural change, however, is flawed [5]. Additionally, the model did not consider potential problems or obstructions that might make practice more challenging.
Conceptual Framework
The framework for the study was modified from knowledge, attitude, and HACCP practices (KAP) model after many models were evaluated based on their strengths and weaknesses (see Fig.2). As previously mentioned, the model was changed to make it more appropriate for this study. To narrow the scope of the study, the modification excluded the HACCP practice. As a result, the modified framework focused on food vendors' knowledge of food safety issues, vendors' food safety attitude during food preparation, vendors' hygienic practices during food vending, as well as the conducive environment and economic and social drivers of food safety.
Results and Findings
Demographics Some relevant background data were sought from the respondents. These include data on gender, age, educational level, type of dish, health certificate possession and period for renewal. These results were obtained after the data analysis on this information was summarised in Table 1, and Fig.3 and Fig.4 respectively. The questionnaires were distributed to 23 (27.4%) males and 61 (72.6%) females. Respondents aged 18-25 years represented 48.8%, 18(21.4%) respondents aged 26-33 years, 7(8.3%) people aged 34-41 years, 11(13.1%) people aged 42-49 years, and 7(8.3%) people aged 50 years or older. For the sale of dish category, 35(41.7%) of respondents sell soups, 26(31.0%) sell rice, 10(11.9%) sell porridge, and 13(15.5%) sell fries.
Vendors’ Food Safety Attitude
Table 2 shows the results of an analysis of vendors' food safety attitudes during food preparation. The respondents had positive attitudes toward food preparation. As a consequence, most of the respondents 78(92.9%) agreed with the statement, "I wash my hands with soap to prevent any contamination". Similarly, they stated that "they wash and rinse cutting boards, knives, and plates used for raw meat before using them for other foods" with a frequency of 63(75%) and a strong agreement of 13(15.5%). Cross-contamination could then be said to occur at a very low or never rate. Again, 26 (31.0%) strongly agree and 56 (66.7%) agree that they clean their cooking utensils regularly. Despite this, a small percentage of respondents do not practise the following well. Twelve (12) respondents, or 14.3%, disagree that they ensure that leftovers are stored properly. Twenty (20) people, or 23.8%, said they do not wear head caps/aprons during food preparation, although the majority of 64 (76.2%) said they do. Also, while 12(14.3%) stated that they do not wash their hands with soap and warm water before beginning, 72(86.7%) agreed. When coughing or sneezing, 72(85.7%) agree that they cover their mouth, while 12(14.3%) disagree. When cooking, 19% (21.7%) said they do not remove their jewellery, while the majority (75.4%) said they do. 11 people (13.1%) disagree with the statement "I cover my cut with a bandage and wear gloves." However, the majority of 73 (86.9%) agree, indicating a positive attitude toward food safety. More than half of the respondents demonstrated good knowledge in areas such as the need to wear protective clothing such as aprons/overcoats and gloves while cooking. Food handlers are expected to be well-versed in the use of protective clothing, which acts as a barrier between bare hands and the food being handled(Asli, 2022; Brown, 2021; Fellows & Hilmi, 2011). As a result, respondents' knowledge of the need for these hair restraints exceeds the recommended level. Overall, 75.4% of respondents understood the importance and urgency of wearing hair restraints during food preparation and service, which is a good sign for ensuring food safety. Regarding hand washing and mouth covering when coughing or sneezing, it was discovered to be consistent with the observations made by, that most respondents had a very good attitude on the need to wash hands after visiting the toilet, blowing nose, counting money, and sneezing into handkerchiefs before and during food preparation and service [6]. Their responses regarding the wearing of jewellery during food preparation and service indicate that they agree with the suggestion made by that food handlers should not wear rings and other jewellery during food preparation and service because they can harbour germs that can cause foodborne illness. Wearing jewellery could be a source of foreign matter contamination, potentially introducing bacteria, pathogens and other foreign objects into the food and rendering it unsafe for consumption [7,8].
Food Safety Knowledge
Twelve (12) measurement items were used to evaluate the level of knowledge the food vendors possessed regarding food safety, and the results are shown in Table 3. In total, 85% of the respondents correctly answered the knowledge questions about food safety. This observation demonstrates their familiarity with matters related to food safety. The majority of respondents (95,2%) demonstrated a high level of knowledge concerning the statement that "I know that food can be contaminated with any mistakes I make." As a result, 89.2% of the respondents were aware that kitchen towels and dirty work surfaces are significant sources of cross-contamination and vehicles for contamination. In addition, 63.0% of respondents were aware that a government organisation was keeping an eye on them. The significance of a medical exam as a requirement for employment in the food industry was noted to be known to more than half of the respondents (63%) and other relevant subjects. Their knowledge of medical conditions suggests that a sizable portion of them were aware of the public health requirements requiring everyone working in the food industry to undergo regular checkups and medical examination. The respondent understood that food handlers should not handle food if they are ill or exhibiting symptoms. Furthermore, 25 (29.8%) said they did not remove their jewellery when working with food, while 59 (70.2%) said they did. I keep leftover food in the fridge or freezer for the next day and received 61 (72.6%) 'YES' responses and 23 (27.4% 'NO' responses. I mostly attend food hygiene health education programs, of which 48 (57.1%) are "YES" and 36 (42.9%) are "NO." 72.6 per cent of those polled were aware that leftover food can be refrigerated and that freezing can prevent the growth of some microorganisms in food. This means that a sizable proportion of respondents (27.4%) were unaware that some microorganisms are only inactivated under cold or freezing conditions and will reactivate when conditions improve. Similarly, nearly half (42.9%) of respondents were unaware of the importance of participating in food safety educational programs. Finally, 70(83.3%) responded 'YES' to the statement, my vending point is close to an open gutter, but 14(16.7%) responded 'NO,' as shown in Table 3. Almost all of the respondents are knowledgeable about food safety. As a result, following the KAP model, the respondents were expected to exhibit good food safety practices, given that no one demonstrated low or poor knowledge of food safety issues. The KAP model assumes that an individual's behaviour or practice is determined by his or her knowledge, and that simply providing information to an individual can result in a change in attitudes and practice. As a result, their high knowledge levels may have an impact on their food safety practices.
Hygiene Practice
Statistical analysis was performed on data to ascertain respondents' knowledge of food vending hygiene, 11 vendor hygiene practices during food sales have been applied. The distribution of scores with the hygienic procedures used by vendors when selling food is shown in Table 4. The current general consensus is that 97.6% of the respondents agreed with the statements about the hygiene practices of vendors during food vending, demonstrating their familiarity with these issues. This assumption is valid since majority of them had practical knowledge of always washing dishes/bowls in clean, soapy water 78 (92.9%), avoid using bare hands when serving food 76(90.5%), and the need to empty trash cans regularly 77(92.7%). It is important to understand that the consequences of proper waste disposal prevent the spread of insects and pests in the environment. These results further the understanding of the ISO 22000 (2015) standard, which requires that waste containers have appropriate lids and that liquid and solid waste be removed from food processing areas without contaminating their surroundings or their products.
The vast majority of respondents (90%) included in the study were aware that clearing the dining table as soon as a customer finished eating prevented flies and other insects from primarily invading the vending area to cause contamination. Unclean work surfaces and kitchen towels are major sources of cross-contamination and vehicles for contamination, according to this affirmation [9]. 75 of them, or 89.3%, strongly agreed that sweeping or cleaning the vending area properly more than twice a day lowers the risk of food contamination. Additionally, relatively large statistical differences, 67 (79.8%) agreed that customers should frequently have new hand-washing water available. Likewise, about 76 (90.5%) people agreed that cooked foods should be served extremely hot and that people shouldn't handle food with their bare hands to prevent contamination.
Conclusion
Food vendors at the University of Cape Coast and its environs were observed to exhibit a positive food safety attitude during food preparation, as evidenced in a study conducted by Adjei and Adjei (2022). The vendors were found to possess a good understanding of food safety principles and consider hygiene practices when handling and preparing food. However, it was noted that the relationship between the food vendors’ food safety knowledge and attitude did not consistently translate into their practices, indicating that food safety knowledge does not always align with appropriate attitudes and practices. Moreover, the study revealed that while the majority of vendors (75%) held health certificates, a significant proportion (31%) had not renewed their licenses. This raises concerns about the potential impact on food hygiene practices, suggesting that unsafe practices may persist due to the lack of license renewal and oversight .
Abbreviations
(KAP) Knowledge, Attitude, and Practice Model
(HACCP) Hazard Analysis Critical Control Point
Acknowledgement
We express our gratitude to the authors and food vendors in the University of Cape Coast community for generously providing their resources. Additionally, we acknowledge the valuable contributions of the reviewers and editors who supported our work.
Author Contributions
KE conceived the idea of the study. KE, SOD, FA and EAA analysed the data. All authors (KE,SOD,FA,EAA) wrote the manuscript. All authors read, edited, and approved the final version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Availability of Data and Materials
All resources used in this study are available, and the authors will make them available according to their respective copyright and access policies.
Ethics Approval and Consent to Participate
The project adheres to ethical standards set by national and institutional human experimentation committees as well as the 1975 Declaration of Helsinki, amended in 2008. Access and use of resources were conducted ethically and in accordance with project implementation standards. Ethical approval was obtained from the University of Cape Coast Institutional Review Board, and informed consent was secured from the managers who provided interview data.
Consent for Publication
Not applicable.
Competing Interest
The authors declare no competing interests.
|
Variable |
Sub-Scale |
Frequency |
Percentage |
|
Gender |
Male |
23 |
27.4 |
|
Female |
61 |
72.6 |
|
|
Age |
18 - 25 years |
41 |
48.8 |
|
26 – 33 years |
18 |
21.4 |
|
|
34 – 41 years |
7 |
8.3 |
|
|
42 - 49 years |
11 |
13.1 |
|
|
50 and above |
7 |
8.3 |
|
|
Educational Level |
Primary |
35 |
41.7 |
|
Secondary |
39 |
46.4 |
|
|
Tertiary |
10 |
11.9 |
|
|
Type of dish |
Soup dish |
35 |
41.7 |
|
Rice dish |
26 |
31.0 |
|
|
Porridge dish |
10 |
11.9 |
|
|
Fries |
13 |
15.5 |
Table 1: Background information of the respondents
|
|
Statement |
Strongly Disagree F(%) |
Disagree
F(%) |
Agree
F(%) |
Strongly Agree F(%) |
|
1. |
I wash my hands with soap to prevent any contamination |
2(2.4) |
4(4.9) |
67(79.8) |
11(13.1) |
|
2. |
I wash and rinse cutting boards, knives and plates used for raw meat before using them for other foods. |
1(1.2) |
7(8.3) |
63(75) |
13(15.5) |
|
3. |
I clean the cooking utensils regularly |
2(2.4) |
0(0) |
56(66.7) |
26(31.0) |
|
4. |
I ensure that leftovers are preserved in an appropriate place |
0(0) |
12(14.3) |
43(51.2) |
29(34.5) |
|
5. |
I wear head caps /apron |
9(10.7) |
11(13.1) |
43(51.2) |
21(25.0) |
|
6. |
I try to maintain short and clean nails |
1(1.2) |
13(15.5) |
54(64.3) |
16(19.0) |
|
7. |
I try to clean the work area and surfaces frequently |
0(0) |
6(7.1) |
57(67.9) |
21(25.0) |
|
8. |
I remove my jewellery |
4(4.8) |
15(17.9) |
29(34.5) |
36(42.9) |
|
14. |
I cover my mouth when coughing or sneezing |
2(2.4) |
10(11.9) |
60(71.4) |
12(14.3) |
|
15. |
I wash my vegetables with salty water before using |
3(3.6) |
11(13.1) |
46(54.8) |
24(28.6) |
|
16. |
Hands washing with soap and warm water before commencing |
10(11.9) |
28(33.3) |
35(41.7) |
11(13.1) |
|
17. |
I wash my hands only after |
18(21.4) |
32(38.1) |
26(31.0) |
8(9.5) |
|
18. |
I cover my cut with a bandage and use gloves |
3(3.6) |
8(9.5) |
58(69.0) |
15(17.9) |
Table 2: Vendors' Food Safety Attitudes During Food Preparation
|
|
Statements |
YES F(%) |
NO F(%) |
|
1. |
I remove my jewellery when dealing with food |
59(70.2) |
25(29.8) |
|
2. |
I know that food can be contaminated with any fewer mistakes I make. |
80(95.2) |
4(4.8) |
|
3. |
I store leftover foods in the refrigerator/freezer to be used the next day |
61(72.6) |
23(27.4) |
|
4. |
I pour leftover foods into a container and cover it to be used the next day |
54(64.2) |
30(35.7) |
|
5. |
I Pour leftover foods into a container and leave it open to be used the next day |
11(13.1) |
73(86.9) |
|
6. |
I have undergone a medical examination for purposes of food vending |
63(75.0) |
21(25.0) |
|
7. |
I mostly attend health education programs on food hygiene |
48(57.1) |
36(42.9) |
|
8. |
My activities are being monitored by the government agency |
63(75.0) |
21(25.0) |
|
10. |
The person(s) preparing the food has formal training in food preparation and handling |
50(59.5) |
32(38.1) |
|
11. |
My vending point is close to an open gutter |
14(16.7) |
70(83.3) |
|
12. |
Food preparation surfaces can contaminate foods |
75(89.2) |
9(10.7) |
Table 3: Vendors' Level of Food Safety Knowledge
|
|
Statement |
Strongly Disagree F(%) |
Disagree
F(%) |
Agree
F(%) |
Strongly Agree F(%) |
|
1. |
I always wash dishes/ bowls in clean soapy water |
2(2.4) |
4(4.8) |
53(63.1) |
25(29.8) |
|
2. |
I serve food with my bare hands |
2(2.4) |
6(7.1) |
35(41.7) |
41(48.8) |
|
3. |
I collect money with bare hands and never wash my hands before touching the food again |
0(0.0) |
2(2.4) |
57(67.9) |
25(29.8) |
|
4. |
I cover my cut with a bandage when serving food |
14(15.7) |
17(20.2) |
43(51.2) |
10(11.9) |
|
5. |
I cover my head with a cap/ scarf when serving |
17(20.2) |
14(16.7) |
33(39.3) |
20(23.8) |
|
6. |
I often change hands and wash water for customers |
0(0.0) |
17(20.2) |
45(53.6) |
22(26.2) |
|
7. |
I make sure my food is always warm |
19(22.6) |
18(21.4) |
22(26.2) |
25(29.8) |
|
8. |
I make sure my packaging materials are always clean |
4(4.4) |
4(4.8) |
58(69.0) |
18(21.4) |
|
9. |
I clear the eating table immediately customer finishes eating |
2(2.4) |
6(7.1) |
35(41.7) |
41(48.8) |
|
10. |
I sweep my vending area more than twice a day |
2(2.4) |
7(8.3) |
42(50.0) |
33(39.3) |
|
11 |
I empty and clean my dustbin always |
0(0.0) |
6(7.2) |
46(55.4) |
31(37.3) |
Table 4: The Vendors' Hygiene Practices During Food Vending
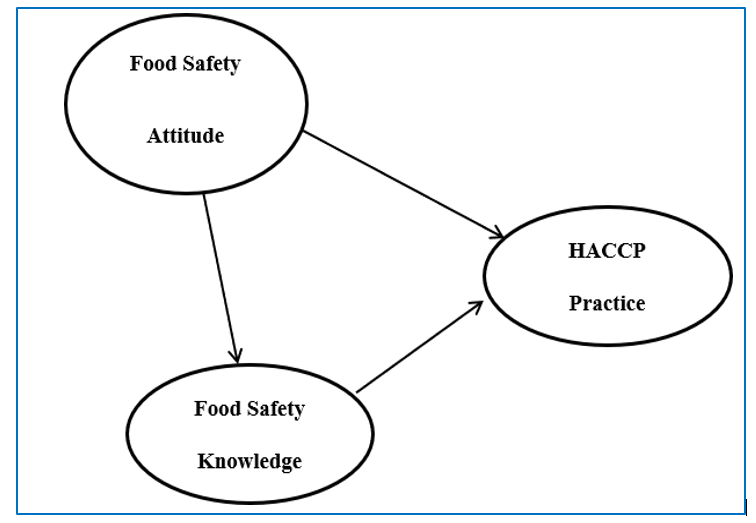
Figure 1: Model of Food Safety Knowledge, Attitude and HACCP Practice
Source: (Ko, 2013)
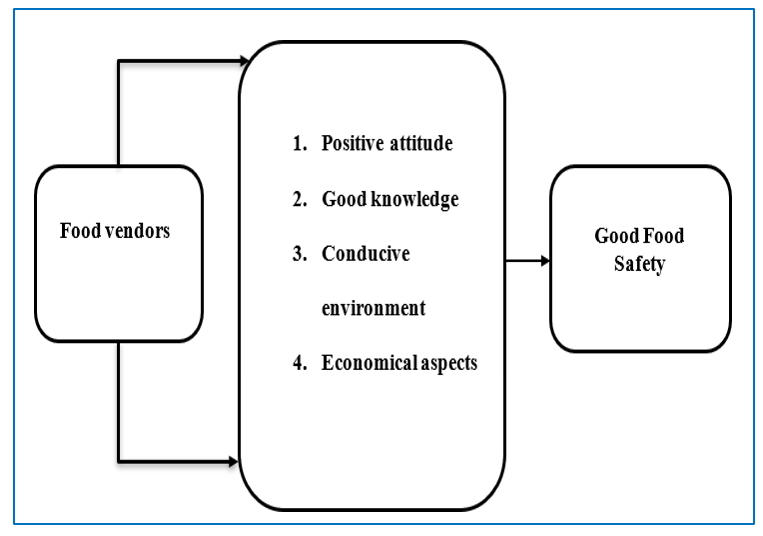
Figure 2: The diagram above depicts the study's conceptual framework
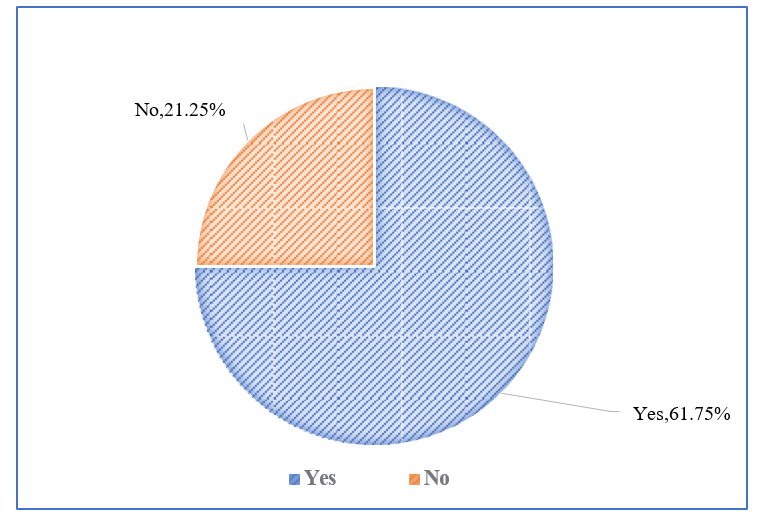
Figure 3: Do you have health certificate?
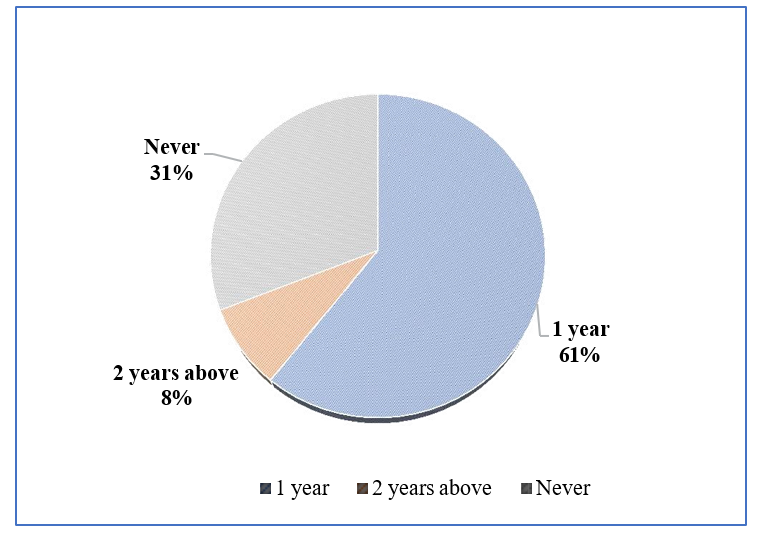
Figure 4: How often do you renew it?
References
- World Health Organization. (2015). WHO estimates of the global burden of foodborne diseases: foodborne disease burden epidemiology reference group 2007-2015. World Health Organization.
- Sharif, L., Obaidat, M. M., & Al-Dalalah, M. R. (2013).Food hygiene knowledge, attitudes and practices of the food handlers in the military hospitals. Food and Nutrition Sciences, 4(03), 245.
- Rennie, D. M. (1995). Health education models and food hygiene education. Journal of the Royal Society of Health, 115(2), 75-79.
- Schwartz, S. (1975). Individual differences in cognition: Some relationships between personality and memory. Journal of Research in Personality, 9(3), 217-225.
- Ehiri, J. E., G. P. Morris, and J. McEwen (1997). "Evaluation of a food hygiene training course in Scotland." Food Control8.3: 137-147.
- Ackah, M., Gyamfi, E. T., Anim, A. K., Osei, J., Hansen, J. K., & Agyemang, O. (2011). Internet Journal of Food Safety. Internet Journal of Food Safety, 13, 191-197.
- Abdullah, S. A. B. (2015). Knowledge, Attitudes and Practices (KAP) of Food Handlers at Ras Al-Khaimah Poultry Company Slaughterhouse RAK, UAE (2015) (Doctoral dissertation, University of Gezira).
- Qoura, O., & Ali, E. L. (2016). The effects of food safety knowledge, attitude and ractices on hotel competitive advantages: Perceptions of food service staff in hotels. Journal of Association of Arab Universities for Tourism and Hospitality, 13(4), 44-62.
- Mba-Jonas, A., Culpepper, W., Hill, T., Cantu, V., Loera, J., Borders, J., ... & Neil, K. P. (2018). A multistate outbreak of human Salmonella Agona infections associated with consumption of fresh, whole papayas imported from Mexico—United States, 2011. Clinical Infectious Diseases, 66(11), 1756-1761.
- Apanga, S., Addah, J., & Sey, D. R. (2014). Food safety knowledge and practice of street food vendors in rural northern Ghana.
- Arvanitoyannis, I. S. (2009). HACCP and ISO 22000: Application to foods of animal origin. John Wiley & Sons.
- Asli, K. (2022). Food safety knowledge, beliefs and behaviour among health sciences-related field undergraduate students at a local university. Jurnal Sains Kesihatan Malaysia, 20(2), 13-21.
- Brown, L. (2021). Using data to improve practice: Looking back on 20 years of restaurant food safety research. Journal of environmental health, 83(7), 40-43.
- Chang, J. M., Chen, T. H., & Fang, T. J. (2005). Pesticide residue monitoring in marketed fresh vegetables and fruits in central Taiwan (1999-2004) and an introduction to the HACCP system. Journal of Food and Drug Analysis, 13(4), 5.
- Fellows, P., & Hilmi, M. (2011). Selling street and snackfoods.
- Ifeadike, C. O., Ironkwe, O. C., Adogu, P. O., & Nnebue, C.C. (2014). Assessment of the food hygiene practices of food handlers in the Federal Capital "federal capital territory". Tropical journal of medical research, 17(1), 10.
- Ko, W. H. (2013). The relationship among food safety knowledge, attitudes and self-reported HACCP practices in restaurant employees. Food control, 29(1), 192-197.
- Mapelu, I. C., & Onyango, D. (2018). The Role of personal and premises hygiene in the assuage of food safety in selected hotels within Eldoret town.